





+8 more
Viva questions on askin tumour left upper lung zone also give description
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Pancoast tumor" AND "superior sulcus"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from the textbooks. Let me compile the full viva answer.
Pancoast Tumour (Superior Sulcus Tumour) - Left Upper Lung Zone
Image Description
Image 1 - CXR (PA view): Left apical soft-tissue opacity in the left upper zone, slightly asymmetric compared to the right apex. This can be mistaken for apical pleural thickening - a key diagnostic pitfall.
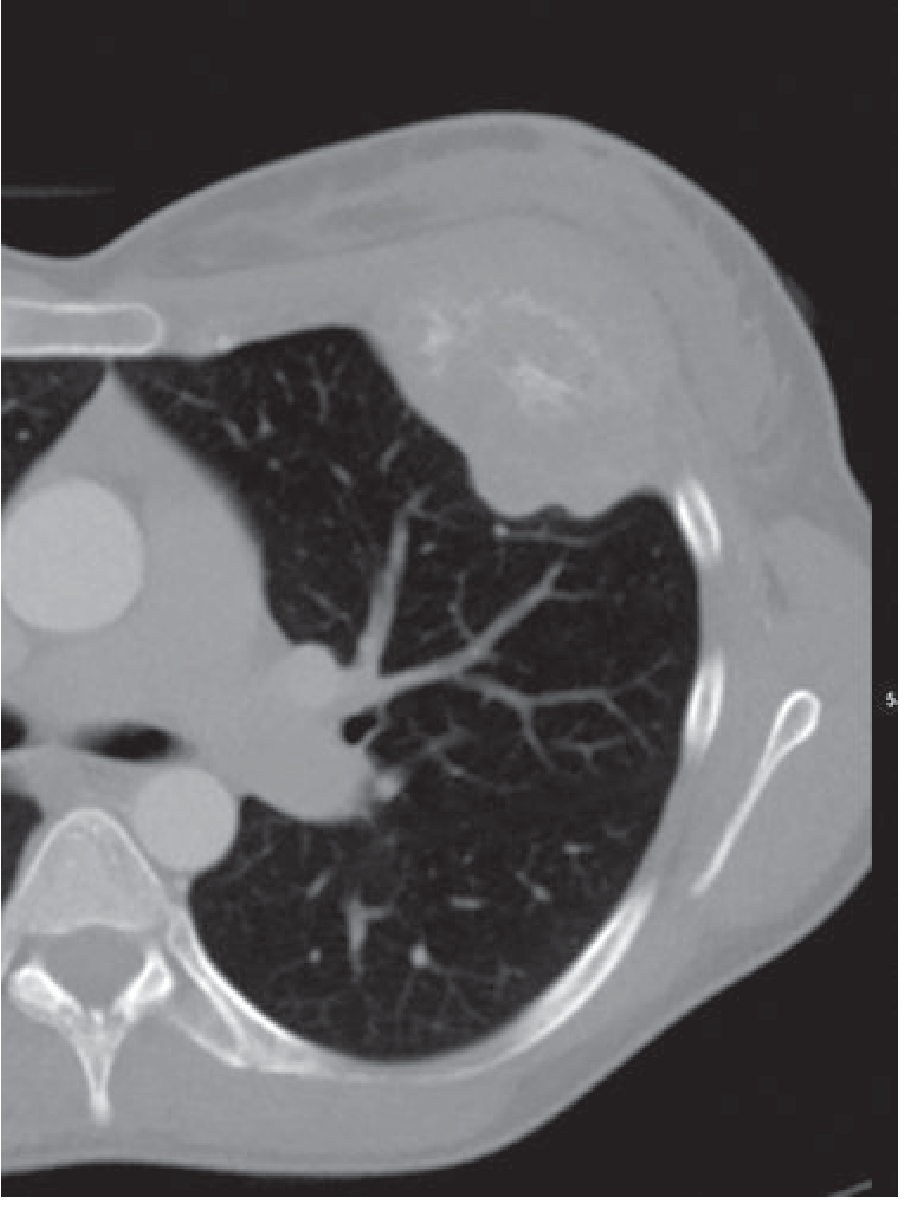
Image 2 - CT Axial (plain): Soft tissue mass in the left apical region abutting the chest wall, with apparent chest wall involvement. The mass occupies the superior sulcus region.
Image 3 - CT Coronal: Demonstrates the large left apical mass clearly. There is also visible involvement of surrounding structures. Note the right lung appears relatively clear.
Image 4 - CT Sagittal: Shows the left apical mass in the posterior sagittal plane with evidence of posterior chest wall and rib involvement.
Image 5 - PET (MIP): Two intensely FDG-avid foci are visible - one in the upper thorax (primary tumour) and one in the pelvis/lower abdomen (possible distant metastasis), indicating metabolically active disease at multiple sites.
Image 6 - PET-CT Fusion (Axial): The orange/yellow hot spot representing intense FDG uptake is co-localised to the left apical mass on CT, confirming this is a metabolically active malignancy - consistent with a Pancoast tumour.
VIVA QUESTIONS & ANSWERS
Q1. What is a Pancoast tumour?
A. A Pancoast tumour is a primary bronchogenic carcinoma arising from the extreme apex of the lung, at or above the first rib, involving the structures of the superior pulmonary sulcus. It was first described by Henry Pancoast in 1932. The designation is reserved for tumours involving the parietal pleura or structures overlying the first rib - chest wall involvement below the second rib does not qualify as a Pancoast tumour.
(Schwartz's Principles of Surgery, p. 1938; Murray & Nadel's Respiratory Medicine)
Q2. What is Pancoast Syndrome? List its components.
A. Pancoast syndrome is present in approximately one-third of patients with superior sulcus tumours. It is a constellation of:
| Feature | Mechanism |
|---|---|
| Shoulder and arm pain | Invasion of parietal pleura, brachial plexus, vertebral bodies, 1st-3rd ribs |
| Pain radiating along ulnar nerve distribution | C8, T1, T2 nerve root involvement |
| Horner's Syndrome (ptosis, miosis, anhidrosis, enophthalmos) | Invasion of paravertebral sympathetic chain and stellate ganglion |
| Weakness and atrophy of hand muscles | Lower brachial plexus involvement |
| SVC distension (face/neck/thorax veins) | Superior vena cava compression |
| Paraplegia (late) | Extension through intervertebral foramina causing spinal compression |
(Murray & Nadel's, p. 867-869; S. Das Manual of Clinical Surgery, p. 4291-4295)
Q3. What is the most common histological type?
A. The most common cause is Non-Small Cell Lung Cancer (NSCLC), which accounts for 85% of all lung cancers. Within NSCLC:
- Squamous cell carcinoma - historically most common type, closely correlated with smoking, tends to arise centrally but can be peripheral; may cavitate
- Adenocarcinoma - now the most common overall subtype, often peripheral in location
- SCLC and other tumour types can rarely present as Pancoast tumour
(Robbins Basic Pathology; Murray & Nadel's)
Q4. What are the radiological features on CXR?
A.
- Apical soft-tissue opacity or asymmetric apical cap (>5 mm asymmetry is suspicious)
- May mimic benign apical pleural thickening - the key differential
- Erosion of posterior aspects of the 1st, 2nd, or 3rd ribs
- Associated vertebral body destruction in advanced disease
- In some cases, the CXR may be normal - CT is then essential
- The typical spherical/oval shape of peripheral lung cancers may be absent here; the tumour may appear as an irregular apical mass
(Grainger & Allison's Diagnostic Radiology, p. 1629)
Q5. What is the role of CT, MRI, and PET-CT?
A.
CT:
- Confirms the apical mass, defines chest wall invasion
- Identifies other pulmonary nodules and mediastinal lymphadenopathy
- Helps stage the tumour
MRI (preferred for Pancoast):
- Superior to CT for evaluating invasion through pleura and subpleural fat
- Better evaluation of brachial plexus involvement
- Better definition of subclavian vessel involvement
- MR angiography gives the best assessment of vascular invasion of subclavian vessels
PET-CT (as in this case):
- Differentiates benign apical pleural caps from malignant Pancoast tumour
- Determines extent of metabolic activity
- Detects distant metastases
- Identifies residual disease or tumour relapse post-treatment
(Murray & Nadel's, p. 871; Grainger & Allison's PET/CT section)
Q6. How is Pancoast tumour staged?
A. Superior sulcus tumours are staged using the TNM system (NSCLC):
- T3N0M0 = Stage IIB (25% of cases in large series)
- Stage IIIA - approximately 22%
- Stage IIIB (T4 or N3) - approximately 53% (most common stage at presentation)
- One-third to one-half of all superior sulcus tumours have identifiable distant metastases at diagnosis
Poor prognostic factors:
- Weight loss
- Vertebral body or supraclavicular nodal involvement
- N1 or N2 nodal disease
- Incomplete resection
(Murray & Nadel's, p. 871)
Q7. How is tissue diagnosis obtained?
A.
- Flexible fiberoptic bronchoscopy - first-line diagnostic test; diagnostic yield ~50%
- TTNA (Transthoracic Needle Aspiration) - diagnostic yield >90%, even when bronchoscopy is non-diagnostic
- EBUS- or EUS-guided FNA for mediastinal/nodal staging
- Mediastinoscopy - required to exclude N2 disease; negative FNA alone is insufficient to confirm node-negative disease
Q8. What is the treatment of Pancoast tumour?
A. Treatment is multimodal and depends on staging:
For resectable disease (no mediastinal N2 involvement):
- Neoadjuvant chemoradiotherapy (concurrent cisplatin + etoposide + 45 Gy thoracic RT over 5 weeks) - current standard
- Surgical resection - en bloc thoracotomy with:
- Chest wall and vascular structure resection
- Anatomic lobectomy
- Portion of lower brachial plexus trunk
- Stellate ganglion resection
- Chest wall reconstruction if required
Results of the North American Intergroup Trial:
- Pathologic complete response in resected specimen: 66%
- 5-year OS: 44% overall; 54% for complete resection
- Brain is the most common relapse site
Contraindications to surgery:
- N2 mediastinal lymph node involvement
- T4 with N2 disease
- Subclavian artery encasement
For unresectable/advanced disease:
- Concurrent chemoradiotherapy followed by immunotherapy
- Palliative systemic therapy for metastatic disease
(Schwartz's Principles of Surgery, p. 1938-1945; Murray & Nadel's, p. 873)
Q9. What are the key differentials for an apical lung lesion?
A.
- Pancoast tumour (primary bronchogenic carcinoma)
- Apical pleural thickening (benign - bilateral, symmetrical)
- Apical tuberculosis (most common in Indian context - often cavitates, associated lymphadenopathy)
- Lymphoma
- Metastatic deposits
- Fibrous tumour of pleura
- Subclavian artery aneurysm
- Cervical rib
Q10. What are the paraneoplastic syndromes associated with lung cancer?
A. These are especially relevant with SCLC but can occur with any type:
| Syndrome | Mechanism |
|---|---|
| SIADH | Ectopic ADH (SCLC) |
| Cushing's syndrome | Ectopic ACTH (SCLC) |
| Hypercalcaemia | PTHrP secretion (squamous cell carcinoma) |
| Eaton-Lambert syndrome | Antibodies against voltage-gated Ca²⁺ channels (SCLC) |
| Peripheral neuropathy/encephalopathy | Paraneoplastic |
| Hypertrophic pulmonary osteoarthropathy | Periosteal new bone formation |
| Finger clubbing | |
| Acanthosis nigricans |
(Robbins Basic Pathology; Murray & Nadel's)
Q11. What structures can be invaded in a left-sided Pancoast tumour (as in this case)?
A. On the left side specifically:
- Left subclavian artery and vein
- Left brachial plexus (C8, T1, T2 roots)
- Left stellate ganglion -> Horner's syndrome
- Left recurrent laryngeal nerve -> hoarseness (wraps around the aortic arch on the left)
- T1-T2 vertebral bodies and intervertebral foramina
- 1st, 2nd, 3rd ribs and adjacent chest wall
- Left subclavian vein -> arm oedema
- Pericardium (advanced)
The left recurrent laryngeal nerve loops under the aortic arch, making hoarseness a more specific finding with left-sided apical tumours compared to the right side.
Q12. What is the relevance of PET-CT in staging (as shown in the images)?
A. The PET-CT in this case shows:
- Primary FDG-avid left apical mass confirming metabolically active malignancy
- Second FDG-avid focus in the lower abdomen/pelvis suggesting distant metastasis (M1 disease)
This has critical implications: if M1 disease is confirmed, the patient is Stage IV and surgery is contraindicated. The primary treatment would be systemic therapy (targeted if driver mutation present, immunotherapy if PD-L1 positive, or chemotherapy). PET-CT upstages or downstages approximately 20-30% of NSCLC patients compared to CT alone.
(Grainger & Allison's, PET/CT section; Murray & Nadel's)
Summary Box for Viva:
| Feature | Pancoast Tumour |
|---|---|
| Location | Extreme lung apex, superior sulcus, above 1st rib |
| Most common type | NSCLC (squamous cell / adenocarcinoma) |
| Classic triad | Shoulder/arm pain + Horner's + Hand muscle atrophy |
| Best imaging | MRI (chest) + PET-CT for staging |
| Stage at presentation | Usually IIIB (53%), IIB (25%), IIIA (22%) |
| Standard treatment | Neoadjuvant chemoRT -> Surgery (en bloc resection) |
| 5-year survival (complete resection) | ~54% |
| Most common relapse site | Brain |
Recent evidence: A 2025 systematic review (Langer et al., Lung Cancer - PMID 40651130) and a 2023 review of surgical approaches (Petrella et al., J Pers Med - PMID 37511781) continue to support multimodal neoadjuvant chemoradiotherapy followed by en bloc surgical resection as the standard of care for resectable Pancoast tumours.
Askin tumour imaging
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Askin tumor" OR "thoracopulmonary small cell tumor"
Searching the Web
Askin tumour imaging radiology CT MRI features thoracopulmonary
Reading File
Reading Web Page
https://appliedradiology.com/articles/askin-tumor
Reading File
Loading Image
Loading Image
I have the CT image from the textbook showing the Askin tumour (destructive anterior rib lesion with chest wall mass). Now I have all the information needed for a comprehensive answer.
Askin Tumour - Imaging
What is an Askin Tumour?
Askin tumour is a malignant small round cell tumour of the thoracopulmonary region arising from the chest wall, pleura, lung, or anterior mediastinum. It was first described by Frederic Askin in 1979 as a series of small round blue cell tumours originating in the soft tissues of the chest wall.
It is now classified as part of the Ewing Sarcoma Family of Tumours (ESFT), which includes:
- Ewing sarcoma (bone)
- Peripheral PNET (pPNET)
- Neuropithelioma
- Askin tumour (thoracopulmonary PNET)
All share the same cytogenetic hallmark: t(11;22)(q24;q12) - reciprocal translocation between chromosomes 11 and 22, producing the EWS-FLI1 fusion gene (rarely FUS-ERG translocation).
(Grainger & Allison's Diagnostic Radiology, p. 1377)
Who Gets It?
| Feature | Detail |
|---|---|
| Age | Children and young adults; most under 20 years |
| Peak | Second decade (10-20 years) |
| Sex | Male:Female = 1.4:1 (slight male predominance) |
| Ethnicity | 9x more common in Caucasians |
| Location | Chest wall, rib periosteum, pleura, lung, anterior mediastinum |
Imaging Modalities
1. Chest X-Ray (CXR)
- Large, poorly defined soft-tissue mass in the hemithorax
- May occupy an entire hemithorax
- Pleural-based opacity - can mimic a massive pleural effusion or empyema
- Rib destruction or splaying (may be absent in early cases)
- Ipsilateral pleural effusion - common
- Secondary lung atelectasis/collapse from mass effect
- The exact origin (chest wall vs. pleura vs. lung) is often indeterminate
2. CT (Chest) - Modality of Choice for Initial Assessment
This is the textbook CT image of an Askin tumour from Grainger & Allison's (Fig. 41.41):
Axial CT of the chest showing a destructive anterior rib lesion with associated soft-tissue chest wall mass - biopsy confirmed Ewing sarcoma/Askin tumour. - Grainger & Allison's Diagnostic Radiology
CT features:
| Feature | Detail |
|---|---|
| Mass | Large, heterogeneous soft-tissue mass - typically > 5 cm at presentation |
| Density | Heterogeneous attenuation due to necrosis, haemorrhage, cystic degeneration |
| Location | Pleural-based, chest wall, or combined intrathoracic + extrathoracic extension |
| Rib involvement | Rib erosion/destruction in 25-63% of cases; the underlying rib may be encased or destroyed |
| Pleural features | Pleural effusion (often large); nonuniform pleural thickening; enhancing nodular pleural deposits |
| Growth pattern | Solitary or multiple masses; eccentric growth along the chest wall |
| Calcification | Occasionally seen; dystrophic calcification within necrotic areas |
| Hydropneumothorax | Reported in some cases |
| Enhancement | Heterogeneous enhancement post-contrast; vascular enhancement indicates neoplastic hypervascularity |
| Metastases | Lung metastases (contralateral lung nodules) in advanced disease; lymphadenopathy |
| Intraspinal extension | Can extend through neural foramina - important to assess |
Key CT pearl: The site of origin is often difficult to determine precisely on CT - the tumour may appear to arise from the rib, intercostal soft tissues, parietal pleura, or peripheral lung simultaneously.
3. MRI - Best for Local Extent and Surgical Planning
| Sequence | Appearance |
|---|---|
| T1-weighted | Intermediate signal (similar to muscle); areas of haemorrhage appear bright (high T1) |
| T2-weighted / STIR | Intermediate to high signal; areas of necrosis appear very bright |
| Post-Gadolinium | Heterogeneous enhancement; vascular/neoplastic hypervascularity |
| Haemorrhage | High signal on both T1 and T2 (subacute haemoglobin) |
| Necrosis | Non-enhancing areas with high T2 signal |
MRI advantages over CT:
- Superior assessment of chest wall invasion depth
- Better delineation of brachial plexus/neurovascular bundle involvement
- Detects intraspinal/epidural extension through neural foramina
- Better characterises pleural vs. pulmonary origin
- Guides surgical planning for en bloc resection margins
4. PET-CT (FDG-PET)
- Askin tumours are intensely FDG-avid (hot masses) - similar to what you saw in the patient's PET-CT in the previous case
- Useful for:
- Confirming metabolic activity of primary tumour
- Staging - detecting distant bone, lung, and nodal metastases
- More sensitive than bone scintigraphy for osseous metastases
- Monitoring response to chemotherapy
- Detecting recurrence post-treatment
5. Bone Scintigraphy
- Historically used for staging
- Detects osseous metastases (present in <20% at diagnosis)
- Now largely superseded by FDG-PET and whole-body MRI, which are more sensitive
(Grainger & Allison's, p. 1398)
Imaging Summary Table
| Modality | Key Finding |
|---|---|
| CXR | Large pleural-based opacity ± rib destruction ± pleural effusion |
| CT | Heterogeneous chest wall mass, rib erosion (25-63%), pleural effusion, necrosis, extrathoracic extension |
| MRI | Intermediate T1 / high T2, haemorrhage, necrosis, gadolinium enhancement; best for local staging |
| PET-CT | Intensely FDG-avid; used for systemic staging and treatment response |
| Bone scan | Osseous metastases; largely replaced by PET |
Differential Diagnosis for a Large Chest Wall Mass in a Young Patient
- Ewing sarcoma of rib (overlaps significantly - same family)
- Pleuropulmonary blastoma (younger children, <6 years)
- Chondrosarcoma (calcified matrix; older adults)
- Lymphoma (mediastinal/hilar nodes more prominent; less rib destruction)
- Rhabdomyosarcoma (no specific rib erosion; younger patients)
- Mesothelial tumour/mesothelioma (older adults, asbestos history)
- Neuroblastoma (younger children, catecholamine secretion)
- Empyema necessitans (infective context; lenticular shape; ring enhancement)
Pathological Correlation (Why Imaging Looks Heterogeneous)
The heterogeneous CT/MRI appearance reflects:
- Necrosis (commonest - tumour outgrows its blood supply)
- Haemorrhage (highly vascular tumour)
- Cystic degeneration
- Viable tumour (soft-tissue attenuation islands)
On histology: small round blue cells with scanty cytoplasm, arranged in sheets or lobules; CD99 (MIC2) positive; PAS-positive glycogen granules.
Important Points for Viva
- No imaging findings are pathognomonic - tissue biopsy (percutaneous CT-guided) is always required
- CD99 (MIC2) is the most important immunohistochemical marker (positive)
- EWS-FLI1 translocation t(11;22) on molecular/cytogenetic analysis is confirmatory
- Overall prognosis is poor: <40% 2-year survival; metastatic disease at diagnosis worsens outcome significantly
- Treatment: multimodal - neoadjuvant chemotherapy + surgery (en bloc chest wall resection) + adjuvant chemoradiotherapy for localised disease; chemotherapy ± radiation for metastatic/unresectable disease
(Grainger & Allison's Diagnostic Radiology, p. 1377-1386; PMC8041657; Applied Radiology Askin tumour case report)
S1 mai pedicle hota hai
Reading File
Finding Sources
Finding Sources
Searching the Web
S1 sacral vertebra pedicle anatomy does S1 have pedicle radiology
Finding Sources
Finding Sources
Finding Sources
Searching the Web
S1 vertebra pedicle hota hai ya nahi sacrum anatomy hindi radiology viva
Bahut acchi information mili. Ab clearly answer deta hoon:
✅ Haan - S1 mein Pedicle HOTA HAI
Yeh ek common misconception hai. S1 vertebra mein pedicle present hota hai - lekin woh lumbar pedicles se anatomically alag hota hai.
S1 Pedicle ki Anatomy
Structure
S1 sacrum ka sabse upar ka vertebra hai (L5 ke neeche). Sacrum 5 sacral vertebrae (S1-S5) ke fusion se banta hai. S1 ke pedicles:
| Parameter | Measurement |
|---|---|
| Height / Width | ~20 mm height, ~10-11 mm width |
| Length | ~34-35 mm (lumbar pedicles se longer) |
| Medial angle | ~10-11 degrees |
S1 Pedicle, Lumbar Pedicles Se Kaise Alag Hai?
| Feature | Lumbar Pedicles (L1-L5) | S1 Pedicle |
|---|---|---|
| Shape | Tube-like, well-defined cortical ring | Short, high cancellous bone content, cortical ring absent/incomplete |
| Visibility on X-ray | Clearly visible as oval "eyes" (Scottie dog sign) | Medial aur superior border hi visible hoti hai; clearly defined nahi |
| Length | Variable (shorter higher up) | Longer (~35 mm) but lower cortical density |
| Lateral border | Well-corticated | Poorly defined, merges with sacral ala |
| Foramina | Intervertebral foramina flanking | Anterior + posterior sacral foramina |
Radiology Mein S1 Pedicle Kyun Important Hai?
1. Pedicle Screw Fixation (Surgical Relevance)
S1 pedicle screw placement lumbosacral fusion mein bahut common hai:
- Entry point: S1 superior facet ke inferior border se
- Trajectory: Promontory ki taraf aim karna (cranio-caudal angulation)
- Screw tricortical purchase zyada strong hoti hai (anterior + superior cortex breach)
- S1 screw loosening risk higher hota hai (~41%) because cortical ring absent hai
2. Pedicle on X-ray (Plain Film)
- Lumbar vertebrae mein AP view par pedicle oval "eye" shape mein dikh ta hai (Scottie dog ka eye = pedicle)
- S1 par pedicle clearly visible nahi hota standard AP view par - yahi confusion ka source hai
- Lekin CT scan par S1 pedicles clearly identifiable hain
3. Lumbosacral Junction (L5-S1)
- L5 ka pedicle S1 ke upar hota hai
- L5-S1 disc space ke foramen ke floor mein S1 pedicle contributes karta hai
- Wikipedia confirms: "They are attached to the body of the first sacral vertebra and to each ala, by short thick pedicles"
Scottie Dog Sign (Viva Point)
Lumbar oblique X-ray par "Scottie Dog" ke parts:
| Scottie Dog Part | Anatomical Structure |
|---|---|
| Nose | Transverse process |
| Eye | Pedicle |
| Ear | Superior articular process |
| Neck | Pars interarticularis |
| Body | Lamina |
| Front leg | Inferior articular process |
Yeh sign L1-L5 par clearly dikh ta hai. S1 par Scottie dog nahi dikhta - isliye logon ko lagta hai ki S1 mein pedicle nahi hota.
Summary (Viva ke liye)
"S1 mein pedicle HOTA HAI, lekin woh lumbar pedicles se structurally alag hai. S1 pedicle short, cancellous-rich aur poorly corticated hota hai, isliye plain X-ray par clearly visible nahi hota. CT par clearly identify hota hai. Surgically, S1 pedicle screw lumbosacral fusion mein routinely use hota hai with trajectory aimed toward the sacral promontory."
Confusion ka source: Plain AP radiograph par L1-L5 ke pedicles oval eyes ki tarah dikh te hain, lekin S1 ka pedicle sacrum ke fusion aur ala ke overlap ki wajah se plain film par visible nahi hota - isliye yeh myth chal ta hai ki S1 mein pedicle nahi hota. CT se clearly confirm hota hai ki hota hai.
This is a shared conversation. Sign in to Orris to start your own chat.