Ascending paralysis with low DBP with fever approach
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching the Web
ascending paralysis low diastolic blood pressure fever differential diagnosis clinical approach
Excellent. I now have comprehensive information to construct a thorough clinical approach. The key insight about "low DBP with fever" in ascending paralysis is critical - this points toward either:
- GBS with autonomic dysfunction (labile BP, vasodilation causing low DBP)
- Infectious/sepsis-related causes (fever driving vasodilation, low DBP = wide pulse pressure = sepsis physiology)
- Specific toxins (tetrodotoxin, organophosphates with autonomic features)
- Beriberi (wet beriberi: neuropathy + vasodilatory low DBP heart failure)
Let me now compose the comprehensive answer.
Ascending Paralysis + Low DBP + Fever: Clinical Approach
Understanding the Triad
The combination of ascending paralysis + fever + low diastolic blood pressure (DBP) is a high-stakes triad that narrows and refines the differential diagnosis considerably. Low DBP specifically suggests vasodilation (wide pulse pressure), which can arise from:
- Autonomic nervous system dysregulation (GBS pandysautonomia)
- Sepsis/systemic infection causing vasodilatory shock
- High-output cardiac states (wet beriberi)
- Direct toxin-mediated vasodilation
Step 1: Differentiate Ascending vs. Descending Paralysis
| Feature | Ascending Paralysis | Descending Paralysis |
|---|---|---|
| Starts in | Lower limbs, moves up | Cranial nerves first, moves down |
| Examples | GBS, polio, tick paralysis, beriberi | Botulism, diphtheria |
| Reflexes | Lost (areflexia) | Lost (botulism) or preserved |
Step 2: Differential Diagnosis (Fever Modifies the List)
The presence of fever is a pivotal clue - classical GBS criteria actually state "absence of fever at onset" as a supportive feature. So fever pushes you toward infectious/toxic causes, while still keeping GBS (with secondary infection trigger) in mind.
A. INFECTIOUS CAUSES (Fever Prominent)
1. Poliomyelitis / Poliovirus-like Illness (Enteroviral Myelitis)
- Fever + flaccid asymmetric paralysis (anterior horn cell destruction)
- Meningeal signs + CSF pleocytosis (vs. GBS which has albuminocytological dissociation)
- Low DBP from sepsis physiology
- Key: asymmetric, predominantly motor, early fever
- Other enteroviruses (EV-D68, EV-A71, West Nile virus) cause similar "acute flaccid myelitis (AFM)"
2. West Nile Virus / Acute Flaccid Myelitis
- Fever + headache + asymmetric flaccid paralysis (anterior horn cell involvement)
- Often with encephalitis or meningitis
- Diagnosis: serology (CSF IgM), PCR
- Low DBP from systemic febrile illness / encephalitis-related autonomic dysregulation
3. Rabies (Paralytic Form, ~20%)
- Paralytic rabies: ascending flaccid paralysis progressing to quadriparesis, facial paralysis - closely mimics GBS
- Fever + autonomic dysfunction (labile BP, low DBP)
- History of animal bite critical; CSF may show mild pleocytosis
- As per Harrison's 22E: "Flaccid paralysis in limb(s) progressing to quadriparesis with facial paralysis" - [Harrison's Principles of Internal Medicine 22E, p. 5293]
4. Diphtheria
- Exotoxin-mediated neuropathy - descending initially (palatal palsy, accommodation palsy) then can generalize
- Fever + characteristic pseudomembrane
- Can cause autonomic dysfunction with low BP
5. Neuroborreliosis (Lyme Disease)
- Ascending weakness + radicular pain + fever
- Facial palsy (Bannwarth syndrome)
- Endemic exposure history
B. GBS WITH AUTONOMIC DYSFUNCTION + FEVER (Septic Trigger)
GBS is classically post-infectious - the fever may be from the triggering infection (Campylobacter, CMV, EBV, Zika), not from the GBS itself. Up to two-thirds of GBS patients develop autonomic dysfunction, which includes:
- Labile blood pressure (wide swings between hypertension and hypotension)
- Tachycardia / bradycardia
- Low DBP from parasympathetic over-activation or sympathetic dysregulation
- Urinary retention, ileus, excessive sweating
"In Guillain-Barré syndrome, up to two thirds of patients may have autonomic dysfunction, which can be life-threatening. Manifestations include labile blood pressure and heart rate, paralytic ileus, and urinary retention." - [Goldman-Cecil Medicine, p. 4063]
GBS diagnostic criteria (from Bradley's Neurology):
- Required: Progressive bilateral limb weakness + areflexia/hyporeflexia
- Supportive: Progression over days to 4 weeks, relative symmetry, bifacial palsies, autonomic dysfunction, mild sensory signs, elevated CSF protein with <10 cells/μL
- [Bradley and Daroff's Neurology in Clinical Practice, p. 2663]
GBS variants to know:
- AIDP (commonest in West)
- AMAN / AMSAN (axonal, associated with C. jejuni - more severe)
- Miller Fisher syndrome (ophthalmoplegia + ataxia + areflexia)
- Pandysautonomia variant
C. TOXIC / METABOLIC CAUSES (Fever from Secondary Infection)
Beriberi (Wet Beriberi - Thiamine Deficiency)
- Classic triad: ascending sensorimotor neuropathy + high-output heart failure + low DBP (vasodilatory)
- Wide pulse pressure is characteristic: low DBP with preserved or elevated systolic BP
- Fever from secondary infection
- Malnutrition, alcoholism, rice-based diet
- This is the one condition where low DBP is PATHOPHYSIOLOGICALLY central (vasodilation from thiamine-deficient peripheral vasodilation + cardiac failure)
- Treatment: IV thiamine immediately
Organophosphate / Carbamate Poisoning
- Intermediate syndrome: ascending paralysis 24-96 hours post-acute cholinergic crisis
- Autonomic dysfunction with wide BP variability
- Fever from aspiration or excess secretions
- Toxidrome: miosis, bradycardia, excessive secretions; but intermediate syndrome may have a "cleaner" presentation
Marine Toxins
- Tetrodotoxin (puffer fish): ascending paralysis within 4-24 hours, hypotension, bradycardia
- Saxitoxin (paralytic shellfish poisoning): similar
- Ciguatoxin: paresthesias, weakness, autonomic dysfunction
- Fever may be low-grade from systemic effect
Heavy Metal Toxicity
- Arsenic: ascending neuropathy + Mees' lines, GI illness, low BP
- Thallium: ascending neuropathy + alopecia
Step 3: Key Differentiating Features
| Condition | Fever | Symmetry | Reflexes | CSF | Low DBP Mechanism | Key Clue |
|---|---|---|---|---|---|---|
| GBS (AIDP) | Absent at onset (trigger may cause fever) | Symmetric | Absent | Albumino-cytological dissociation | Autonomic dysregulation | Areflexia, post-infectious |
| Polio / AFM | High fever, early | Asymmetric | Absent | Pleocytosis | Sepsis | Epidemic, anterior horn |
| Paralytic rabies | Present | Ascending, symmetric-ish | Reduced | Mild pleocytosis | Autonomic storm | Animal bite Hx |
| West Nile | Present | Asymmetric | Absent | Pleocytosis | Systemic infection | Encephalitis features |
| Wet beriberi | Secondary | Symmetric | Reduced | Normal | Vasodilation (thiamine def.) | Wide pulse pressure, heart failure |
| Tick paralysis | Absent/low | Ascending | Absent | Normal | None specific | Tick found, rapid recovery on removal |
| Botulism | Absent | Descending | Normal initially | Normal | Autonomic blockade | Pupil dilation, no fever |
| Diphtheria | Present | Descending initially | Normal | Mild changes | Myocarditis | Pseudomembrane, palatal palsy |
Step 4: Immediate Investigations
Bedside / Emergency
- Vital signs: BP (both lying and standing - check for orthostatic component), HR, SpO2
- Bedside spirometry: Forced Vital Capacity (FVC) - if <20 mL/kg, observe in ICU; <15 mL/kg consider intubation (the "20-15-30 rule" in GBS: FVC <20, MIP < -30 cmH2O)
- ECG: Autonomic instability causes cardiac arrhythmias in GBS
- Serum potassium: Hypokalemic periodic paralysis (low K+ = ascending paralysis + low DBP from associated conditions)
- Blood glucose, rapid sepsis screen
Laboratory
- CBC, CRP, procalcitonin (infection)
- Serum electrolytes (K+, Mg2+, Na+, Ca2+)
- LFTs, RFTs
- Thiamine levels (if wet beriberi suspected)
- Blood cultures (if febrile)
- Serology: anti-ganglioside antibodies (GM1, GD1b, GQ1b), C. jejuni serology
- Organophosphate screen (RBC cholinesterase)
CSF Analysis (Lumbar Puncture)
| Finding | Interpretation |
|---|---|
| High protein + <10 WBC (albuminocytological dissociation) | GBS |
| Pleocytosis (>10 WBC) | Viral myelitis, polio, rabies, meningitis |
| Normal | Tick paralysis, early GBS, toxins |
Nerve Conduction Studies / EMG
- Confirms demyelination (GBS/AIDP): slow conduction velocity, conduction blocks, prolonged F-waves
- Axonal pattern (AMAN/AMSAN): reduced amplitudes, inexcitable nerves
- Normal in early GBS (can lag 1-2 weeks)
Imaging
- MRI spine: Rule out compressive myelopathy, transverse myelitis (T2 signal changes), epidural abscess
- MRI brain: Encephalitis, brainstem involvement (West Nile, rabies, ADEM)
- Chest X-ray: Aspiration, mediastinal widening (diphtheria - anthrax in bioterrorism)
Step 5: Management Approach
1. Airway - PRIORITY ONE
- Monitor FVC every 4-6 hours in any progressive ascending paralysis
- The "20-15-30 rule":
- FVC < 20 mL/kg → ICU admission
- FVC < 15 mL/kg → consider intubation
- MIP < -30 cmH2O → consider intubation
- Bulbar weakness → early intubation regardless of FVC
- Hypercarbia is a late and unreliable sign - do not wait for it
2. Hemodynamic Management (Low DBP)
- Avoid aggressive antihypertensives (labile BP in GBS - hypertension follows hypotension)
- For symptomatic hypotension: IV fluids cautiously, avoid vasoconstrictors unless refractory
- If wide pulse pressure + warm extremities + fever → think sepsis or beriberi (vasodilatory)
- IV thiamine 200-500 mg immediately if wet beriberi suspected (safe, therapeutic and diagnostic)
3. Treat the Underlying Cause
| Cause | Treatment |
|---|---|
| GBS | IVIG 2g/kg over 5 days OR plasmapheresis (5 exchanges over 2 weeks) - equivalent efficacy; steroids NOT recommended |
| Polio/Enteroviral AFM | Supportive; IVIG may help in some |
| Rabies | Milwaukee protocol (experimental); largely palliative if unvaccinated |
| Diphtheria | Antitoxin + penicillin/erythromycin |
| Tick paralysis | Remove tick - dramatic rapid recovery |
| Wet beriberi | IV thiamine 200-500 mg TDS |
| Organophosphate | Atropine + pralidoxime |
| Botulism | Antitoxin (heptavalent), supportive ventilation |
4. GBS-Specific ICU Management
- IVIG or plasmapheresis (no benefit to combining both)
- Cardiac monitoring (autonomic instability causes arrhythmias, sudden death)
- DVT prophylaxis (immobile patients)
- Nasogastric feeding if bulbar palsy
- Pain management (neuropathic pain with gabapentin, carbamazepine)
- Physiotherapy early
Step 6: Red Flags Requiring Immediate Action
- Rapid respiratory failure (FVC declining fast) → intubate, ICU
- Cardiac arrhythmia (autonomic GBS) → continuous cardiac monitoring, treat cause
- Bulbar palsy (dysphagia, dysarthria) → aspiration risk, early intubation
- Hypotension unresponsive to fluids → consider sepsis, beriberi, adrenal crisis
- Fever + pleocytosis on LP → treat empirically for bacterial meningitis/encephalitis while awaiting cultures
- Animal bite history → rabies post-exposure prophylaxis/isolation
Clinical Summary Algorithm
Ascending Paralysis + Fever + Low DBP
↓
1. Secure Airway (FVC monitoring) - FIRST
↓
2. Is paralysis TRULY ascending (legs first)?
├── Yes → GBS, polio, AFM, tick, beriberi, toxins
└── No (cranial nerves first) → Botulism, diphtheria (descending)
↓
3. Fever CHARACTER:
├── High fever + asymmetric + CSF pleocytosis → Polio/AFM/West Nile/Rabies
├── Low-grade + symmetric + areflexia + albuminocytological dissociation → GBS (infection trigger)
└── Fever + wide pulse pressure + heart failure signs → Wet beriberi (give thiamine NOW)
↓
4. Low DBP TYPE:
├── Vasodilatory (warm, bounding pulse, wide PP) → Sepsis, beriberi, GBS autonomic
└── Cardiogenic (cold, narrow PP) → Diphtheritic myocarditis, stress cardiomyopathy (GBS)
↓
5. KEY EXAM:
├── Find tick → REMOVE immediately
├── Pupil dilation → Botulism
├── Pseudomembrane throat → Diphtheria antitoxin
└── Animal bite → Rabies protocol
Sources:
- [Bradley and Daroff's Neurology in Clinical Practice, block28, p. 2663] - GBS diagnostic criteria and differential diagnosis
- [Adams and Victor's Principles of Neurology, 12th Ed, block15, p. 2070-2073] - GBS differential vs. polio, West Nile, tick paralysis
- [Miller's Anesthesia 10e, block33, p. 12034-12035] - GBS critical care, respiratory failure criteria, autonomic dysfunction
- [Goldman-Cecil Medicine, block56, p. 4063] - GBS autonomic dysfunction, labile BP
- [Tintinalli's Emergency Medicine, block15] - Poliomyelitis clinical features; clinical features of acute paralysis
- [Merck Manual Professional - GBS] - Differential: myasthenia, botulism, polio, tick, West Nile
- [Neurology.org clinical case] - Wet beriberi as ascending neuropathy with low DBP/heart failure
Minkxidil side effects, withdrawal, course for androgenetic alopecia
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
minoxidil androgenetic alopecia withdrawal shedding side effects duration of treatment 2024 2025
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Searching PubMed
minoxidil androgenetic alopecia efficacy safety
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer. Let me compile it.
Minoxidil for Androgenetic Alopecia (AGA): Complete Clinical Guide
Background & Mechanism
Androgenetic alopecia (AGA - male/female pattern hair loss) is the most common cause of hair loss in adults >40 years and can begin during puberty. In susceptible follicles, DHT binds androgen receptors, activating genes that gradually transform large terminal follicles into miniaturized vellus follicles.
Minoxidil (Rogaine) was the first FDA-approved drug for AGA. Originally developed as an antihypertensive, it gained attention for hair loss when oral users developed generalized hypertrichosis. Its exact mechanism on hair follicles is not fully understood, but involves:
- Opening of ATP-sensitive potassium channels in follicular cells
- Increases follicle size, resulting in thicker hair shafts
- Stimulates and prolongs the anagen (growth) phase of the hair cycle
- Increases the percentage of anagen follicles
- Increased proliferation of dermal papilla cells; decreased apoptosis in the germinative pool
Individual response variability is partly explained by differing levels of sulfotransferase enzyme activity within hair follicles - this enzyme catalyzes conversion to the active metabolite minoxidil sulfate. Aspirin may inhibit this activity and could theoretically reduce efficacy.
Minoxidil does not affect androgen production, excretion, or metabolism - it is not anti-androgenic.
Grading of AGA (Before Starting Treatment)
Male Pattern (Hamilton-Norwood, I-VII):
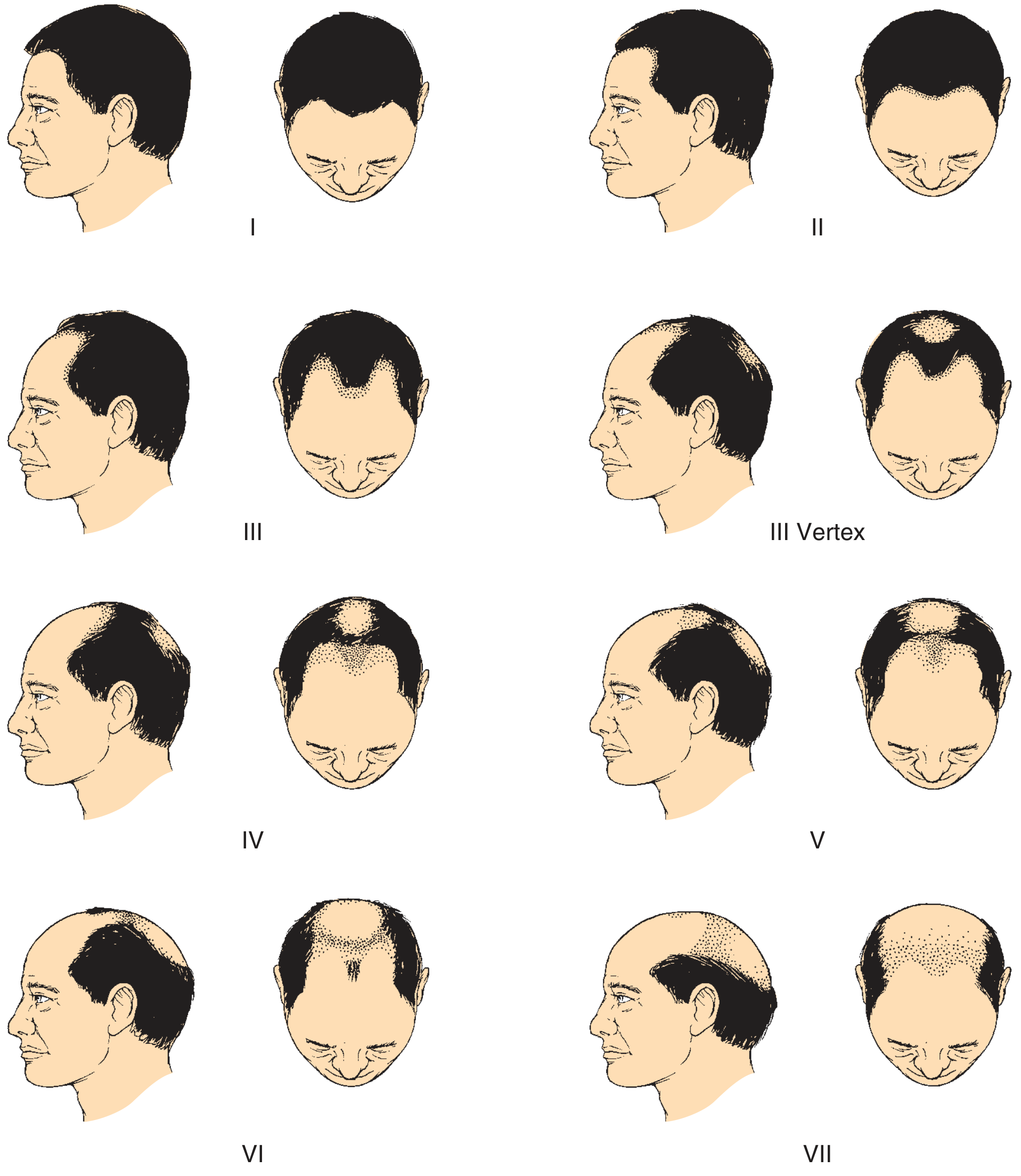
- Vertex balding responds better to minoxidil than frontal/hairline recession
- Norwood I-III: best candidates; IV-VII: limited benefit, may need surgical options
Female Pattern (Ludwig I-III / Sinclair 1-5):
- Diffuse thinning over the crown with preserved frontal hairline
- Ludwig I: mild widening of part; II: moderate; III: extensive thinning
Formulations, Doses, and Approved Use
| Formulation | Strength | Approved For | Notes |
|---|---|---|---|
| Topical solution | 2% | Men and women | Contains propylene glycol (more irritant) |
| Topical solution | 5% | Men (primary); women (off-label) | 45% more hair growth vs 2% at 48 weeks |
| Topical foam | 5% | Men and women | No propylene glycol - less irritant, better adherence |
| Oral (off-label) | 0.25-5 mg/day | Men and women | Emerging use; NOT FDA-approved for AGA |
Oral minoxidil doses (off-label, current evidence):
- Women: 0.625-2.5 mg/day (start low, e.g. 0.625 mg)
- Men: 0.625-5 mg/day (typically 2.5-5 mg)
- Also used for alopecia areata and chronic telogen effluvium in patients intolerant or unresponsive to topical form
Course of Treatment - Timeline
| Timepoint | What to Expect |
|---|---|
| Weeks 3-6 (onset) | "Shedding phase" - paradoxical increase in hair loss. This is normal - minoxidil pushes telogen hairs out to make way for new anagen hairs. Do NOT stop for this reason. |
| Months 3-4 | Shedding resolves; new anagen hairs begin emerging (often fine/short initially) |
| Months 4-6 | Visible improvement begins in responsive patients |
| Months 6-12 | Optimal assessment period; if no response by 12 months, reconsider |
| Peak effect | Typically at 1-2 years of continuous use |
| Ongoing | Maintenance phase - continued use required indefinitely |
"Vertex balding is more responsive to therapy than frontal balding. Chronic dosing studies have demonstrated that the effect of minoxidil is not permanent, and cessation of treatment will lead to hair loss in 4-6 months." - [Katzung's Basic and Clinical Pharmacology, 16th Ed, p.1690]
"Minoxidil-induced hair growth is commonly associated with shedding of telogen hairs and a paradoxical worsening of hair loss ~3 to 6 weeks following initiation of treatment. However, this resolves with continued treatment." - [Dermatology 2-Volume Set 5e, Ch.69]
Key principle: Minoxidil only works while it is being used. It does not alter the underlying genetic trajectory of AGA - it is not a cure.
Side Effects
Topical Minoxidil
| Side Effect | Detail |
|---|---|
| Initial shedding (telogen effluvium) | Weeks 3-6; normal; resolves spontaneously; do not stop |
| Allergic/irritant contact dermatitis | Most common; often due to propylene glycol in solution (switch to 5% foam which lacks propylene glycol) |
| Scalp pruritus | From vehicle irritation |
| Unwanted facial hypertrichosis | Cheeks/forehead from inadvertent spread; reversible on stopping |
| Systemic absorption | Minimal in normal scalp; possible hypotensive effect - monitor in cardiac disease patients |
Oral Minoxidil (Low-Dose, Off-Label)
| Side Effect | Frequency | Detail |
|---|---|---|
| Hypertrichosis | Most common | Unwanted hair on face (cheeks, forehead), arms, body. Greater risk with genetic predisposition for dark facial hair. In women, co-prescribing spironolactone may reduce this. |
| Facial/periorbital edema | Uncommon | Fluid retention; ankle edema |
| Postural/orthostatic hypotension | Uncommon | Especially at higher doses |
| Tachycardia | Uncommon | Reflex from vasodilation |
| Headache | Uncommon | |
| Pericarditis | Rare | Reported with oral use (uncommon at low doses) |
| Palpitations | Less frequent with sublingual vs oral (0% vs 9.3% in 2025 RCT) | |
| Fetal hypertrichosis | If used in pregnancy | Contraindicated in pregnancy and breastfeeding |
| Cardiac tamponade | Very rare case reports |
"Side effects of minoxidil include unwanted hypertrichosis of the cheeks or forehead, headache, ankle edema, and for topical preparations, allergic or irritant contact dermatitis... reported cardiovascular side effects from oral minoxidil (uncommon with low doses) include hypotension, tachycardia, and pericarditis." - [Dermatology 2-Volume Set 5e, Ch.157]
"The most common side effect with oral low-dose minoxidil is hypertrichosis. Additional potential side effects include postural hypotension, lower extremity edema, tachycardia, and headache." - [Goodman & Gilman's Pharmacological Basis of Therapeutics]
Withdrawal / Discontinuation
This is one of the most important counselling points for patients.
What Happens When You Stop
Minoxidil does not alter the natural course of AGA - it only temporarily supports hair growth. Upon stopping:
- Weeks 2-6 post-stop: Shedding begins as hairs supported by minoxidil enter the telogen phase simultaneously (synchronized effluvium)
- Months 3-6 post-stop: Visible thinning becomes apparent; shedding continues
- Months 6-12 post-stop: Hair density returns to pre-treatment baseline (or where it would have been with natural disease progression)
"Hair growth was lost when [minoxidil] was discontinued." - [Goodman & Gilman's]
"Treatment must be continued or any drug-induced hair growth will be lost." - [Katzung 16th Ed]
Key Points on Withdrawal
- There is no "rebound" worse than baseline - hair returns to where genetics would have taken it, plus any progression during treatment
- Severity of post-discontinuation shed varies by duration of use, age, and severity of underlying AGA
- Tapering (gradually reducing dose/frequency over 3-6 months) may reduce the severity of the shed, though no robust RCT data supports this
- Combining with finasteride or DHT blockers before stopping can help maintain some of the benefit
Practical Prescribing Guide
Application (Topical)
- Apply 1 mL (solution) or half-cap (foam) to dry scalp twice daily
- Targeted application to the affected area (vertex, mid-scalp)
- Wash hands thoroughly after application
- Avoid contact with eyes and non-scalp skin
- Allow to dry before going to bed (to prevent transfer to pillow/face)
Monitoring
- Cardiovascular monitoring in patients with cardiac disease (due to possible hypotension)
- Check for contact dermatitis after 2-4 weeks
- Reassess at 6 months; if no improvement at 12 months, discontinue or reassess
Pregnancy & Breastfeeding
- Contraindicated - fetal hypertrichosis reported; topical systemic absorption unlikely but risk not established
Comparison with Other AGA Treatments
| Drug | Mechanism | Evidence | Use |
|---|---|---|---|
| Minoxidil (topical) | K+ channel opener, anagen prolongation | Level 1 (FDA-approved) | Men and women |
| Finasteride 1 mg/day | 5α-reductase type II inhibitor → ↓ DHT | Level 1 (FDA-approved) | Men only (teratogenic) |
| Dutasteride 0.5 mg/day | Inhibits type I + II 5α-reductase | Level 1 (approved in some countries) | Men; higher efficacy than finasteride |
| Spironolactone 50-200 mg/day | Anti-androgen (aldosterone antagonist) | Off-label | Women with female pattern AGA; also reduces hypertrichosis from oral minoxidil |
| Low-dose oral minoxidil | Same as topical | Off-label, growing evidence | Those intolerant of topical or poor response |
| Microneedling + minoxidil | Enhances penetration, scalp wound healing | Emerging evidence (meta-analysis 2023) | Combination improves efficacy over topical alone |
"Patients are advised to allow at least 6 months before expecting to see a therapeutic effect. If they discontinue... the AGA will return to its pre-treatment appearance." - [Dermatology 2-Volume Set 5e, re: finasteride, same principle applies to minoxidil]
Summary for Patient Counselling
- Start: Expect initial shedding (weeks 3-6) - this is normal, continue treatment
- Wait: First visible benefit at 4-6 months; full assessment at 12 months
- Commit: Indefinite use required; stopping = reversal of benefit within 6-12 months
- Form matters: 5% foam preferred if scalp irritation occurs (no propylene glycol)
- Oral option: Useful if topical is inadequate or poorly tolerated; monitor for hypertrichosis, BP, edema
- Pregnancy: Stop before conception; breastfeeding contraindicated
- Combine: Finasteride + minoxidil provides complementary (additive) mechanisms in men
Sources:
- Cummings Otolaryngology Head and Neck Surgery, Ch. 22 - Medical Treatment of AGA
- Katzung's Basic and Clinical Pharmacology, 16th Ed, p.1690 - Minoxidil pharmacology
- Goodman & Gilman's Pharmacological Basis of Therapeutics - Androgenic Alopecia
- Dermatology 2-Volume Set 5e (Bolognia), Ch.69 (AGA) and Ch.157 (side effects)
- Frontiers in Pharmacology 2025 - Topical, oral, sublingual minoxidil review
- PubMed: PMID 37665358 - Minoxidil + microneedling meta-analysis (2023); PMID 40056230 - Combined microneedling vs topical minoxidil meta-analysis (2025)
This is a shared conversation. Sign in to Orris to start your own chat.