Hypertension emergency vs urgency
Reading File
Finding Sources
Searching PubMed
"hypertensive emergency" AND "hypertensive urgency" AND management
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have excellent material. Let me compile the comprehensive answer.
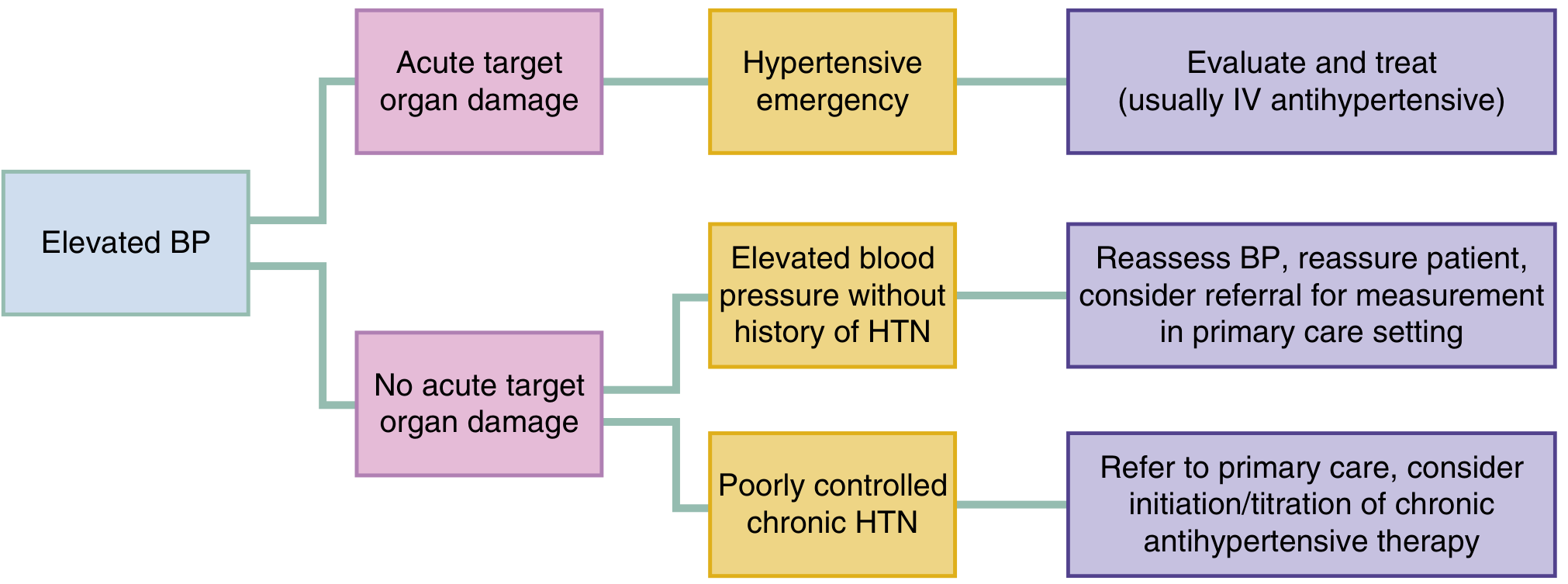
Hypertensive Emergency vs. Urgency
Core Distinction
The single most important differentiator is acute target organ damage (TOD) - not the BP number itself.
| Feature | Hypertensive Emergency | Hypertensive Urgency |
|---|---|---|
| BP level | Typically ≥ 180/120 mmHg | Typically ≥ 180/120 mmHg |
| Acute target organ damage | YES | NO |
| Setting | ICU / monitored inpatient | Outpatient / ED discharge |
| Treatment route | IV antihypertensives | Oral agents or observation |
| Speed of BP reduction | Controlled, gradual over hours | Slow, over 24-48 hours |
| Urgency of treatment | Immediate | Non-emergent |
"A hypertensive emergency is a disease state defined by acute TOD, manifest by newly developed clinical sequelae or diagnostic test abnormalities. A hypertensive emergency can exist in patients with or without underlying chronic HTN." - Rosen's Emergency Medicine
Hypertensive Emergency
Target Organs and Clinical Presentations
| Organ | Clinical Syndrome |
|---|---|
| Brain | Hypertensive encephalopathy, acute ischemic stroke, intracranial hemorrhage |
| Heart | Acute coronary syndrome, acute decompensated heart failure |
| Kidneys | Acute kidney injury, thrombotic microangiopathy |
| Aorta | Aortic dissection |
| Eyes | Hypertensive retinopathy (papilledema, flame hemorrhages, cotton wool spots, macular edema) |
| Obstetric | Pre-eclampsia / eclampsia |
Pathophysiology
Severe hypertension overwhelms cerebral and systemic autoregulation, triggering a cascade of endothelial dysfunction, fibrinoid necrosis of arterioles, and end-organ ischemia. The "onion skin" concentric subendothelial thickening of arterioles and microangiopathic hemolysis (MAHA) are histologic hallmarks seen in the kidney.
BP Reduction Goals (Emergency)
Key principle: Control of ongoing end-organ damage is more important than any absolute BP number. Reduction should be gradual - sudden drops can induce ischemia.
| Clinical Scenario | Target |
|---|---|
| Most hypertensive emergencies | Reduce MAP by ~20-25% in first hour, then to ~160/100 over 2-6 hours |
| Ischemic stroke (thrombolysis planned) | < 185/110 mmHg before tPA; maintain < 180/110 |
| Ischemic stroke (no thrombolysis) | Treat only if BP > 220/120; reduce ~15% over 24 hours |
| Spontaneous intracranial hemorrhage | Target SBP 140 mmHg rapidly via IV agents |
| Aortic dissection | SBP < 120 within minutes; heart rate < 60 (IV beta-blocker first) |
| Acute decompensated heart failure | Vasodilators (nitroprusside/nitroglycerin) |
| Pre-eclampsia / eclampsia | < 155/105 mmHg with IV labetalol or hydralazine |
IV Agents Used in Emergency
| Drug | Class | Onset | Duration | Notes |
|---|---|---|---|---|
| Labetalol | Alpha + beta blocker | 2-5 min | 3-6 h | 20-80 mg IV bolus q10 min or infusion; preferred in stroke, pregnancy |
| Nicardipine | CCB | 5-15 min | 4-6 h | 5-15 mg/h IV; preferred when fine titration needed |
| Clevidipine | CCB (4th gen) | 1-2 min | 1-5 min | 2-32 mg/h; ultra-short acting, easiest to control |
| Esmolol | Beta-1 blocker | 1-2 min | 20 min | Good for dissection (heart rate control); 0.5-1 mg/kg load then infusion |
| Sodium nitroprusside | NO donor/vasodilator | Immediate | 1-2 min | Potent; risk of cyanide toxicity; avoid in stroke (raises ICP) |
| Nitroglycerin | Nitrate | 2-5 min | 5-10 min | Preferred in ACS/flash pulmonary edema |
| Hydralazine | Direct vasodilator | 10-20 min | 2-4 h | Causes reflex sympathetic activation; used in pregnancy |
| Phentolamine | Alpha blocker | 1-2 min | 10-30 min | Catecholamine excess (pheochromocytoma, cocaine) |
| Fenoldopam | Dopamine agonist | < 5 min | 30 min | Renal-protective; useful in AKI |
Avoid beta-blockers alone in cocaine-induced hypertension (unopposed alpha stimulation). Avoid nitroprusside in acute stroke (raises ICP).
Hypertensive Urgency (No Target Organ Damage)
Key Points
- Elevated BP (≥ 180/120) WITHOUT acute TOD - this includes patients with chronic poorly-controlled HTN, missed doses, or newly detected BP elevation
- Acute reduction is NOT required and may be harmful - sublingual nifedipine and similar rapid-acting agents have caused reflex hypoperfusion and strokes
- Nonspecific symptoms (headache, dizziness, epistaxis) are common but do NOT reliably correlate with BP level and do NOT by themselves indicate a hypertensive emergency
- Epistaxis: Despite popular belief, there is no causal relationship between acute severe hypertension and nosebleeds
Management
- Restart missed oral medications if applicable
- If initiating new therapy, use long-acting oral agents (amlodipine, lisinopril, HCTZ)
- Arrange outpatient follow-up within 24-72 hours
- No need to achieve a specific BP target before ED discharge
- Do not administer short-acting agents (clonidine, hydralazine) solely to lower numbers - evidence shows this increases subsequent ED visits without improving outcomes
Diagnostic Workup in Emergency
| Test | Purpose |
|---|---|
| BMP / Creatinine / UA | Renal involvement, electrolytes |
| CBC + peripheral smear | MAHA (schistocytes suggest TMA) |
| ECG + Troponin + BNP | Cardiac involvement |
| Chest X-ray | Pulmonary edema, widened mediastinum |
| CT head (non-contrast) | ICH, rule out ischemic stroke |
| CT angiography chest | Aortic dissection if suspected |
| Fundoscopy | Hypertensive retinopathy (papilledema = emergency) |
| Urine pregnancy test | Pre-eclampsia in women of childbearing age |
Disposition
- Emergency: Admit to ICU with continuous arterial line monitoring and IV infusion titration
- Urgency / poorly controlled HTN: Discharge with oral agents + PCP follow-up within 1-3 days; incidence of short-term adverse events is low when TOD has been ruled out
Sources:
- Rosen's Emergency Medicine, 9th Ed., Ch. 70 (Hypertension)
- Morgan & Mikhail's Clinical Anesthesiology, 7th Ed.
- Harrison's Principles of Internal Medicine, 22nd Ed.
- Washington Manual of Medical Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.