Ventilators modes
Reading File
Finding Sources
Searching PubMed
"mechanical ventilation" AND "ventilator modes"
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough overview of ventilator modes, drawn from Harrison's, Murray & Nadel's, and Sabiston's Surgery:
Ventilator Modes
Core Concept: The Four Basic Settings
Every ventilator mode controls four parameters:
- Breath size - tidal volume (VT) in volume-controlled modes, or inspiratory pressure in pressure-controlled modes
- Breath frequency - set rate (fully controlled) or patient-triggered (partial/full support)
- PEEP - positive end-expiratory pressure, always present in some form
- FiO2 - fraction of inspired oxygen
The "mode" determines which variables the clinician sets (independent) versus which ones the ventilator monitors (dependent). - Harrison's Principles of Internal Medicine 22e
Standard Modes
1. Assist-Control (AC) - Volume Control (VC-AC)
The most commonly used mode in ICU settings.
- Clinician sets: VT, respiratory rate (RR), PEEP, FiO2, inspiratory flow rate
- Monitored: peak airway pressure, plateau pressure, minute ventilation (VE)
- If the patient is apneic, the set RR is delivered. If the patient triggers extra breaths above the set rate, each patient-triggered breath still receives the full set tidal volume
- The dependent variable is airway pressure - this must be monitored carefully to avoid barotrauma
Advantages: Guaranteed minimum VT and VE; straightforward CO2 control
Disadvantages: Dyspneic patients may fight the set inspiratory flow, increasing work of breathing; high plateau pressures can cause barotrauma
Disadvantages: Dyspneic patients may fight the set inspiratory flow, increasing work of breathing; high plateau pressures can cause barotrauma
A key check: measure plateau pressure with an inspiratory hold (no flow = alveolar pressure isolated). Keep plateau pressure < 30 cmH2O. - Sabiston Textbook of Surgery
2. Assist-Control - Pressure Control (PC-AC)
- Clinician sets: inspiratory driving pressure, RR, PEEP, FiO2
- Monitored: tidal volume, VE
- Every breath (time-triggered or patient-triggered) raises airway pressure to the set level above PEEP; inhalation ends when inspiratory flow falls below a threshold
- VT is a dependent variable - it changes with lung compliance. If compliance worsens, VT drops; if compliance improves, VT rises
Advantages: Limits barotrauma (if patient effort is minimal); inspiratory flow is variable, which can improve patient comfort and synchrony
Disadvantages: No guarantee of VT or VE - must monitor closely; spontaneous respiratory effort can generate unexpectedly large VTs ("effort-dependent volume" risk)
Disadvantages: No guarantee of VT or VE - must monitor closely; spontaneous respiratory effort can generate unexpectedly large VTs ("effort-dependent volume" risk)
A paralyzed patient on PC-AC: the inspiratory driving pressure needed to reach a given VT equals the plateau pressure one would measure in VC-AC at that same VT. - Harrison's 22e
3. Pressure Support Ventilation (PSV)
The most widely used mode overall, analogous to a BiPAP machine.
- Clinician sets: inspiratory support pressure, PEEP, FiO2
- Monitored: VT, RR, VE
- Every breath is patient-triggered - no mandatory breaths. The ventilator delivers flow to reach the set pressure and cycles off when inspiratory flow drops to ~20% of peak flow (adjustable: 10-35%)
- Patients control their own RR, VT, and inspiratory time
- Used for weaning and in patients who are less sedated and able to participate in respiratory work
Advantages: Best synchrony with patient's neural respiratory effort; patients can control VT and timing
Disadvantages: Risk of apnea/hypoventilation if patient effort fails - must monitor RR, VT, and VE closely; no backup rate guarantee
Disadvantages: Risk of apnea/hypoventilation if patient effort fails - must monitor RR, VT, and VE closely; no backup rate guarantee
Cycling off matters: if the threshold is set too low (cycles late), patients begin exhaling against the ventilator (delayed cycling). If set too high (cycles early), breath ends before patient effort is complete (premature cycling). Waveform analysis confirms correct synchrony.
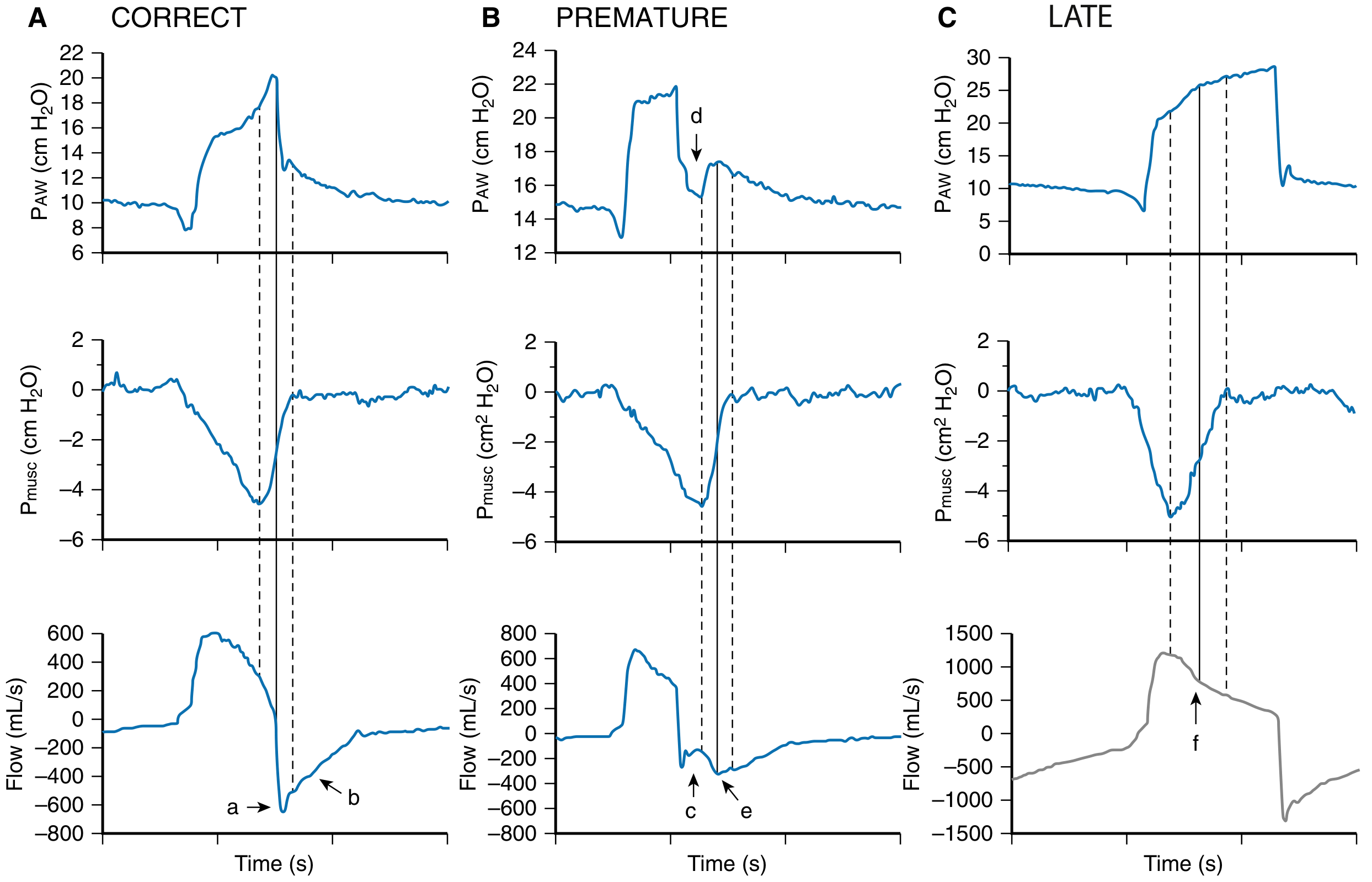
Waveform analysis of PSV cycling: (A) Correct - dashed lines mark patient effort start and end aligning with ventilator cycle. (B) Premature - ventilator cycles off before patient effort ends. (C) Late - ventilator continues into early expiration. - Murray & Nadel's Respiratory Medicine
4. Synchronized Intermittent Mandatory Ventilation (SIMV)
A hybrid of AC and PSV.
- Delivers a minimum guaranteed number of mandatory breaths (as VC or PC breaths)
- If the patient's RR exceeds the set rate, spontaneous breaths between mandatory breaths are either unassisted or supported by an added pressure support level (SIMV + PS)
- The key difference from AC: in AC, every patient-triggered breath gets a full mandatory breath; in SIMV, spontaneous breaths above the set rate are only partially supported (or unsupported)
Current status: Largely fallen out of favor. Evidence shows SIMV delays liberation from mechanical ventilation compared to PSV-based weaning. It is not recommended as a primary weaning strategy. - Murray & Nadel's
Summary Table (From Harrison's 22e)
| Mode | Clinician Sets | Monitored | Advantages | Disadvantages |
|---|---|---|---|---|
| AC-Volume Control | VT, RR, PEEP, FiO2, flow rate | Peak pressure, plateau pressure, VE | Guaranteed VT and VE | Barotrauma if plateau high; dyssynchrony |
| AC-Pressure Control | Driving pressure, RR, PEEP, FiO2 | VT, VE | Limits barotrauma; variable flow improves comfort | No VT guarantee; patient effort can cause large VT |
| Pressure-Regulated Volume Control | VT, RR, PEEP, FiO2 | Peak/plateau pressure, VE | Variable flow (comfort); guaranteed minimum VT | Variable effort can still exceed set VT |
| Pressure Support | Inspiratory pressure, PEEP, FiO2 | VT, RR, VE | Patient controls timing; best synchrony | Apnea/hypoventilation risk; no backup rate |
Advanced Modes
Pressure-Regulated Volume Control (PRVC)
A hybrid: pressure-targeted breath (like PC) but with VT as a feedback variable. The ventilator automatically adjusts the applied inspiratory pressure breath-to-breath to achieve the clinician-set VT. If compliance improves, the pressure drops; if compliance worsens, pressure rises. Also called "adaptive pressure ventilation" on some machines.
Volume Support (VS)
Like PSV but with automatic pressure adjustment to hit a target VT. Every breath is patient-triggered, pressure-targeted, flow-cycled - but the pressure target adjusts to maintain set VT.
Airway Pressure Release Ventilation (APRV)
- Applies a high CPAP level (P-High) for a prolonged time (T-High), then briefly releases to a low pressure (P-Low) for a short time (T-Low)
- Allows spontaneous breathing throughout the cycle
- The high pressure maintains alveolar recruitment; the brief release allows CO2 clearance
- Used in severe ARDS and reduced-compliance lungs where frequent derecruitment is a problem
- A recent meta-analysis of ~19 years of ARDS studies suggested a mortality benefit compared to conventional modes, though no difference in rescue maneuver need - Sabiston 14e
- Bilevel ventilation is similar to APRV but with a longer T-Low period
Adaptive Support Ventilation (ASV)
- The clinician sets only a desired minute ventilation and patient height (to estimate dead space)
- The ventilator calculates resistance, compliance, and expiratory time constant
- Automatically adjusts the frequency-VT pattern to minimize work of breathing and avoid air trapping
- Behaves like volume support when the patient is triggering
Proportional Assist Ventilation (PAV+) and Neurally Adjusted Ventilatory Assist (NAVA)
These modes deliver pressure in proportion to patient effort, addressing a key limitation of all other modes (where support is independent of effort):
- PAV+: Measures respiratory system elastance and resistance via end-inspiratory occlusions; delivers a set proportion of the total inflation pressure needed by the patient
- NAVA: Uses diaphragm EMG (via esophageal catheter electrodes) to sense diaphragmatic electrical activation and deliver pressure proportional to that signal
Both modes increase delivered pressure when the patient works harder, unloading respiratory muscles appropriately.
High-Frequency Oscillatory Ventilation (HFOV)
- Extremely low tidal volumes at very high frequencies (up to 15 Hz)
- Used as a salvage mode or bridge to ECMO in severe ARDS
- Despite theoretical appeal (ultra-low volume trauma), clinical trials in adults have not shown mortality benefit; may have a role in the pediatric population
Noninvasive Ventilation (NIV)
Delivered via nasal or full-face mask, without an endotracheal tube:
- CPAP: Single continuous positive pressure throughout the respiratory cycle; keeps alveoli open, improves oxygenation, reduces work of breathing in obstructive sleep apnea and cardiogenic pulmonary edema
- BiPAP: Two pressure levels - higher inspiratory positive airway pressure (IPAP) + lower expiratory positive airway pressure (EPAP). The pressure difference drives tidal volume
Best indications for NIV:
- COPD exacerbation with moderate hypercapnia (pH 7.25-7.35): reduces intubation need and hospital stay
- Acute cardiogenic pulmonary edema: rapid improvement with diuresis + BiPAP
- Chronic respiratory failure (scoliosis, neuromuscular disease): nocturnal NIV reduces admissions
Contraindications to NIV (requires secure airway instead): delirium, inability to manage secretions, hemodynamic instability - Harrison's 22e
Lung-Protective Ventilation Strategy (LPV)
Regardless of mode, the standard of care targets:
- VT: 6-8 mL/kg ideal body weight
- PEEP: 5-10 cmH2O
- Plateau pressure: < 30 cmH2O
- Driving pressure (plateau - PEEP): minimize, target < 15 cmH2O
- These parameters reduce ventilator-induced lung injury (VILI), especially in ARDS - Current Surgical Therapy 14e
This is a shared conversation. Sign in to Orris to start your own chat.