What is sickle cell anemia
Reading File
Searching the Web
sickle cell anemia overview pathophysiology treatment 2025
Finding Sources
Searching PubMed
"sickle cell disease" AND treatment
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have rich textbook content and images. Let me compile the full answer.
Sickle Cell Anemia
Sickle cell anemia is the most common hereditary hemolytic anemia, caused by a single point mutation in the beta-globin (HBB) gene. It is the prototypic hemoglobinopathy.
Genetics and Epidemiology
- Inheritance: Autosomal recessive. The mutation causes glutamate to be replaced by valine at position 6 of the beta-globin chain, producing abnormal sickle hemoglobin (HbS).
- In the United States, approximately 8% of people of African descent are heterozygous (sickle cell trait), and about 1 in 600 have sickle cell anemia (homozygous HbSS).
- The HbS allele is prevalent in equatorial Africa, parts of India, southern Europe, and the Middle East because it confers protection against falciparum malaria.
Pathogenesis
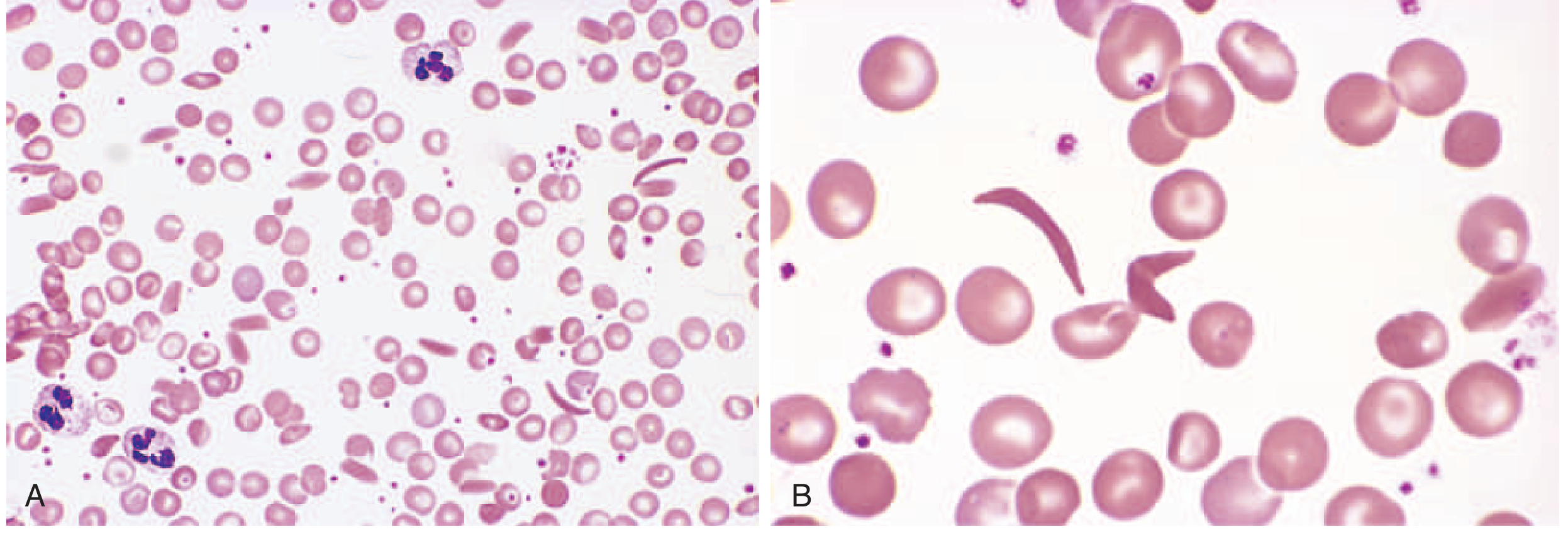
Fig. 10.3 - Peripheral smear in sickle cell anemia. Panel A (low power) shows a mixture of elongated sickled and normal red cells. Panel B (high power) shows the classic crescent/sickle shape clearly.
On deoxygenation, HbS molecules undergo a conformational change that drives them to polymerize into long fibers via their abnormal valine residues. These polymer fibers distort the red cell into an elongated, crescent/sickle shape.
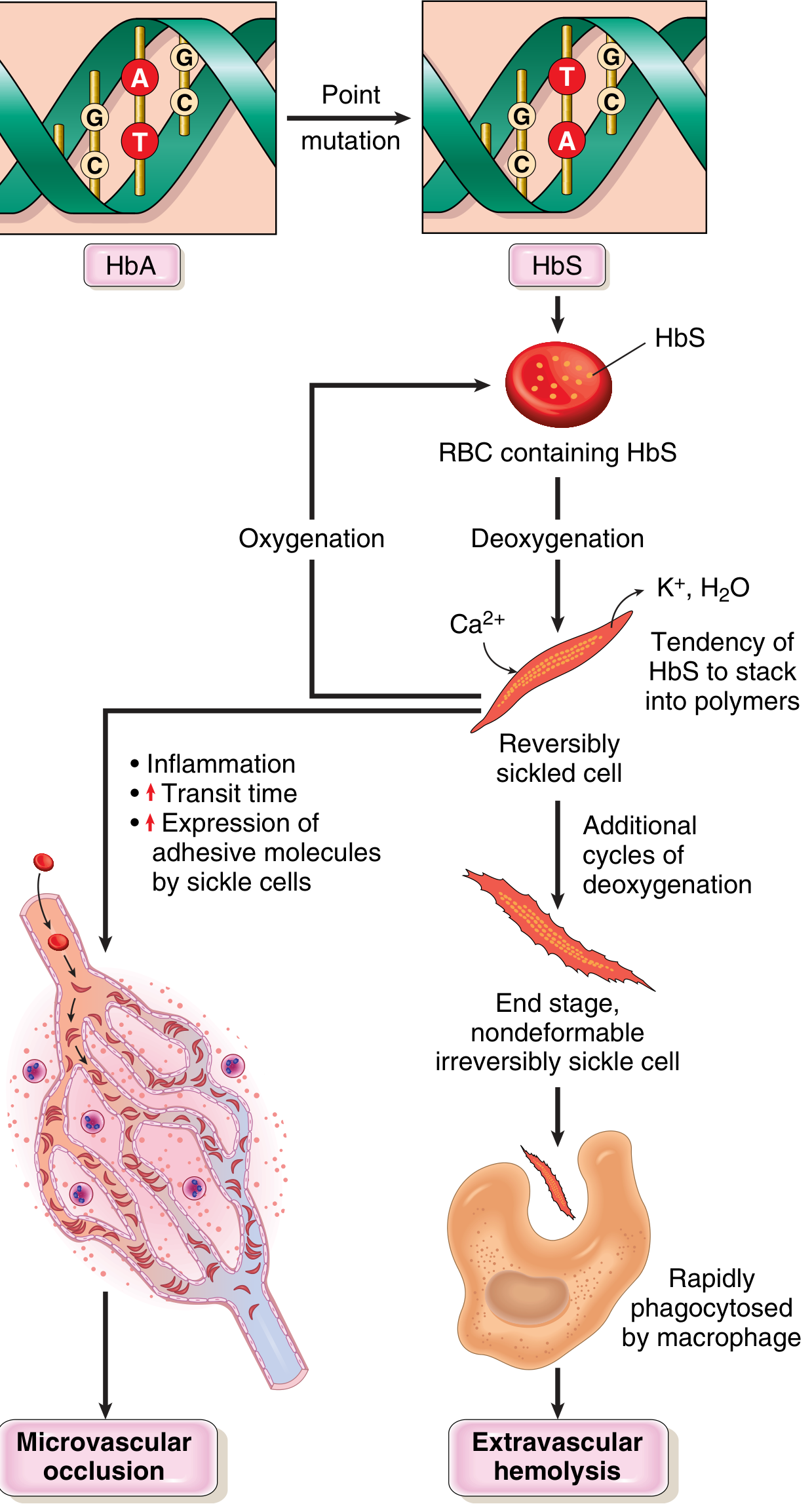
Fig. 10.4 - Pathophysiology of sickle cell disease (Robbins & Kumar Basic Pathology)
Three key factors determine the clinical severity of sickling:
| Factor | Effect |
|---|---|
| Other hemoglobin types (HbA, HbF) | HbA and HbF retard HbS polymerization. Newborns are protected until HbF falls (~5-6 months of age). Heterozygotes (sickle cell trait) rarely sickle in vivo. |
| Intracellular HbS concentration | Dehydration increases Hb concentration, promoting sickling. Co-existing alpha-thalassemia reduces sickling. |
| Microvascular transit time | Sluggish flow (spleen, bone marrow, inflamed tissues) prolongs the time available for polymerization to occur. |
Sickling is initially reversible on reoxygenation. Repeated cycles cause calcium influx, loss of K+ and water, and membrane damage, creating irreversibly sickled cells prone to hemolysis. The red cell lifespan drops to ~20 days (one-sixth of normal).
Two Major Pathologic Consequences
1. Chronic Hemolytic Anemia
- Hematocrit typically 18-30% (normal: 38-48%)
- Compensatory reticulocytosis and hyperbilirubinemia
- Compensatory erythroid hyperplasia in marrow causes "crew-cut" skull on X-ray
2. Vaso-occlusive Crises
Sickle cells are sticky and block small blood vessels, causing ischemia and pain in various organs.
Clinical Features
The disease is asymptomatic until ~6 months of age, when HbF is replaced by HbS.
Common vaso-occlusive crises:
- Hand-foot syndrome - bone infarction in hands and feet; most common presenting symptom in young children
- Acute chest syndrome - sickling in hypoxemic pulmonary beds (can be triggered by pneumonia or fat emboli from infarcted bone); a leading cause of death
- Stroke - ischemia from cerebrovascular occlusion; the other leading cause of death
- Aplastic crisis - sudden drop in red cell production, typically triggered by parvovirus B19 infection of erythroblasts
- Proliferative retinopathy - vasoocclusion in the eye can cause blindness
- Priapism - painful, prolonged erection that can lead to penile fibrosis
Organ damage over time:
- Autosplenectomy - repeated splenic infarcts reduce the spleen to a fibrous nubbin; functionally asplenic by adulthood
- Functional asplenia makes patients highly susceptible to encapsulated bacteria (pneumococcus) and gram-negative organisms like Salmonella (osteomyelitis)
- Fatty changes in heart, liver, and renal tubules from hypoxia
- Avascular necrosis of the femoral head and other bones
Diagnosis
- Newborn screening (heel-stick): gel electrophoresis identifies HbS; mandatory in the United States
- Peripheral blood smear: elongated, boat-shaped irreversibly sickled cells in homozygous disease
- Sickling test: in sickle cell trait, sickling can be induced in vitro by hypoxia
- Prenatal diagnosis: fetal DNA analysis via amniocentesis or chorionic villus sampling
Treatment
| Approach | Details |
|---|---|
| Hydroxyurea | Increases HbF levels, reducing sickling frequency and severity; first-line disease-modifying therapy |
| Analgesics | Pain crises managed with NSAIDs, opioids; ketorolac is commonly used in emergency settings |
| Blood transfusions / exchange transfusion | For severe anemia, acute chest syndrome, stroke. Goal: HbS <40%, Hb ~10 g/dL |
| Prophylactic penicillin | Given to children with asplenia to prevent encapsulated bacterial infections |
| Pneumococcal vaccination | Essential for asplenic patients |
| Hematopoietic stem cell transplant (HSCT) | Currently the only established cure; limited by donor availability and transplant-related risks |
| Gene therapy (CRISPR/Cas9) | Emerging curative approach - a 2026 systematic review (PMID 39794549) confirmed clinical trial success for CRISPR-based therapies in SCD and thalassemia |
| Pyruvate kinase activators | Novel therapeutic target - a 2026 meta-analysis (PMID 41742605) explored this emerging class |
Note on pregnancy: Hydroxyurea is contraindicated in pregnancy. Vaso-occlusive crises are more frequent during pregnancy, and pregnant patients with SCD have a ~sixfold increased risk of maternal death.
Sickle Cell Trait vs. Sickle Cell Anemia
| Sickle Cell Trait (HbAS) | Sickle Cell Anemia (HbSS) | |
|---|---|---|
| Genotype | Heterozygous (one copy) | Homozygous (two copies) |
| % HbS | ~40% | ~100% |
| Symptoms | Usually none | Chronic anemia + crises |
| Sickling in vivo | Rare | Common under stress/hypoxia |
| Malaria protection | Yes | Yes (but disease burden high) |
Sources: Robbins & Kumar Basic Pathology, pp. 386-388 | Rosen's Emergency Medicine, p. 3377 | NCBI StatPearls - Sickle Cell Anemia | Frontiers in Pharmacology 2025 - Gene therapy in SCD
What it do
Not much! Just here and ready to help. What do you need?
What it cause does it stop synthesis blood or destroy blood cell
Great question! Sickle cell anemia destroys red blood cells (hemolysis), it does NOT stop their production. Here's the breakdown:
It Destroys Blood Cells - Here's How
Normal red blood cells live about 120 days.
Sickle cells live only about 20 days - they die 6x faster than normal.
Why do they get destroyed?
-
The sickle shape makes them fragile - the stiff, crescent-shaped cells rupture easily as they try to squeeze through tiny blood vessels.
-
The spleen traps and destroys them - the spleen is the body's filter for damaged red cells. It recognizes sickle cells as abnormal and breaks them down rapidly.
-
Repeated sickling damages the membrane - each time a cell sickles and un-sickles, it takes damage. Eventually the cell becomes permanently deformed and gets cleared by the immune system.
So Why Does Anemia Happen?
The bone marrow IS still producing red blood cells - actually it works overtime trying to keep up (this is called compensatory reticulocytosis). But the destruction is so fast that production can't keep pace.
Think of it like a leaky bucket - you keep filling it (production), but water keeps pouring out the holes (destruction). The bucket never fills up.
The One Exception - Aplastic Crisis
There IS a situation where production STOPS temporarily - called an aplastic crisis, triggered by parvovirus B19 infection. The virus infects the bone marrow cells that make red blood cells, halting production. This causes a sudden severe drop in hemoglobin on top of the ongoing destruction - a medical emergency.
Bottom line: Sickle cell anemia is a hemolytic (destruction-based) anemia, not a production failure. The cells are made fine, they just don't survive long enough.
This is a shared conversation. Sign in to Orris to start your own chat.