
a81d893a-f01b-4b42-a66f-ada3f25d3082.jpg
Diagnosis and treatment
analyse_media
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Diagnosis: Pseudomembranous Oral Candidiasis (Thrush)
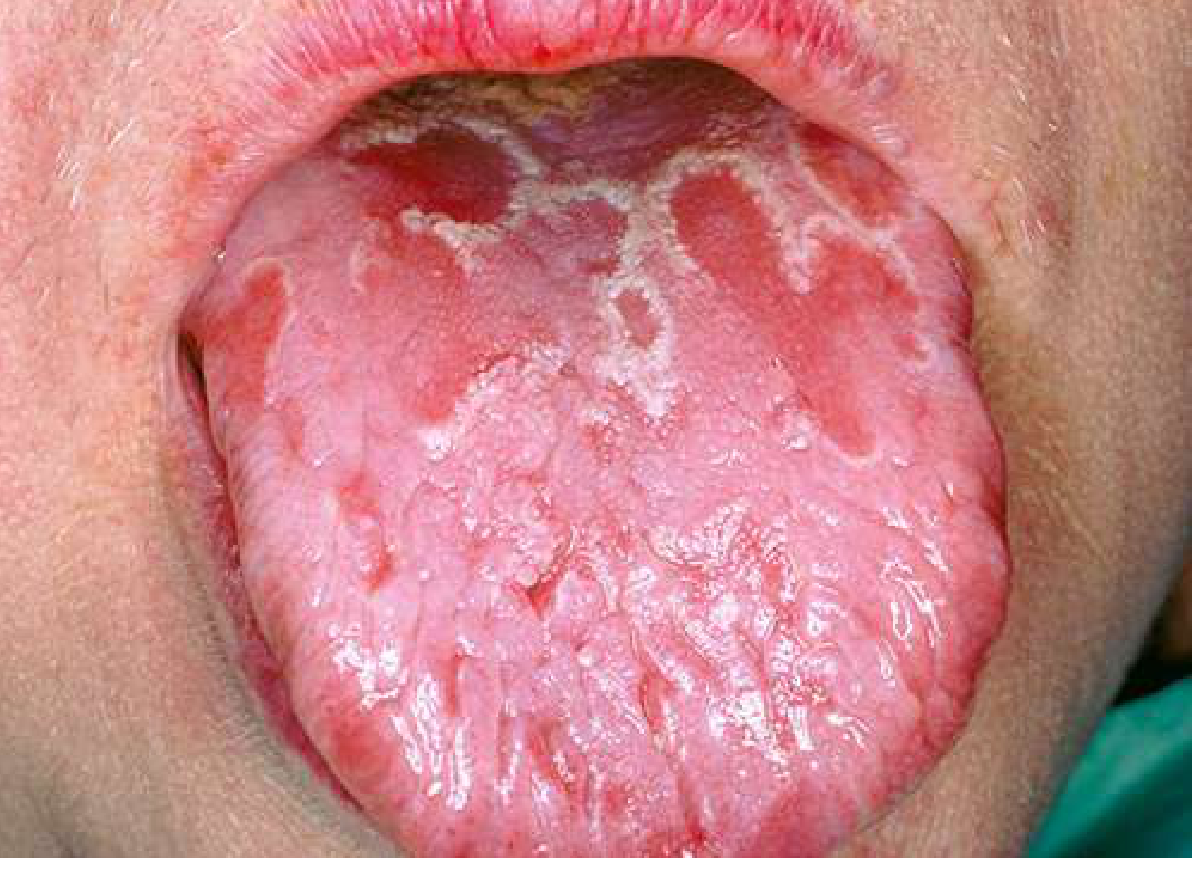
The image shows the classic appearance of pseudomembranous oral candidiasis (thrush): a well-demarcated, raised, white-to-cream colored plaque on the soft palate with surrounding diffuse erythema of the pharyngeal mucosa. The tongue itself appears relatively normal, which is consistent with early or palate-predominant thrush.
For comparison, here is a textbook image of oral candidiasis (geographic tongue variant shown; the white patches on an erythematous base are the hallmark):
Key Diagnostic Features in This Image
| Feature | Finding |
|---|---|
| White plaque | Raised, cream-colored patch on soft palate - can be rubbed off leaving a red/bleeding base |
| Background mucosa | Diffuse erythema of soft palate and posterior pharynx |
| Tongue | Largely normal (no thick plaques here) |
| Distribution | Palate - a classic site |
Differential Diagnosis
- Pseudomembranous candidiasis (most likely) - white plaques that wipe off, on erythematous base
- Erythematous (atrophic) candidiasis - more red/burning presentation; may coexist
- Hairy leukoplakia - white villous patches on the lateral tongue (EBV-associated, seen in HIV); does NOT wipe off; different location
- Lichen planus - white lacy/reticular pattern; does not wipe off
- Leukoplakia - pre-malignant white patch; does not wipe off; no erythema typically
- Streptococcal/viral pharyngitis exudate - usually on tonsils with fever and sore throat
The scrapability of the white patch is the clinical key: if it wipes off leaving a raw, red base, it is candidiasis. If it does not wipe off, leukoplakia or lichen planus must be considered.
Predisposing Factors to Assess
- Recent antibiotic or corticosteroid (including inhaled) use
- Diabetes mellitus or other endocrine disorder
- Wearing dentures
- HIV infection / immunosuppression (candidiasis is an AIDS-defining illness in adults without other risk factors)
- Xerostomia (Sjogren syndrome, anticholinergic drugs, radiotherapy)
- Malignancy or chemotherapy
If this patient has no dentures, no recent antibiotics, and no other obvious cause, HIV testing and immune workup are warranted.
Treatment
First-line (topical) - mild/moderate disease:
- Clotrimazole troches 10 mg dissolved in mouth 5 times daily for 7-14 days (preferred - no systemic side effects)
- Nystatin suspension 400,000-600,000 units swished and swallowed 4 times daily for 7-14 days
- Nystatin pastilles 200,000 units dissolved 4 times daily
Systemic therapy - moderate/severe or immunocompromised:
- Fluconazole 200 mg loading dose on day 1, then 100 mg daily for 7-14 days (drug of choice)
- For fluconazole-resistant cases: itraconazole oral solution 200 mg daily, or posaconazole
Special situations:
- Xerostomic patients (insufficient saliva to dissolve troches): use vaginal nystatin tablets 100,000 units dissolved slowly twice daily, or miconazole mucoadhesive buccal tablets 50 mg daily - these contain little cariogenic sugar
- Denture-associated candidiasis: disinfect and ensure good fit of the denture in addition to antifungal therapy
- Recurrent/immunosuppressed patients: may need long-term maintenance antifungal therapy
Treatment endpoint: Symptoms of mucosal burning resolve, tolerance of spicy/acidic foods returns, and filiform papillae normalize - this can take 2-12 weeks depending on salivary function.
Sources: Goldman-Cecil Medicine, p. 4154-4155; Rosen's Emergency Medicine, p. 2410; Andrews' Diseases of the Skin, p. 354
Clinical note: This is a visual/clinical assessment based on the photograph. Definitive diagnosis requires in-person examination (including scraping the lesion) and, if needed, KOH preparation or culture. A healthcare provider should also evaluate for underlying immunosuppression if no obvious precipitant is identified.
This is a shared conversation. Sign in to Orris to start your own chat.