what is cholecystokinin
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Now I have everything needed for a thorough, well-cited answer.
Cholecystokinin (CCK)
CCK is a peptide hormone produced primarily by I cells in the mucosa of the duodenum and upper jejunum. Its name literally means "bile sac mover" - chole (bile) + cysto (sac) + kinin (move) - reflecting its first known action of contracting the gallbladder.
Structure
- Originally identified as a 33-amino acid peptide, but multiple forms exist: CCK-58, CCK-33, CCK-22, CCK-8, and CCK-7, all derived from a single gene via post-translational processing of a preprohormone.
- The minimum active fragment is the C-terminal heptapeptide (CCK-7).
- CCK shares the same C-terminal five amino acids as gastrin, which is why CCK has mild gastrin-like activity.
- The tyrosine at position 7 from the C-terminal is sulfated - a structural feature unique to CCK (unlike gastrin, which has a non-sulfated form).
(Costanzo Physiology 7th Ed.; Ganong's Review of Medical Physiology 26th Ed.)
Stimuli for Release
CCK is released in response to:
- Fats - monoglycerides and fatty acids (long-chain, >10 carbons); NOT intact triglycerides
- Proteins - small peptides, amino acids, proteoses, and peptones (partial protein digestion products)
- CCK-releasing peptide (from intestinal mucosa) and monitor peptide (from pancreas) - these trigger a short-lived positive feedback loop; the loop terminates once proteolytic enzymes degrade these peptides
(Sleisenger & Fordtran's GI and Liver Disease; Ganong's 26th Ed.)
Actions (Five Major Effects)
| Action | Mechanism/Result |
|---|---|
| Gallbladder contraction | Contracts GB + relaxes sphincter of Oddi → bile flows into duodenum for fat emulsification |
| Pancreatic enzyme secretion | Stimulates acinar cells to secrete lipases, amylase, proteases; accounts for 70-80% of post-meal pancreatic enzyme output |
| Inhibition of gastric emptying | Slows delivery of chyme from stomach → allows adequate time for digestion and absorption |
| Pancreatic HCO3- secretion | Minor direct effect, but potentiates the action of secretin |
| Trophic effects | Promotes growth of the exocrine pancreas and gallbladder |
Additionally, CCK inhibits gastric acid secretion by binding to CCK-1 receptors on somatostatin (D) cells in the gastric mucosa → somatostatin is released → suppresses gastrin from G cells and directly inhibits parietal cells.
(Costanzo Physiology 7th Ed.; Guyton & Hall Medical Physiology; Sleisenger & Fordtran's)
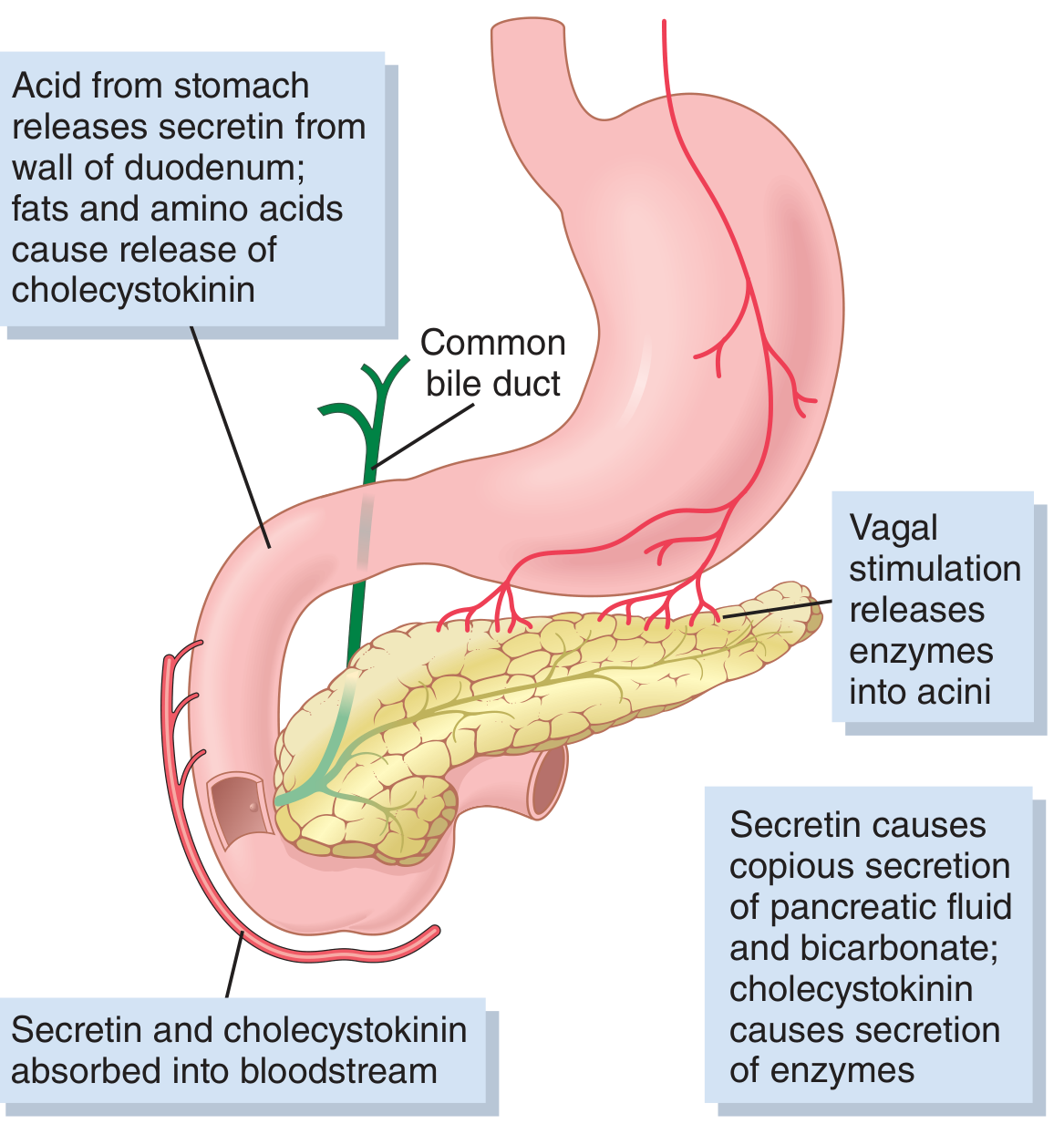
Regulation diagram (from Guyton & Hall):
Receptors
Two receptor subtypes:
- CCK-A (CCK-1) receptors - selective for CCK; primarily peripheral (gallbladder, pancreas, vagal afferents, gastric smooth muscle). Signal via PLC → intracellular Ca2+.
- CCK-B (CCK-2 / gastrin) receptors - equally sensitive to both CCK and gastrin; found throughout the brain (cerebral cortex) and gut. Also signal via PLC → Ca2+.
(Ganong's Review of Medical Physiology 26th Ed.)
CCK in the Brain and Nervous System
CCK is not just a gut hormone - it is also a neuropeptide:
- Found in neurons of the cerebral cortex, distal ileum, colon, and peripheral nerves.
- Acts as a satiety signal in the hypothalamus, particularly via the nucleus of the solitary tract (NTS) through vagal afferents.
- May be co-released with GABA in some neurons.
(Neuroscience: Exploring the Brain 5th Ed.; Ganong's)
Half-life and Metabolism
The half-life of circulating CCK is approximately 5 minutes. Details of its full metabolic pathway are not well characterized.
Clinical Relevance
| Condition | CCK Change | Explanation |
|---|---|---|
| Celiac disease | Low CCK | Reduced intestinal mucosal surface area → less I cell stimulation |
| Bulimia nervosa | Low CCK | Abnormal feedback; contributes to reduced satiety |
| Chronic pancreatitis | High CCK | Reduced pancreatic enzyme output → loss of negative feedback on CCK release |
| No disease of CCK excess is recognized | - | - |
Diagnostic/therapeutic use:
- CCK + secretin stimulation test: evaluates pancreatic exocrine function
- CCK used radiographically or scintigraphically to assess gallbladder contractility (e.g., CCK-HIDA scan)
(Sleisenger & Fordtran's GI and Liver Disease)
In summary, CCK is a multi-functional gut-brain peptide hormone that coordinates the digestion and absorption of fats and proteins by simultaneously mobilizing bile (gallbladder contraction), unleashing digestive enzymes (pancreatic secretion), and slowing gastric emptying - while also telling the brain to stop eating (satiety).
Where it releases from
Based on what was already covered in the previous answer, here is a focused summary:
Where CCK is Released From
Primary Source - The Gut
CCK is released from I cells (also called "cholecystokinin cells"), which are enteroendocrine cells located in the mucosa of the:
- Duodenum (the first part of the small intestine) - highest concentration
- Jejunum (upper part) - significant source
- Sparse presence further down the small intestine
Once released, CCK enters the bloodstream and travels to its target organs (gallbladder, pancreas, stomach).
(Costanzo Physiology 7th Ed.; Guyton & Hall Medical Physiology; Ganong's Review of Medical Physiology 26th Ed.)
Secondary Sources - The Nervous System
CCK is also produced and released from neurons in:
| Location | Role |
|---|---|
| Cerebral cortex | Neurotransmitter / neuromodulator |
| Distal ileum and colon | Enteric nervous system signaling |
| Peripheral nerves throughout the body | Local signaling |
| Hypothalamus / NTS | Satiety regulation |
Simple Summary
CCK comes primarily from I cells of the duodenum and upper jejunum into the blood, and secondarily from neurons in the brain and gut wall.
The gut I cells are what matter for the classic digestive actions (gallbladder contraction, pancreatic enzyme secretion, slowing gastric emptying). The brain neurons are what mediate the feeling of fullness after a meal.
What is porta hepatitis
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
I have comprehensive information from multiple surgical and anatomical textbooks. Here is the full answer:
Porta Hepatis
The porta hepatis (Latin: "gateway of the liver") is the hilum of the liver - a deep transverse fissure on the visceral (inferior) surface of the liver through which all major neurovascular structures and bile ducts enter or exit. It is a purely anatomical landmark, not a disease.
Location
- Found on the posterior part of the inferior (visceral) surface of the liver
- Lies between the caudate lobe (posteriorly) and the quadrate lobe (anteriorly)
- The hepatoduodenal ligament (the free edge of the lesser omentum) connects the porta hepatis to the first part of the duodenum and encloses all structures passing through it
(Gray's Anatomy for Students; Fischer's Mastery of Surgery 8th Ed.)
Contents - "The Portal Triad"
Three main structures pass through the porta hepatis, arranged in a consistent pattern within the hepatoduodenal ligament:
| Structure | Position | Direction |
|---|---|---|
| Portal vein | Posterior | Enters liver |
| Proper hepatic artery | Left lateral (anterior to portal vein) | Enters liver - divides into left and right branches at the porta hepatis |
| Common hepatic duct | Right lateral (anterior to portal vein) | Exits liver |
Additionally:
- Lymphatic vessels - enter and leave
- Hepatic nerve plexus (sympathetic and parasympathetic fibers) - enters
- Lymph nodes - present at the hilum (hepatic hilar lymph nodes)
Memory tip: "Portal vein is Posterior; artery is left; bile duct is right" - Bill (bile duct) is on the Right, Art (artery) is on the Left, Portal vein is behind them all.
(Fischer's Mastery of Surgery 8th Ed.; Mulholland & Greenfield's Surgery 7th Ed.)
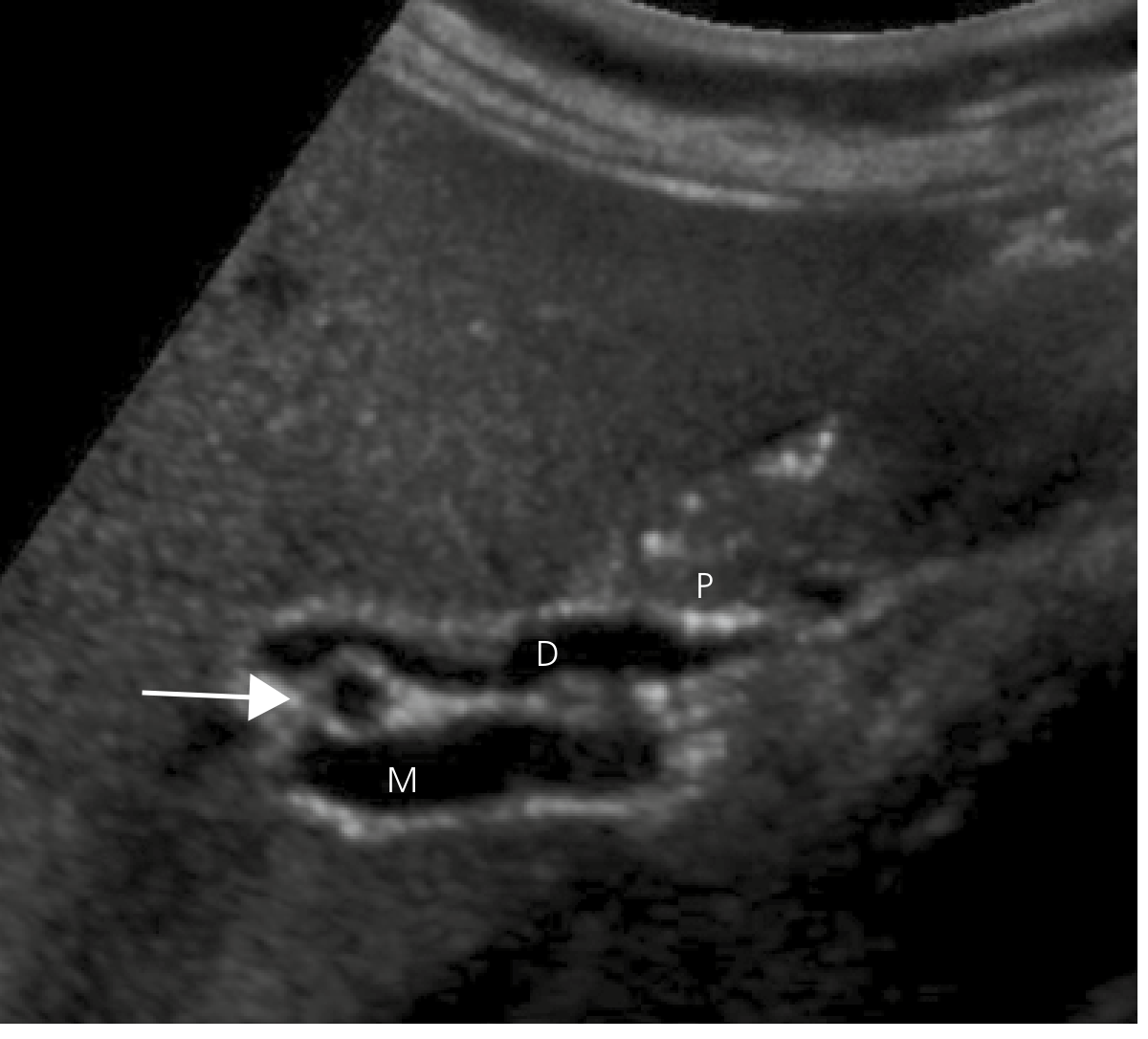
Ultrasound appearance of the porta hepatis
The image below (from Yamada's Textbook of Gastroenterology) shows the porta hepatis on ultrasound - the common bile duct (D) is seen anterior to the main portal vein (M), with the portal vein running posterior:
Surgical Anatomy and the Plate System
The porta hepatis is surrounded by a fibrous sheath continuous with Glisson's capsule. Three anatomical "plates" are defined here:
- Hilar plate - bounded superiorly by segment 4 of the liver, and on right and left by the cystic and umbilical plates
- Cystic plate - in the gallbladder fossa
- Umbilical plate - along the umbilical fissure anteriorly
"Lowering the hilar plate" is a key surgical technique used in liver resections to expose individual vascular and biliary structures.
(Fischer's Mastery of Surgery 8th Ed.)
Pringle Maneuver
Because the portal triad (portal vein + hepatic artery + bile duct) all pass through the porta hepatis together, surgeons can temporarily compress this region between the finger and thumb (through the foramen of Winslow / epiploic foramen) to control bleeding from the liver. This is called the Pringle maneuver.
Clinical Relevance
| Condition | Relevance to Porta Hepatis |
|---|---|
| Cholangiocarcinoma (Klatskin tumor) | Tumor at the confluence of right and left hepatic ducts at the porta hepatis - most common site |
| Biliary atresia | Fibrous obliteration of bile ducts at the porta hepatis; treated with Kasai portoenterostomy (Roux-en-Y anastomosis to the porta hepatis) |
| Porta hepatis lymphadenopathy | Can compress bile duct causing obstructive jaundice; seen in lymphoma, metastatic disease, TB |
| Trauma to porta hepatis | Rare but highly lethal (51% overall mortality); injuries to portal vein have up to 90% mortality with ligation |
| Hepatocellular carcinoma | Portal vein tumor thrombus may extend to the porta hepatis |
(Current Surgical Therapy 14th Ed.; Sleisenger & Fordtran's GI and Liver Disease)
In short: The porta hepatis is the liver's "gateway" - a transverse fissure on the under-surface of the liver where the portal vein and hepatic artery enter, and the hepatic bile duct exits. All three travel together within the hepatoduodenal ligament. It is one of the most important surgical landmarks in abdominal surgery.
Superiorily the neck of the gallbladder is attached to the liver by areolar tissue in which cystic vessels are embedded.. tell me why there is arolar tissue there and what is the importance of cystic vessels
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Excellent - comprehensive information gathered. Here is a detailed, well-cited answer.
Why Areolar Tissue and Why Cystic Vessels Matter at the Gallbladder Neck
Part 1 - Why There is Areolar Tissue Here
What is areolar tissue?
Areolar (loose connective) tissue is a type of connective tissue made of loosely arranged collagen and elastic fibers, with fibroblasts, macrophages, and a gel-like ground substance. It is the body's "packing material."
Why does it sit between the gallbladder neck and the liver?
1. The gallbladder is NOT fused to the liver - it sits in a "bed"
The gallbladder lies in a fossa on the inferior surface of the liver (between segments IV and V), attached to it via the cystic plate - a fibrous sheet continuous with Glisson's capsule. Between the gallbladder's muscular wall (muscularis) and the cystic plate, there is a thin layer of areolar tissue that progressively thickens from the top of the gallbladder downward. This loose tissue:
- Allows slight mobility of the gallbladder as it fills and empties, and with respiratory movements
- Acts as a connective tissue scaffold through which vessels, nerves, and lymphatics can travel to reach the gallbladder wall
- Provides a natural surgical plane - during cholecystectomy, the gallbladder is dissected from the liver by working through this areolar tissue layer
(Fischer's Mastery of Surgery 8th Ed.)
2. The cystic plate beneath it is not just passive
The cystic plate contains small bile ducts (Ducts of Luschka) - accessory bile ducts less than 1 mm in diameter that pass through the plate from the liver parenchyma into the gallbladder. The areolar tissue "bridge" between the gallbladder and liver accommodates these tiny communicating structures. If dissection goes too deep (into or beyond the cystic plate), the right portal pedicle can be breached, injuring the right hepatic duct or artery.
(Fischer's Mastery of Surgery 8th Ed.)
3. Developmental reason
Embryologically, the gallbladder develops as an outgrowth of the hepatic diverticulum and migrates to its bed in the liver. The areolar tissue represents the residual loose mesenchymal connection from this developmental attachment - it is never a true peritoneal reflection superiorly (unlike the free inferior surface, which is peritonealized).
Part 2 - The Cystic Vessels and Their Importance
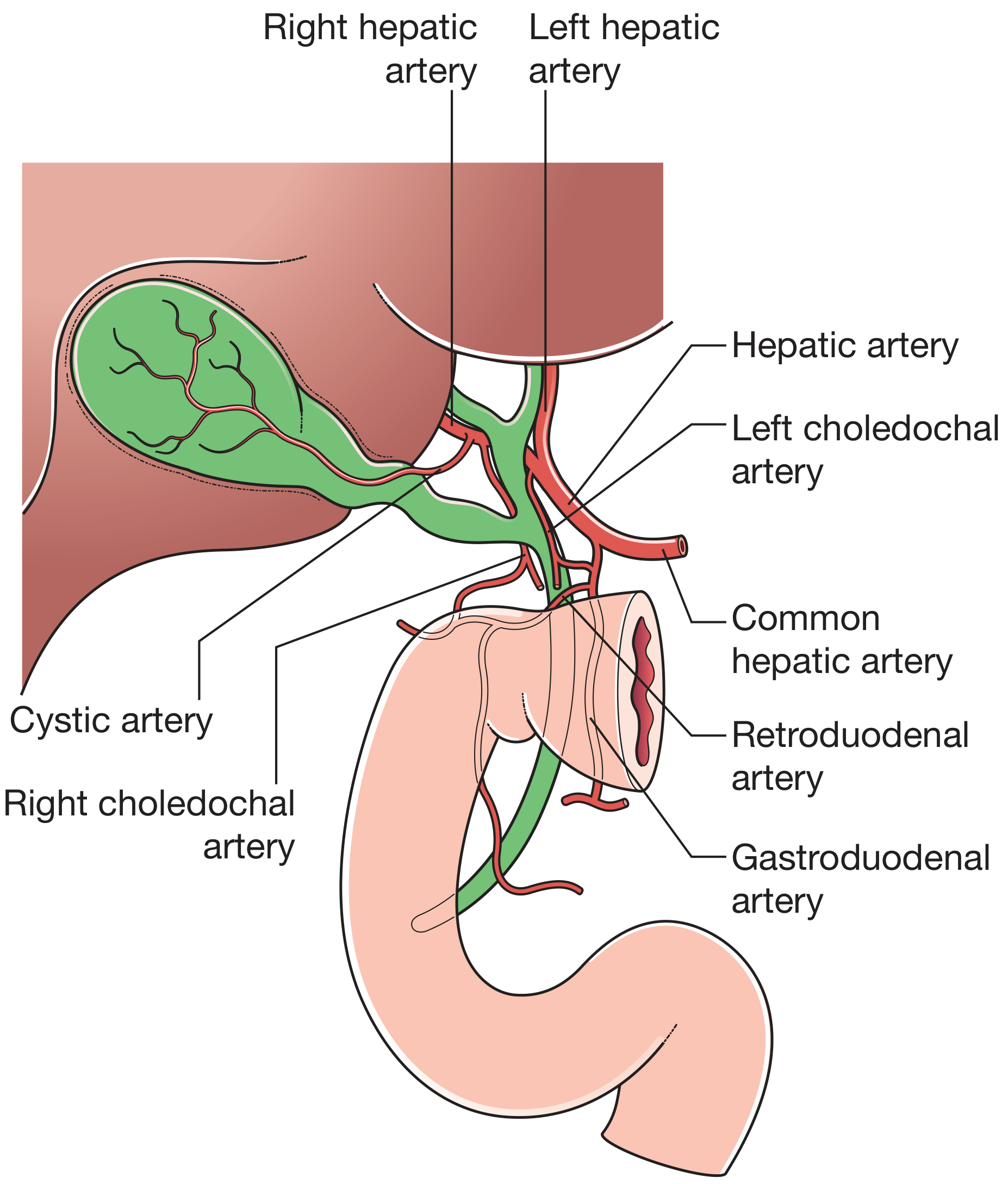
A. The Cystic Artery
| Feature | Detail |
|---|---|
| Origin | Usually from the right hepatic artery (most common, ~75%) |
| Other origins | Left hepatic artery, common hepatic artery, gastroduodenal artery, superior mesenteric artery (highly variable) |
| Course | Runs through the triangle of Calot (hepatocystic triangle) to reach the gallbladder neck |
| Division | Bifurcates into anterior and posterior branches at the neck of the gallbladder |
Why it matters:
-
Sole blood supply - The cystic artery is the gallbladder's only dedicated arterial supply. Compromise of this artery (e.g., in acute cholecystitis with thrombosis) leads to gallbladder wall ischemia and gangrene - a surgical emergency.
-
Surgical danger - Since the cystic artery is embedded in the areolar tissue at the neck and runs close to the right hepatic artery, it is at high risk during cholecystectomy. In severe inflammation or fibrosis, the right hepatic artery can form an "inverse U-loop" (caterpillar turn), becoming adherent to the gallbladder and mimicking the cystic artery. Mistaking the right hepatic artery for the cystic artery and ligating it is one of the most catastrophic complications of cholecystectomy.
-
Short cystic artery variant - In 5-10% of cases, the cystic artery does not arise from the right hepatic artery until just before it enters the liver, creating a very short cystic artery. Failure to recognize this can lead to inadvertent ligation of the right hepatic artery.
(Yamada's Textbook of Gastroenterology 7th Ed.; Current Surgical Therapy 14th Ed.)
B. The Cystic Veins
The venous drainage of the gallbladder is unique - there is no single dominant cystic vein in most people. Instead:
- Multiple small veins run from the hepatic surface of the gallbladder directly into the liver parenchyma through the cystic plate (draining ultimately into the middle hepatic vein)
- Some veins run toward the cystic duct and join venous collaterals from the common bile duct, then drain into the portal vein (right portal vein specifically)
- In a minority of patients, a single larger cystic vein exists and drains back to the portal vein directly
(Yamada's Textbook of Gastroenterology 7th Ed.; Schwartz's Principles of Surgery 11th Ed.)
Why the venous drainage matters:
-
Direct liver drainage = cancer spread route - Because cystic veins drain directly into hepatic parenchyma (segments IV and V), gallbladder cancer spreads directly into adjacent liver very early. This is why even T1b/T2 gallbladder cancer requires resection of segments IVb and V along with the gallbladder.
-
Bleeding during cholecystectomy - The small veins embedded in the areolar tissue between the gallbladder and cystic plate are a source of troublesome oozing during dissection. Surgeons must be careful here, especially when the tissue is inflamed.
-
Portosystemic anatomy - The cystic vein draining into the right portal vein is part of the normal portal circulation. In portal hypertension, these veins can enlarge as portosystemic collaterals.
(Sleisenger & Fordtran's GI and Liver Disease; Current Surgical Therapy 14th Ed.)
Summary Table
| Structure | Location | Why Important |
|---|---|---|
| Areolar tissue | Between gallbladder muscularis and cystic plate | Allows mobility, transmits vessels/nerves, surgical dissection plane, contains Ducts of Luschka |
| Cystic artery | In areolar tissue / triangle of Calot | Only arterial supply to GB; highly variable; at risk during cholecystectomy |
| Cystic veins | Areolar tissue over hepatic surface | Direct liver drainage (cancer spread); bleeding source; portal drainage |
The clinical bottom line: this small region of areolar tissue at the gallbladder neck is one of the most surgically treacherous areas in the abdomen. Understanding it precisely is essential for safe cholecystectomy and for understanding how gallbladder disease spreads.
What is the importance of hartmanns pouch
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Excellent coverage from multiple major surgical textbooks. Here is the complete answer:
Hartmann's Pouch - Definition and Importance
What is it?
Hartmann's pouch is an asymmetric outpouching (diverticulum) on the inferior surface of the infundibulum of the gallbladder - the transitional zone between the gallbladder body and neck. It is not always present in normal anatomy; it represents either a natural anatomical variant or, more often, an acquired bulge caused by repeated stone impaction and stretching of the wall.
"Frequently, an asymmetric bulging of the right side of the neck may occur. This bulge, known as the infundibulum (or Hartmann's pouch)..."
- Fischer's Mastery of Surgery 8th Ed.
Its anatomical relations are important: it lies immediately superior to the duodenum, and may be tethered to the first part of the duodenum by the cholecystoduodenal ligament (right edge of the lesser omentum).
Importance of Hartmann's Pouch
1. Most Common Site of Gallstone Impaction
Gallstones preferentially lodge in Hartmann's pouch due to its dependent, bulging anatomy. When a stone gets stuck here, it obstructs the cystic duct outlet - the consequence is acute cholecystitis.
"In approximately 90% of cases, the underlying cause [of acute cholecystitis] is obstruction of the outlet of the gallbladder by a gallstone in the cystic duct, gallbladder neck, or Hartmann's pouch."
- Sleisenger & Fordtran's GI and Liver Disease
2. Mirizzi Syndrome
This is the most clinically significant consequence of Hartmann's pouch pathology. When a large stone becomes impacted in Hartmann's pouch (or the cystic duct), it can compress the adjacent common hepatic duct, causing obstructive jaundice.
Classification:
| Type | Description |
|---|---|
| Type I | Stone in Hartmann's pouch compresses but does not erode into the common hepatic duct - external compression only |
| Type II | Stone erodes through the wall into the common hepatic duct - cholecystocholedochal fistula; <1/3 of bile duct involved |
| Type III | Fistula with 1/3 to 2/3 of bile duct wall involvement |
| Type IV | Fistula with >2/3 of bile duct wall involved - requires Roux-en-Y hepaticojejunostomy |
Clinical presentation: repeated bouts of pain, fever, and jaundice - can mimic a Klatskin (hilar cholangiocarcinoma) tumor on imaging.
Incidence: ~1% of all patients undergoing cholecystectomy.
(Sleisenger & Fordtran's; Goldman-Cecil Medicine)
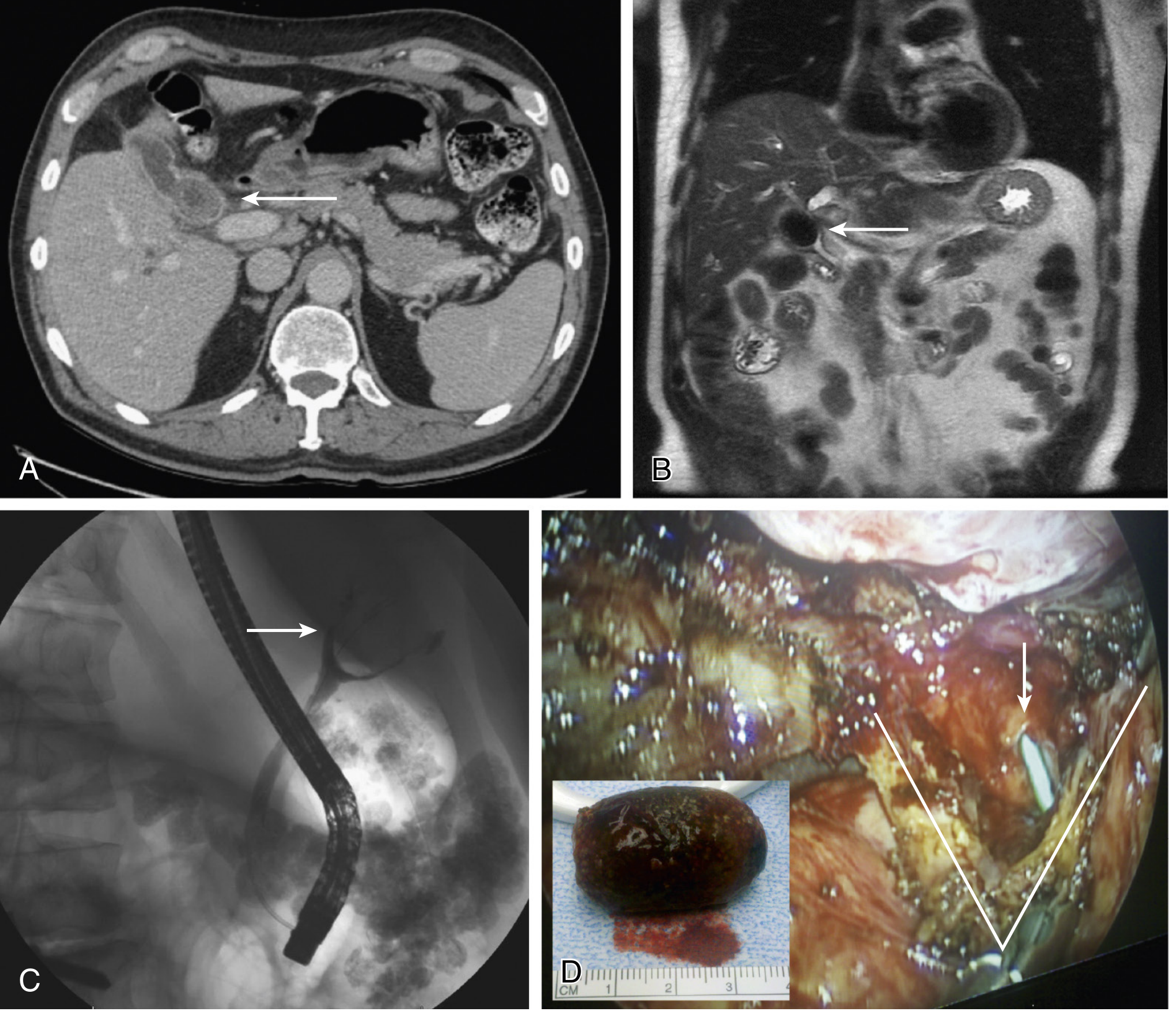
The imaging below shows Type III Mirizzi syndrome with a large gallstone impacted in the infundibulum (Hartmann's pouch) compressing and fistulating into the common hepatic duct:
3. Surgical Hazard During Cholecystectomy
Hartmann's pouch is a major source of danger during cholecystectomy for two reasons:
a) Obscures the cystic duct junction:
The pouch can hang down and hide the exact point where the cystic duct begins. The surgeon must divide the cholecystoduodenal ligament and mobilize Hartmann's pouch before the cystic duct can be clearly identified and safely clipped. Failing to do this is a known cause of bile duct injury.
b) Tethering to duodenum:
Because Hartmann's pouch lies immediately above the duodenum and may be adherent to it, vigorous traction during cholecystectomy risks tearing the duodenum.
(Fischer's Mastery of Surgery 8th Ed.)
4. Role in Subtotal Cholecystectomy
In cases of severe inflammation (e.g., gangrenous cholecystitis, Mirizzi syndrome), when total cholecystectomy is too dangerous, surgeons perform a subtotal cholecystectomy - the fundus and body are excised, leaving Hartmann's pouch intact near the cystic duct to avoid damaging the bile duct. Hartmann's pouch thus becomes the landmark defining how much gallbladder to leave behind safely.
(Fischer's Mastery of Surgery 8th Ed.)
Summary
| Feature | Clinical Significance |
|---|---|
| Stone impaction | Causes acute cholecystitis (~90% of cases) |
| Compression of common hepatic duct | Mirizzi syndrome Type I - obstructive jaundice |
| Erosion into common hepatic duct | Mirizzi syndrome Types II-IV - cholecystocholedochal fistula |
| Tethering to duodenum | Risk of duodenal injury during surgery |
| Obscures cystic duct | Must be mobilized first to prevent bile duct injury at cholecystectomy |
| Subtotal cholecystectomy landmark | Defines safe limit of resection in difficult cases |
In short, Hartmann's pouch is a small anatomical feature with disproportionately large clinical consequences - it is the principal site of stone trapping, the origin of Mirizzi syndrome, and a key surgical landmark that the operating surgeon must identify and respect in every cholecystectomy.
This is a shared conversation. Sign in to Orris to start your own chat.