Panophthalmitis case presentation for residency notes and answers to viva questions ophthalmology
Reading File
Finding Sources
Finding Sources
Searching the Web
panophthalmitis ophthalmology residency viva questions case presentation clinical features management
Reading File
Reading Web Page
https://eyewiki.org/Panophthalmitis
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
I now have comprehensive information to compile a complete, high-quality residency case presentation and viva Q&A. Let me compile this now.
Panophthalmitis - Residency Case Presentation & Viva Q&A
CASE PRESENTATION
Chief Complaint
A 45-year-old male farmer presents with severe pain, redness, and progressive loss of vision in the right eye for 3 days, following a penetrating injury by a wooden stick 5 days ago.
History of Present Illness
- 5 days ago: sustained penetrating injury to the right eye with a wooden stick while working in the field
- Initially treated at a local clinic with topical antibiotics and discharged
- Over the next 48 hours: pain worsened dramatically, eye became progressively red, swollen eyelids developed, and vision dropped to only light perception
- Associated features: fever (38.8°C), headache, nausea, inability to move the eye (painful ophthalmoplegia)
- No history of similar episodes; no known systemic illness
Past History
- No prior ocular surgery or trauma
- No diabetes mellitus, hypertension, or immunosuppressive conditions
- No drug allergies
Examination Findings
General: Febrile (38.8°C), mildly toxic-looking
Systemic: No cardiac murmurs; no focal neurology
Ocular Examination - Right Eye:
| Parameter | Findings |
|---|---|
| Visual Acuity | Light perception only |
| Eyelids | Severe edema, erythema, unable to fully open |
| Conjunctiva | Massive chemosis, intense conjunctival injection |
| Cornea | Edematous, hazy, corneal opacity with wound track visible |
| Anterior Chamber | Hypopyon (3 mm), AC flare 4+ |
| Iris | Muddy, congested; pupil sluggish |
| Lens | Hazy; red reflex absent |
| Extraocular motility | Complete ophthalmoplegia; pain on any attempted movement |
| IOP | Low (4 mmHg by Tonopen) |
| Proptosis | Present (3 mm by Hertel exophthalmometry) |
| B-scan ultrasound | Dense vitreous echoes; choroidal thickening; retinal detachment; T-sign (fluid in sub-Tenon space) |
Left Eye: Normal; VA 6/6; no inflammation
Investigations
| Investigation | Result |
|---|---|
| CBC | Leukocytosis - WBC 17,000/mm³ with neutrophilia |
| Blood cultures | Sent (x2) |
| Blood glucose | 6.8 mmol/L (normal) |
| CRP/ESR | Elevated |
| CT orbit (axial + coronal) | Proptosis, extrascleral extension of inflammation, orbital fat stranding; no foreign body on CT (wooden - radiolucent) |
| MRI orbit | Better delineation of soft tissue involvement; wooden foreign body may be identified as hypointense signal void |
| Vitreous tap (if performed before evisceration) | Gram-positive cocci in clusters (Staphylococcus sp.) |
Diagnosis
Right eye Panophthalmitis (exogenous, post-traumatic) secondary to penetrating injury with organic foreign body (wood).
Management
1. Immediate Stabilization:
- IV access, IV fluids, analgesics
- Blood and wound cultures before antibiotics
2. Systemic Antibiotics (IV):
- Vancomycin 1 g IV q12h (Gram-positive coverage, including MRSA)
- Ceftazidime 2 g IV q8h (Gram-negative coverage)
- Consider adding metronidazole if anaerobic contamination suspected (organic matter)
- Moxifloxacin 400 mg IV/oral can achieve therapeutic vitreous levels and may be used as adjunct
3. Intravitreal Antibiotics (before evisceration if vision salvage attempted):
- Vancomycin 1 mg/0.1 mL + Ceftazidime 2.25 mg/0.1 mL intravitreal
- Intravitreal dexamethasone 0.4 mg/0.1 mL (select severe cases)
4. Surgical Management:
Given the extent of disease (proptosis, complete ophthalmoplegia, no vision, orbital involvement), evisceration was performed.
- Evisceration preferred over enucleation in panophthalmitis:
- Shorter operating time
- Intact scleral shell allows better orbital implant retention, good cosmesis
- Better prosthetic mobility
- Pre-op CT/MRI must exclude scleral abscess (if present, enucleation preferred)
- Specimen sent for histopathology and microbiology
5. Post-operative:
- Continue IV antibiotics for 2 weeks, then oral completion
- Daily wound care, regular follow-up
- Prosthetic fitting after 6-8 weeks
Outcome
- Systemic infection controlled
- Evisceration specimen: suppurative pan-necrotic inflammation involving all ocular coats
- Culture: Staphylococcus aureus (MSSA)
- Antibiotics de-escalated to beta-lactam per sensitivity
- Prosthesis fitted at 8 weeks; good cosmetic outcome
PATHOLOGICAL CORRELATE
From Robbins & Cotran Pathologic Basis of Disease:
"Panophthalmitis is applied to eye inflammation involving the retina, choroid, and sclera extending into the orbit."
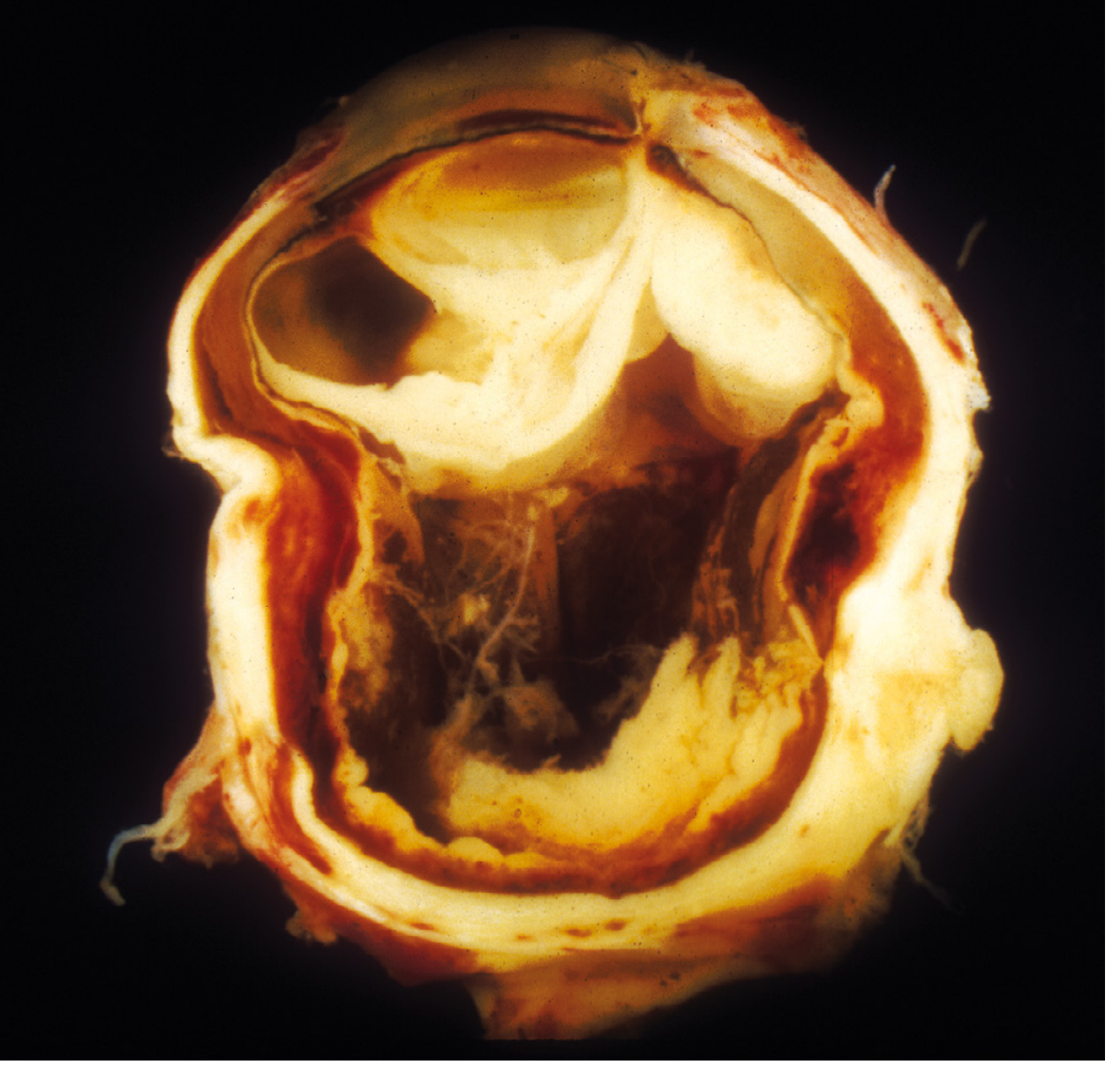
Fig. 29.16 (Robbins) - Exogenous panophthalmitis. Eye removed after foreign body injury. Suppurative inflammation of the entire orbit has distorted the globe architecture.
VIVA QUESTIONS & ANSWERS
Q1. Define Panophthalmitis. How does it differ from Endophthalmitis?
Endophthalmitis is suppurative inflammation of the interior of the eye (vitreous + aqueous chambers), not extending beyond the sclera.
Panophthalmitis is suppurative inflammation involving all coats of the globe (cornea, iris, lens, vitreous, retina, choroid, and sclera) with extension into the orbit and periorbital structures - effectively endophthalmitis + orbital cellulitis.
A simple mnemonic: Pano = Pan (all) - all structures including sclera and orbit.
(Robbins & Cotran Pathologic Basis of Disease)
Q2. What are the routes of infection in Panophthalmitis?
Exogenous:
- Penetrating trauma (most common cause, especially organic matter - wood, vegetable)
- Post-operative: post-cataract, post-glaucoma surgery (bleb-related), post-vitrectomy, post-intravitreal injection
- Perforated corneal ulcer
- Filtering bleb infection
Endogenous (hematogenous):
- Sepsis/bacteremia (endocarditis, UTI, pneumonia)
- IV drug abuse (Candida, S. aureus)
- Immunocompromised states: diabetes mellitus, HIV, transplant patients
- Common endogenous organisms: Klebsiella (especially in East Asian patients with liver abscess), E. coli, Candida
(EyeWiki; Wills Eye Manual)
Q3. What organisms typically cause Panophthalmitis?
Bacteria (most common - exogenous):
- Staphylococcus aureus (post-traumatic; most common gram-positive)
- Streptococcus species (bleb-associated - very virulent)
- Pseudomonas aeruginosa (gram-negative; post-operative)
- Bacillus cereus - particularly devastating post-traumatic (soil/organic matter contamination); rapid onset, often requires evisceration within 24-48 hours
- Gram-negative rods (Klebsiella, E. coli) in endogenous cases
Fungi:
- Aspergillus (exogenous, esp. immunocompromised)
- Candida (endogenous, IV drug users, immunocompromised)
- Rhizopus (mucormycosis - orbital involvement, diabetics)
Viruses:
- HSV, VZV (herpetic panophthalmitis)
- Dengue virus
Q4. What is the clinical presentation of Panophthalmitis?
Symptoms:
- Severe ocular pain (much worse than endophthalmitis)
- Pain on extraocular movement
- Rapidly decreasing vision (may reach no light perception)
- Photophobia
- Headache, fever, malaise
- Nausea/vomiting
Signs (anterior segment):
- Lid edema and erythema
- Chemosis (massive)
- Conjunctival injection / purulent discharge
- Corneal edema, opacity
- Hypopyon
- Hazy AC, anterior uveitis
Signs (posterior/orbital):
- Absent red reflex
- Vitreous exudate
- Proptosis
- Ophthalmoplegia (partial or complete)
- Afferent pupillary defect (APD)
- Reduced or elevated IOP
- Perforated globe (in severe cases)
Systemic:
- Fever, leukocytosis
(EyeWiki; Wills Eye Manual)
Q5. What investigations would you order?
Ocular:
- B-scan ultrasonography - dense vitreous echoes, choroidal thickening, sub-Tenon fluid ("T-sign"), retinal detachment
- Vitreous tap - Gram stain, culture (blood agar, chocolate, Sabouraud, thioglycolate), Giemsa stain
- AC paracentesis - if vitreous tap not possible
Systemic:
4. CBC with differential (leukocytosis)
5. Blood cultures x2 (before antibiotics)
6. CRP, ESR
7. Blood glucose (screen for diabetes)
8. Renal and liver function tests
Imaging:
9. CT orbit - proptosis, extrascleral spread, foreign body (metal/dense), orbital involvement; note: wooden foreign bodies are radiolucent on CT
10. MRI orbit - better for soft tissue; wooden FB appears as hypointense signal void; detects meningeal involvement
Q6. What is the T-sign on B-scan?
The T-sign on B-scan ultrasonography is a characteristic appearance of sub-Tenon fluid accumulation seen in panophthalmitis (and posterior scleritis). The fluid between the Tenon's capsule and sclera creates an echo-free space posterior to the globe that forms a "T"-shape with the optic nerve shadow on cross-section.
It indicates fluid in the episcleral/sub-Tenon space, signifying extension of inflammation/infection beyond the globe - an important pointer to panophthalmitis rather than simple endophthalmitis.
Q7. What is the Endophthalmitis Vitrectomy Study (EVS)? What are its key findings?
The EVS (1995) was a landmark prospective RCT studying management of post-cataract extraction bacterial endophthalmitis.
Key findings:
- Immediate vitrectomy benefited patients with LP (light perception) vision only - significantly better visual outcomes compared to vitreous tap + antibiotics alone
- For patients with HM (hand movements) or better vision, immediate vitrectomy offered no benefit over vitreous tap + inject
- Systemic (IV) amikacin + ceftazidime added no benefit over intravitreal therapy alone in this setting
Important caveat: EVS was specific to post-cataract endophthalmitis. Its results should NOT be directly extrapolated to panophthalmitis, traumatic endophthalmitis, or endogenous endophthalmitis.
(Wills Eye Manual p. 997-999)
Q8. What are the intravitreal antibiotics used and their doses?
| Drug | Dose | Coverage |
|---|---|---|
| Vancomycin | 1 mg / 0.1 mL | Gram-positive (incl. MRSA, Strep) |
| Ceftazidime | 2.25 mg / 0.1 mL | Gram-negative |
| Amikacin | 0.4 mg / 0.1 mL | Gram-negative (if penicillin allergy) |
| Voriconazole | 100 mcg / 0.1 mL | Fungal |
| Amphotericin B | 5-10 mcg / 0.1 mL | Fungal |
| Dexamethasone | 0.4 mg / 0.1 mL | Anti-inflammatory (select cases) |
Note: Vancomycin + Ceftazidime covers most gram-positive and gram-negative organisms empirically.
(Wills Eye Manual - Appendix 12; p. 4946)
Q9. Evisceration vs. Enucleation vs. Exenteration - when is each preferred?
| Procedure | Description | Indication in Panophthalmitis |
|---|---|---|
| Evisceration | Removal of intraocular contents; scleral shell preserved | Preferred for panophthalmitis - shorter time, better cosmesis, lower implant extrusion, better prosthetic mobility |
| Enucleation | Removal of entire globe | If scleral abscess present on imaging (infection extends to sclera making evisceration unsafe); sympathetic ophthalmia concern |
| Exenteration | Removal of globe + orbital contents | If orbital extension with spreading necrotizing fasciitis; mucormycosis; malignancy |
Pre-operative rule: Always obtain CT/MRI before evisceration - if scleral abscess is detected, enucleation is preferred to ensure complete removal of infected tissue.
Sympathetic ophthalmia: A theoretical concern with evisceration (residual uveal tissue); however, clinical evidence is limited. Risk must be weighed against surgical morbidity.
(EyeWiki; Wills Eye Manual)
Q10. What are the complications/sequelae of Panophthalmitis?
Ocular:
- Permanent vision loss (most common)
- Phthisis bulbi (shrunken, atrophic eye)
- Corneal perforation
- Retinal detachment
Orbital/Systemic (severe cases - untreated):
- Orbital cellulitis / abscess
- Cavernous sinus thrombosis (life-threatening)
- Meningitis / Encephalitis
- Cerebral abscess
- Sepsis
- Death (rare with modern treatment)
(EyeWiki)
Q11. What is Bacillus cereus endophthalmitis - why is it special?
Bacillus cereus is notorious for causing rapid and devastating post-traumatic endophthalmitis/panophthalmitis, characteristically associated with:
- Soil or organic matter contamination (agricultural injuries)
- IV drug users (Bacillus grows in contaminated drugs)
- Ring abscess of the cornea
- Progression to no light perception within 24-48 hours
- Toxin production (cereolysin, phospholipase C) causes rapid intraocular destruction
Management is aggressive - early evisceration is often necessary even with antibiotics. Vancomycin is the drug of choice; Bacillus is resistant to cephalosporins.
Q12. What is the role of steroids in Panophthalmitis?
Steroids are adjunctive - they reduce the destructive inflammatory cascade but must not be used until infection is sterilized/controlled:
- Intravitreal dexamethasone (0.4 mg/0.1 mL): given with intravitreal antibiotics in severe cases to reduce vitritis
- Oral prednisone (60 mg/day for 5 days): used in EVS protocol 24-48h after antibiotics; reduces postinfectious inflammation but final visual outcome unchanged
- Topical steroids + cycloplegics: once infection controlled, to manage post-infectious uveitis
Do NOT use steroids before confirming bacterial control - risk of fungal superinfection and masking of progressive infection.
(Wills Eye Manual p. 4946-4973)
Q13. How do you differentiate Panophthalmitis from Orbital Cellulitis clinically?
| Feature | Panophthalmitis | Orbital Cellulitis |
|---|---|---|
| Primary involvement | Intraocular (endophthalmitis + orbital) | Orbital fat/preseptal only |
| Proptosis | Yes | Yes |
| Ophthalmoplegia | Yes (with severe pain) | Yes |
| Hypopyon | Present (intraocular sign) | Absent |
| Absent red reflex | Yes | No |
| Vitreous opacity on B-scan | Yes | No |
| Vision loss | Severe/profound | Mild-moderate |
| Source | Ocular (trauma, surgery, ulcer) or endogenous | Sinus (ethmoiditis), dental, skin |
Q14. What are the differences between exogenous and endogenous endophthalmitis?
| Feature | Exogenous | Endogenous |
|---|---|---|
| Route | Direct inoculation (trauma, surgery, ulcer) | Hematogenous spread |
| Laterality | Unilateral | Bilateral (up to 25%) |
| Common organisms | Staph, Strep, Pseudomonas, Bacillus | Klebsiella, Candida, Staph aureus |
| Common setting | Post-surgical, post-traumatic | Diabetes, immunocompromised, IV drug use, endocarditis |
| Onset | Often acute | Variable |
| Systemic workup | Less critical | Critical (search for source) |
Q15. What is the prognosis of Panophthalmitis?
The visual prognosis is generally poor, even with prompt treatment. Key prognostic factors:
Poor prognostic indicators:
- Virulent organisms (Bacillus cereus, Streptococcus)
- Delay in presentation/treatment
- Presence of RAPD at presentation
- Initial vision of light perception or no light perception
- Immunocompromised state (diabetes, HIV)
- Orbital extension
Systemic prognosis is good with modern antibiotics - mortality is rare except with:
- Cavernous sinus thrombosis
- Fulminant meningitis
- Uncontrolled sepsis
(EyeWiki; Wills Eye Manual; Robbins & Cotran Pathologic Basis of Disease)
QUICK REVISION SUMMARY TABLE
| Domain | Key Points |
|---|---|
| Definition | All coats of globe + orbital extension (endophthalmitis + orbital cellulitis) |
| Most common cause | Penetrating trauma (exogenous); Sepsis (endogenous) |
| Worst organism | Bacillus cereus (rapid destruction, 24-48h) |
| Key sign | Absent red reflex + proptosis + ophthalmoplegia + hypopyon |
| Key investigation | B-scan (T-sign), vitreous culture, CT/MRI orbit |
| Intravitreal Rx | Vancomycin 1mg + Ceftazidime 2.25mg |
| Surgical Rx | Evisceration (preferred); Enucleation if scleral abscess |
| Do NOT | Eviscerate if scleral abscess present (do enucleation instead) |
| EVS study | Vitrectomy for LP vision post-cataract only |
| Complications | Cavernous sinus thrombosis, meningitis, sepsis, death |
| Prognosis | Visual prognosis poor; systemic prognosis good with treatment |
Sources:
- Robbins, Cotran & Kumar - Pathologic Basis of Disease (10th ed.), Ch. 29 "Acute Intraocular Inflammation: Retinitis, Endophthalmitis, and Panophthalmitis," p. 1199/1216
- The Wills Eye Manual (Office and Emergency Room Diagnosis), Section 12.13 Postoperative Endophthalmitis, pp. 997-999
- EyeWiki - Panophthalmitis (AAO)
Generate a summary comparison table of endophthalmitis vs panophthalmitis
Based on everything covered in the previous session, here is the comprehensive comparison table:
Endophthalmitis vs Panophthalmitis — Summary Comparison Table
| Feature | Endophthalmitis | Panophthalmitis |
|---|---|---|
| Definition | Suppurative inflammation of the interior of the eye (vitreous ± aqueous); confined within the scleral coat | Suppurative inflammation of all coats of the globe (cornea, iris, lens, vitreous, retina, choroid, sclera) with orbital/periorbital extension |
| Extent of involvement | Intraocular only (anterior chamber + vitreous) | All ocular coats + orbit = endophthalmitis + orbital cellulitis |
| Scleral involvement | No | Yes - hallmark distinguishing feature |
| Orbital involvement | No | Yes (proptosis, ophthalmoplegia) |
| Severity | Severe | More severe / devastating |
| Pain | Significant | Excruciating; far worse |
| Proptosis | Absent | Present |
| Ophthalmoplegia | Absent | Present (partial or complete) |
| Chemosis | Mild-moderate | Massive |
| Eyelid edema | Mild | Severe, may prevent eye opening |
| Hypopyon | Present | Present |
| Absent red reflex | Present | Present |
| Vitreous opacity | Present | Present |
| T-sign on B-scan | Absent | Present (sub-Tenon fluid - key sign) |
| Proptosis on CT/MRI | Absent | Present; orbital fat stranding |
| Fever / leukocytosis | May be present (endogenous) | Usually present |
| Common causes | Post-operative (cataract, vitrectomy, intravitreal injection), perforated corneal ulcer, bleb-related, hematogenous | Penetrating trauma (esp. organic foreign body), severe post-operative, severe corneal perforation, endogenous sepsis |
| Worst organism | Streptococcus (bleb-related), Bacillus cereus | Bacillus cereus (destruction in 24-48h) |
| Endogenous route | Yes (Klebsiella, Candida, S. aureus) | Yes (same; more advanced disease) |
| Key investigation | B-scan US + vitreous tap + culture | B-scan (T-sign) + CT/MRI orbit + vitreous tap + blood cultures |
| Medical treatment | Intravitreal vancomycin 1 mg + ceftazidime 2.25 mg ± systemic antibiotics | IV vancomycin + ceftazidime (systemic) + intravitreal antibiotics |
| EVS study applicability | Yes - post-cataract endophthalmitis (vitrectomy for LP vision) | No - EVS does NOT apply |
| Surgical treatment | Vitreous tap + inject; Pars plana vitrectomy (PPV) | Evisceration (preferred) or enucleation |
| Evisceration | Not indicated | First-line surgical option |
| Enucleation | Rarely needed | Indicated if scleral abscess present on imaging |
| Exenteration | Not indicated | Reserved for orbital necrotizing fasciitis, mucormycosis |
| Pre-surgical imaging | Optional | Mandatory (CT/MRI to exclude scleral abscess before planning evisceration) |
| Sympathetic ophthalmia risk | Evisceration: theoretical concern | Same theoretical concern; weigh against surgical morbidity |
| Visual prognosis | Guarded to poor (depends on organism and timing) | Poor; often no useful vision salvageable |
| Systemic complications | Rare | Cavernous sinus thrombosis, meningitis, encephalitis, sepsis, death |
| Mortality | Rare | Rare but possible with cavernous sinus thrombosis or sepsis |
| Pathology (Robbins) | Inflammation of vitreous humor interior | Inflammation extending into uvea, sclera, and orbit |
Key "One-Line" Distinctions
- Scleral involvement = the line that separates endophthalmitis from panophthalmitis
- T-sign on B-scan = sub-Tenon fluid = panophthalmitis (not endophthalmitis)
- Proptosis + ophthalmoplegia + hypopyon together = panophthalmitis until proven otherwise
- Evisceration is the surgical answer for panophthalmitis; vitrectomy is the surgical answer for endophthalmitis
- EVS applies to endophthalmitis only - never extrapolate to panophthalmitis
Sources: Robbins & Cotran Pathologic Basis of Disease (10th ed.); The Wills Eye Manual; EyeWiki (AAO)
This is a shared conversation. Sign in to Orris to start your own chat.