Development of kidney with developmental anomalies to score full marks in anatomy university examination
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the comprehensive content needed. Let me compile the full exam-ready answer.
Development of the Kidney with Developmental Anomalies
Source: Langman's Medical Embryology, 14th Edition - Chapter 16: Urogenital System
OVERVIEW
The urogenital system develops from the intermediate mesoderm along the posterior abdominal wall. Both the urinary and genital systems develop from a common mesodermal ridge, and their excretory ducts initially enter a common cavity - the cloaca.
THREE SUCCESSIVE KIDNEY SYSTEMS
Three kidney systems develop in a cranio-caudal sequence, each overlapping the previous:
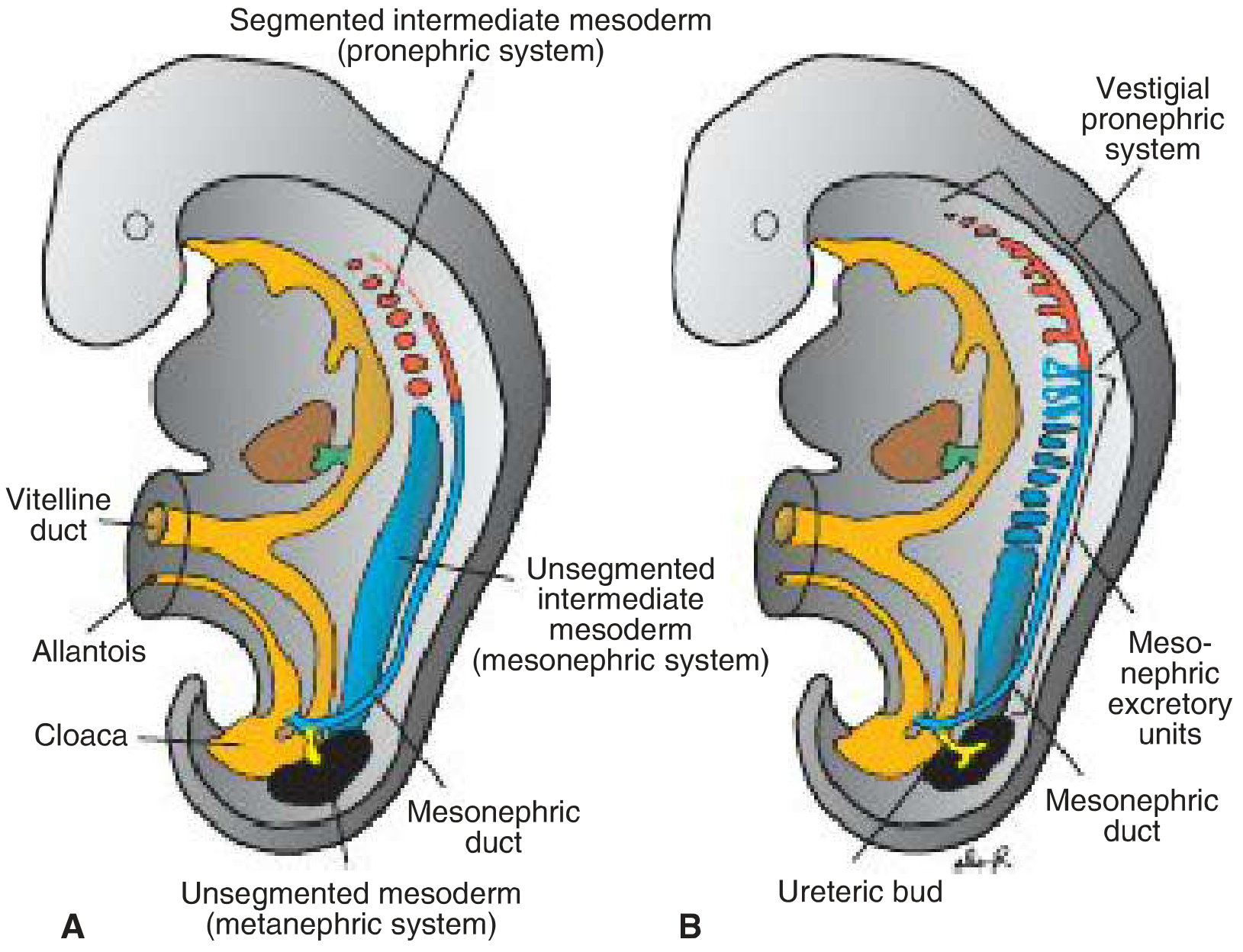
Fig. 16.2 - Intermediate mesoderm giving rise to the three kidney systems. Note the mesonephric (Wolffian) duct and the ureteric bud arising from it.
1. PRONEPHROS
| Feature | Details |
|---|---|
| Timing | Beginning of the 4th week |
| Location | Cervical region (7-10 cell groups) |
| Origin | Segmented intermediate mesoderm |
| Units | Vestigial excretory units called nephrotomes |
| Fate | Completely regresses by end of 4th week |
| Function | Non-functional (rudimentary) |
Key point: Although the pronephros is vestigial, the pronephric duct persists and is taken over by the mesonephros to become the mesonephric (Wolffian) duct.
2. MESONEPHROS
| Feature | Details |
|---|---|
| Timing | 4th week, as pronephros regresses |
| Location | Upper thoracic to upper lumbar (L3) segments |
| Origin | Intermediate mesoderm (thoracolumbar) - unsegmented nephrogenic cord |
| Peak | Forms a large ovoid organ by mid-2nd month |
| Ridge | Urogenital ridge (mesonephros + developing gonad) |
Structure: Tubules become S-shaped, acquire capillary tufts (glomeruli), form Bowman capsule, and drain laterally into the mesonephric (Wolffian) duct which opens into the cloaca.
Fate: Mostly regresses by end of 2nd month.
- In males: a few caudal tubules + the mesonephric duct persist to form the epididymis, vas deferens, ejaculatory duct, seminal vesicles.
- In females: the mesonephric duct disappears (vestigial remnants may remain as Gartner duct cysts).
3. METANEPHROS (The Permanent/Definitive Kidney)
| Feature | Details |
|---|---|
| Timing | Appears in the 5th week |
| Becomes functional | ~12th week |
| Origins | Two sources: (1) Ureteric bud, (2) Metanephric mesoderm |
Two Sources of the Metanephros
A. Ureteric Bud (Collecting System)
- Outgrowth of the mesonephric duct close to its entrance into the cloaca
- Penetrates the metanephric mesoderm (metanephric blastema/cap)
- The bud dilates to form the primitive renal pelvis, then splits into cranial and caudal parts - the future major calyces
- Each calyx forms 2 new buds, continuing to subdivide (~12+ generations of tubules) forming:
- Major calyces
- Minor calyces
- Collecting tubules
- Collecting ducts
B. Metanephric Mesoderm (Excretory Units / Nephrons)
Each collecting tubule is covered by a metanephric tissue cap. Under inductive influence:
- Tissue cap cells form small vesicles → renal vesicles
- Renal vesicles form small S-shaped tubules
- Capillaries grow into one end → differentiate into glomeruli
- Proximal end of tubule forms Bowman capsule (deeply indented by glomerulus)
- Distal end opens into a collecting tubule (establishing a passageway from Bowman capsule to collecting unit)
- Continuous lengthening forms:
- Proximal convoluted tubule (PCT)
- Loop of Henle
- Distal convoluted tubule (DCT)
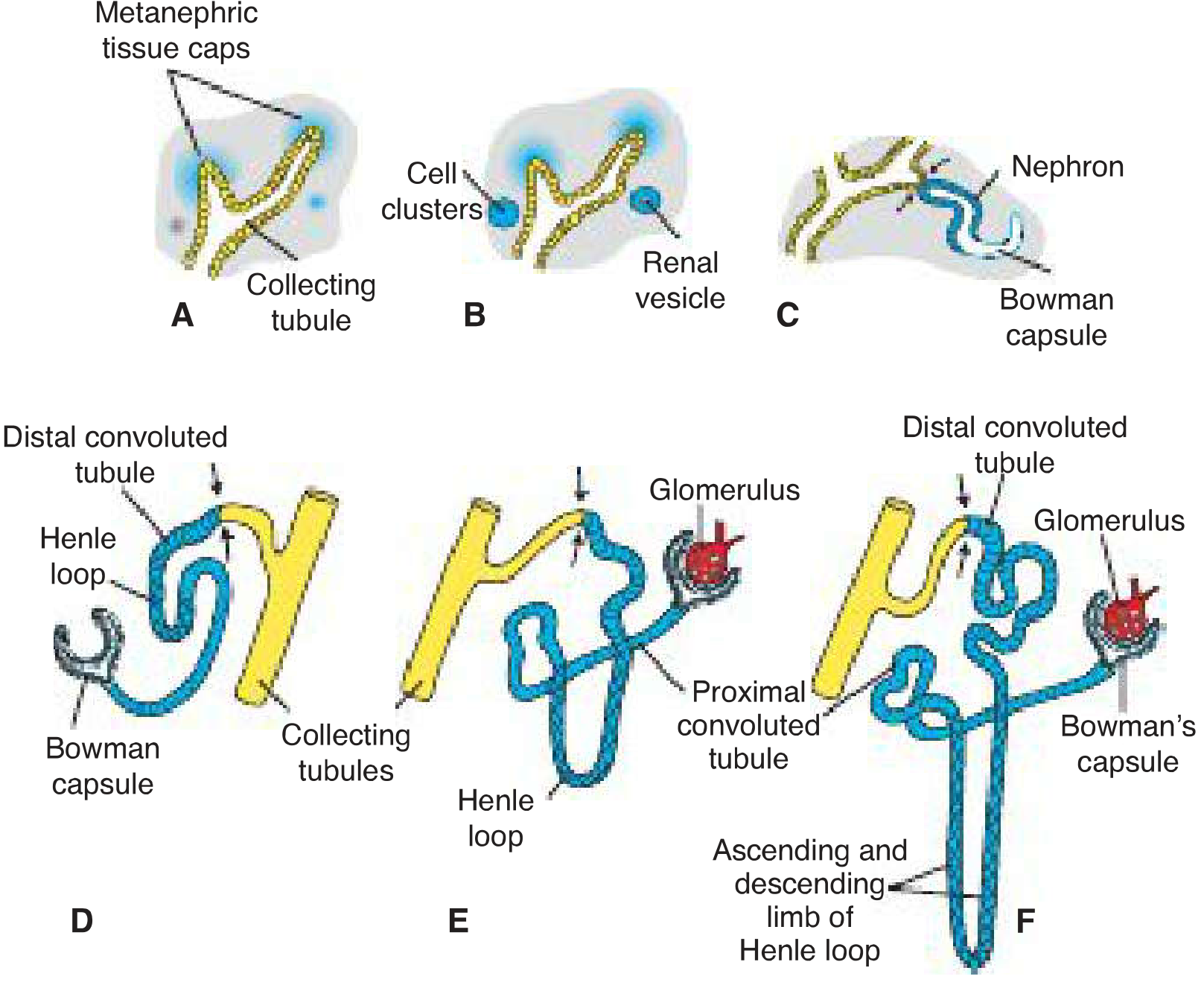
Fig. 16.6 A-F - Development of a metanephric excretory unit. The excretory unit (blue) establishes open communication with the collecting system (yellow), allowing urine flow from glomerulus to collecting ducts.
Key summary: The kidney develops from two sources:
- Metanephric mesoderm → provides excretory units (nephrons)
- Ureteric bud → gives rise to the collecting system
MOLECULAR REGULATION OF KIDNEY DEVELOPMENT
This involves critical epithelial-mesenchymal interactions:
| Signal | Source | Target | Effect |
|---|---|---|---|
| WT1 (Wilms tumor gene) | Metanephric mesenchyme | Self | Makes mesenchyme competent to respond to induction; also regulates GDNF and HGF |
| GDNF (glial-derived neurotrophic factor) | Mesenchyme | Ureteric bud epithelium (via RET receptor) | Stimulates branching and growth of ureteric buds |
| HGF (hepatocyte growth factor / scatter factor) | Mesenchyme | Ureteric bud epithelium (via MET receptor) | Stimulates branching and growth |
| FGF2 (fibroblast growth factor 2) | Ureteric bud | Mesenchyme | Blocks apoptosis, stimulates proliferation in metanephric mesenchyme; maintains WT1 |
| BMP7 (bone morphogenetic protein 7) | Ureteric bud | Mesenchyme | Same as FGF2 |
| WNT9B, WNT6 | Ureteric bud | Mesenchyme | Converts mesenchyme to epithelium for nephron formation |
ASCENT (POSITIONAL CHANGE) OF THE KIDNEY
- Metanephros initially lies in the pelvic region
- Ascends to the lumbar/abdominal position due to:
- Diminution of body curvature
- Growth of the body in lumbar and sacral regions
- As it ascends, vascular supply shifts from pelvic branches to progressively higher aortic branches
- The kidney also rotates medially ~90° so the hilum faces medially
Timing of function: Kidney becomes functional near the 12th week; urine is passed into amniotic cavity and mixes with amniotic fluid. The placenta (not kidney) is responsible for waste excretion in fetal life.
Nephron numbers: ~1 million nephrons per kidney at birth; no new nephrons form after birth.
DEVELOPMENTAL ANOMALIES OF THE KIDNEY
1. Renal Agenesis
| Type | Features |
|---|---|
| Bilateral renal agenesis | Incompatible with life; leads to oligohydramnios (↓ amniotic fluid because fetus cannot produce urine), Potter sequence |
| Unilateral renal agenesis | Compatible with life; remaining kidney undergoes compensatory hypertrophy |
Potter Sequence (Potter Syndrome):
- Caused by bilateral renal agenesis → oligohydramnios → uterine compression
- Features: flattened face (Potter facies), club feet, pulmonary hypoplasia (life-threatening), limb deformities
- Associated defects: cardiac anomalies, tracheal/duodenal atresias, cleft lip/palate, brain abnormalities
- Severe associated reproductive tract defects: absent/abnormal vagina and uterus (females), absent vas deferens/seminal vesicles (males)
Cause: Failure of the ureteric bud to develop, or failure of the metanephric mesoderm to respond to induction.
2. Ectopic (Pelvic) Kidney
- During ascent through the arterial fork formed by the umbilical arteries, one kidney may fail to pass through
- Remains in the pelvis close to the common iliac artery = pelvic kidney
- The kidney retains its fetal (pelvic) blood supply
- Usually asymptomatic, but prone to:
- Hydronephrosis (angulation of ureter)
- Urinary tract infections
- Renal calculi
3. Horseshoe Kidney
- Most common fusion anomaly of the kidney (1 in 400-500 people)
- Mechanism: During passage through the arterial fork of the umbilical arteries, both kidneys are pushed together and their lower poles fuse
- The fused mass (horseshoe) is usually at the level of the lower lumbar vertebrae (specifically L3), trapped beneath the inferior mesenteric artery - which prevents complete ascent
- The isthmus connecting the two kidneys is typically parenchymal or fibrous
- Clinical implications:
- Increased risk of ureteropelvic junction obstruction
- Increased risk of renal calculi and UTI
- Associated with Turner syndrome (45, XO)
4. Polycystic Kidney Disease (PKD)

Polycystic kidney - surface view showing multiple cysts.
Two forms exist:
| Feature | ARPKD (Autosomal Recessive) | ADPKD (Autosomal Dominant) |
|---|---|---|
| Incidence | 1/5,000 births | 1/500-1/1,000 births |
| Cysts arise from | Collecting ducts | All segments of the nephron |
| Progression | Rapid - renal failure in infancy/childhood | Slow - usually no failure until adulthood |
| Severity | More severe | Less severe |
| Gene defect | Mutations in ciliary proteins | Mutations in ciliary proteins (PKD1, PKD2) |
Pathogenesis: Both types are ciliopathies - mutations in genes encoding proteins localized in cilia that are important for ciliary function.
Related ciliopathy syndromes:
- Bardet-Biedl syndrome: renal cysts + obesity + intellectual disability + limb defects
- Meckel-Gruber syndrome: renal cysts + hydrocephalus + microphthalmia + cleft palate + absence of olfactory tract + polydactyly
5. Duplex (Double) Ureter and Collecting System
- Results from early splitting of the ureteric bud before it contacts the metanephric blastema
- May be:
- Partial duplication - ureters join before entering the bladder
- Complete duplication - two separate ureters entering the bladder (or elsewhere)
- Metanephric tissue may be divided into two parts, each with its own renal pelvis and ureter
- Ectopic ureter: results from development of two ureteric buds; the abnormal bud moves down together with the mesonephric duct and opens into the vagina, urethra, or vestibule (females) or epididymal region (males)
- In females: the ectopic ureteral opening below the external urethral sphincter causes continuous dribbling of urine despite normal micturition
6. Multicystic Dysplastic Kidney (MCDK)
- Results from failure of the ureteric bud to contact the metanephric mesoderm or from atresia of the ureter early in development
- Kidney is non-functional and replaced by cysts
- Usually unilateral (bilateral = incompatible with life)
Summary Table: Developmental Anomalies at a Glance
| Anomaly | Embryological Basis | Key Clinical Feature |
|---|---|---|
| Bilateral renal agenesis | Failure of ureteric bud / metanephric response | Potter sequence; oligohydramnios |
| Unilateral renal agenesis | Same, unilateral | Compensatory hypertrophy; often asymptomatic |
| Pelvic kidney | Failure to ascend through umbilical artery fork | Risk of UTI, hydronephrosis |
| Horseshoe kidney | Fusion of lower poles during ascent | Trapped below inferior mesenteric artery |
| Polycystic kidney (AR) | Ciliopathy; cysts from collecting ducts | Renal failure in infancy/childhood |
| Polycystic kidney (AD) | Ciliopathy; cysts from all nephron segments | Renal failure in adulthood |
| Duplex ureter | Early splitting of ureteric bud | Ectopic ureter may open into vagina/urethra |
| Supernumerary kidney | Separate ureteric bud induction | Rare; accessory kidney |
QUICK EXAM REVISION MNEMONICS
"3 P's of kidney development": Pronephros → Paramesonephros (Mesonephros) → Permanent (Metanephros)
Ureteric bud gives: Pelvis, major/minor calyces, collecting tubules, ureter
Metanephric mesoderm gives: Bowman capsule, PCT, loop of Henle, DCT (everything proximal to collecting duct)
Horseshoe kidney is trapped by: Inferior Mesenteric Artery (IMA)
Potter sequence (OPAL): Oligohydramnios → Pulmonary hypoplasia → Absent kidneys → Limb deformities
PKD is a ciliopathy: Both AR and AD forms involve mutations in cilia-related proteins
FREQUENTLY ASKED EXAM POINTS
- Pronephros = vestigial, non-functional, disappears by end of week 4
- Mesonephros = functional temporarily; mesonephric duct is key (becomes Wolffian duct; forms male genital ducts)
- Metanephros = permanent kidney; appears week 5, functional week 12
- The kidney develops from TWO sources (must state both for full marks)
- Kidney ascent: pelvic → abdominal; rotation: hilum faces medially
- ~1 million nephrons at birth; no new nephrons form after birth
- WT1 mutation → associated with Wilms tumor (nephroblastoma) in children - one of the most common childhood abdominal tumors
- Horseshoe kidney: most common fusion anomaly, halted by inferior mesenteric artery
- Potter sequence: always explain the mechanism (bilateral agenesis → oligohydramnios → compression → features)
- Polycystic kidney = ciliopathy (high-yield molecular fact)
- Langman's Medical Embryology, 14th Edition - Chapter 16: Urogenital System
This is a shared conversation. Sign in to Orris to start your own chat.