Introduction to hemodynamic and electrophysiology of heart
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive content from the textbooks. Let me compose the full response.
Introduction to Hemodynamics and Electrophysiology of the Heart
PART 1: CARDIAC ELECTROPHYSIOLOGY
1.1 Overview
Cardiac electrophysiology encompasses all processes involved in the electrical activation of the heart: the cardiac action potentials, conduction of those potentials along specialized tissues, excitability and refractory periods, autonomic modulation of heart rate and conduction velocity, and the ECG.
The ultimate purpose of this electrical activity is mechanical: the ventricles must be electrically activated and then contract. Sequence is everything - the atria must activate before the ventricles, and the ventricles must contract apex to base for efficient blood ejection. - Costanzo Physiology 7th Edition, p. 137
1.2 Cardiac Conducting System
The heart contains two types of muscle cells:
- Contractile cells - the working muscle of atria and ventricles; generate force and pressure
- Conducting cells - specialized muscle cells (SA node, internodal tracts, AV node, Bundle of His, Purkinje fibers) that spread action potentials rapidly without contributing significantly to force generation
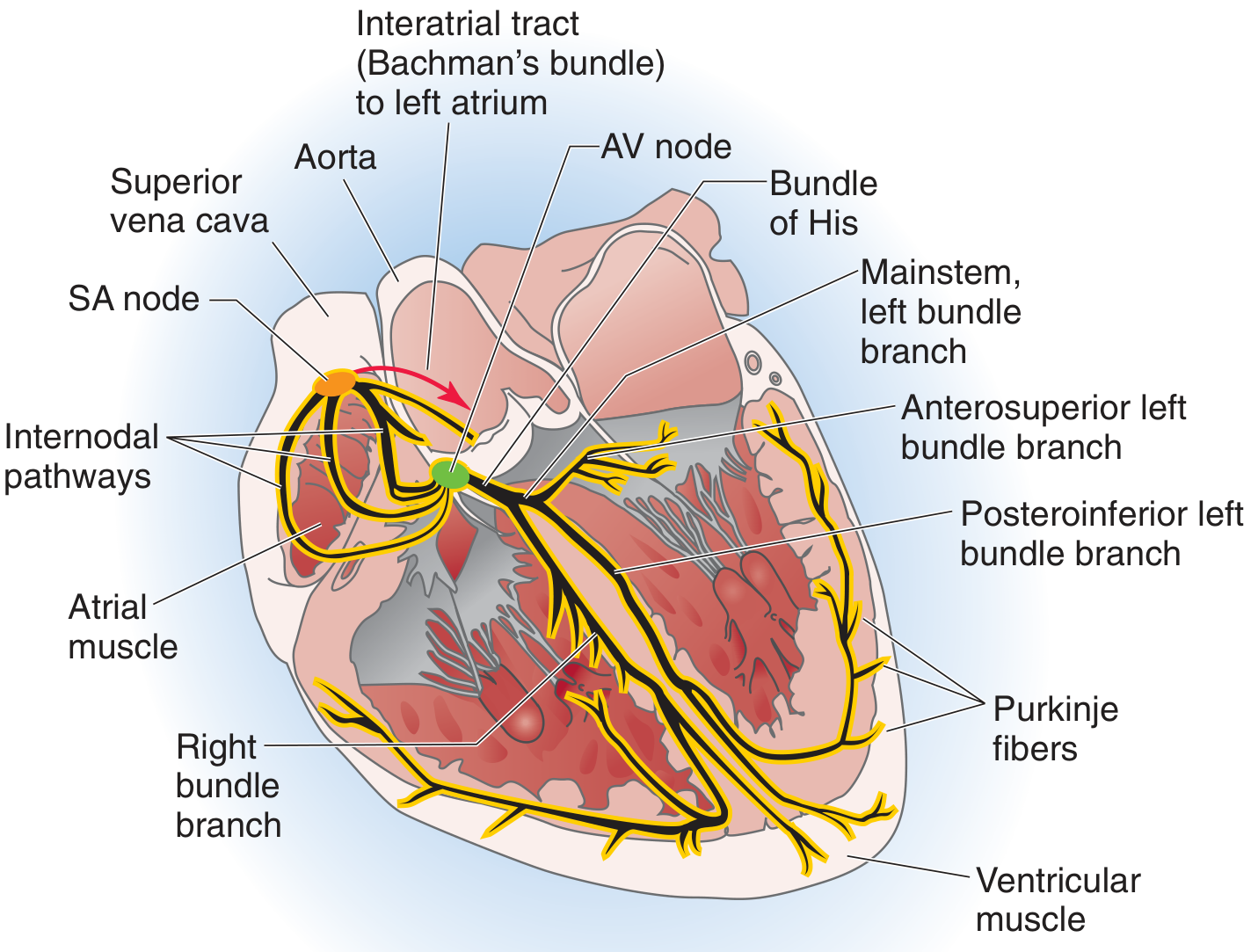
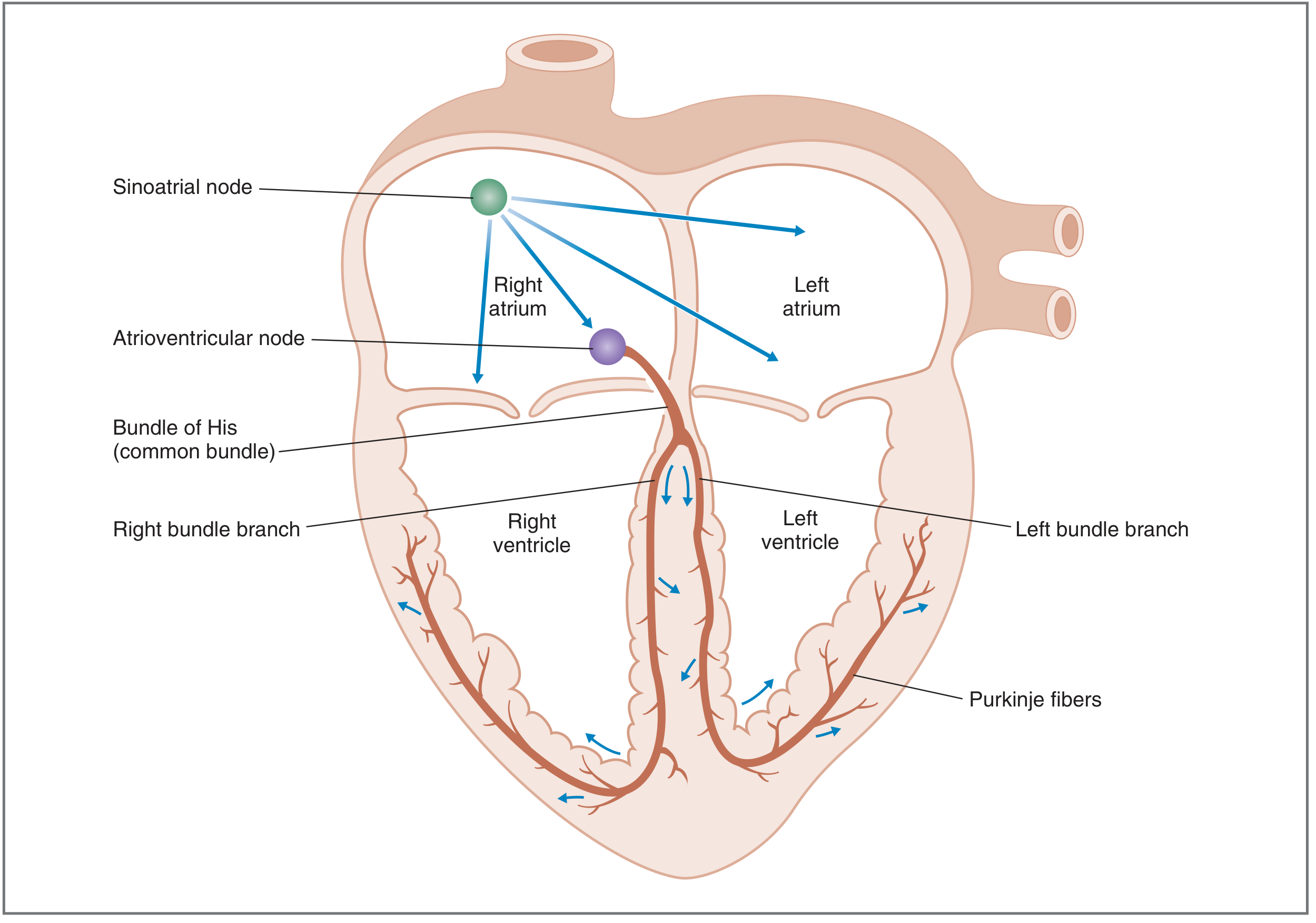
Normal sequence of activation:
- SA node (right atrium) - the primary pacemaker; fires 60-100 impulses/min
- Atrial internodal tracts - spread excitation to both atria and simultaneously to the AV node
- AV node - deliberately slows conduction (ensuring ventricular filling before contraction). This is the only electrical bridge between atria and ventricles (the fibrous AV ring blocks direct spread)
- Bundle of His → left and right bundle branches → Purkinje system - conduction is extremely fast here, distributing activation simultaneously to both ventricles. Rapid conduction apex to base allows efficient ejection.
Normal sinus rhythm requires: (1) origin in SA node, (2) rate 60-100/min, (3) correct sequence and timing of myocardial activation. - Costanzo Physiology, p. 138
Latent pacemakers (cells in AV node, His-Purkinje system) also have automaticity but are suppressed by the SA node's faster rate. Their intrinsic rates are lower (AV node ~40-60/min, ventricles ~20-40/min) and they take over only if the SA node fails.
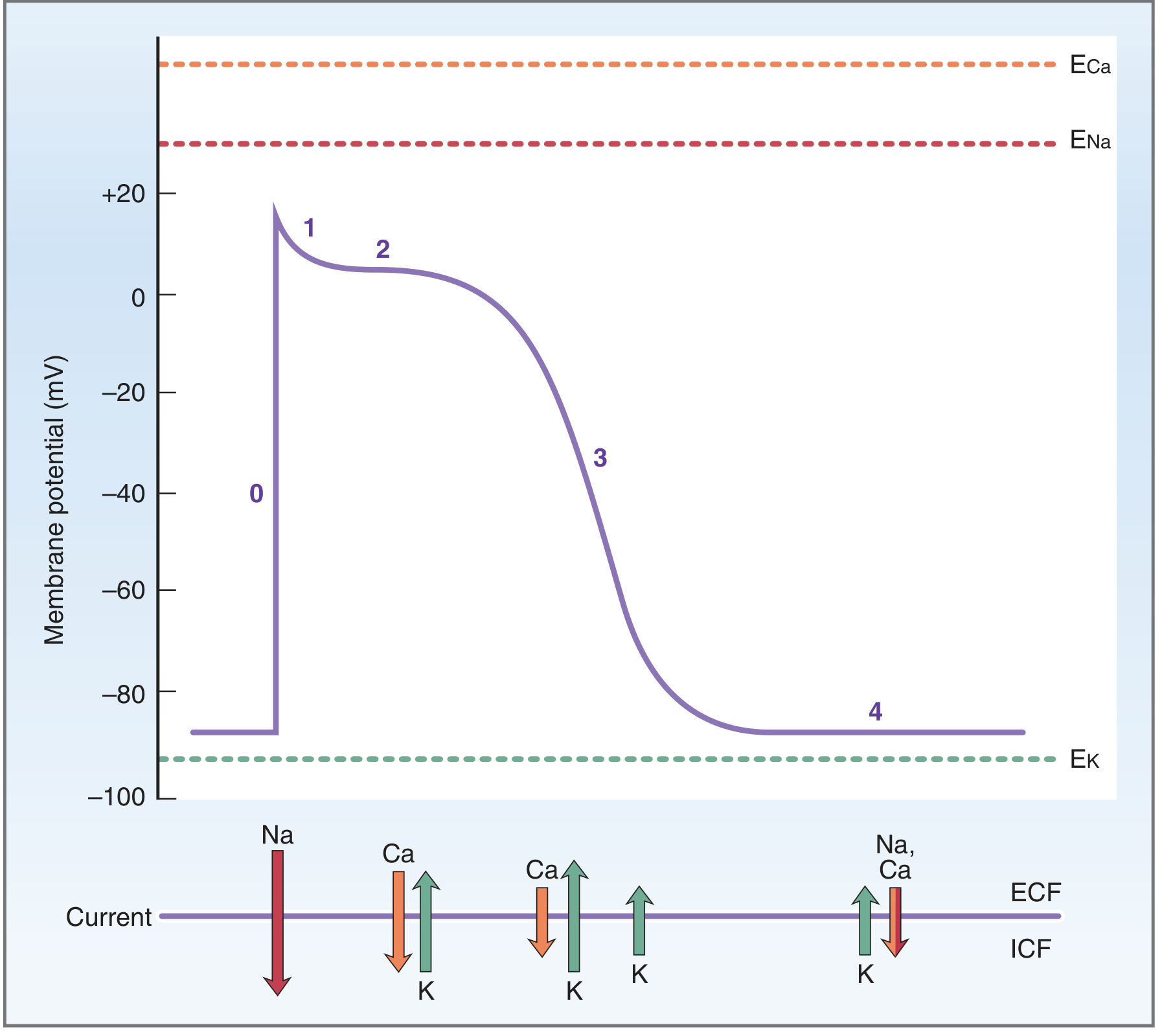
1.3 Cardiac Action Potential - Ventricular Type
The resting membrane potential of ventricular cells is about -85 to -90 mV, maintained primarily by high K+ conductance (membrane potential approaches E_K).
| Phase | Name | Ionic Mechanism |
|---|---|---|
| 0 | Upstroke (rapid depolarization) | Fast Na+ channels open → massive Na+ influx (INa) → membrane reaches ~+20 mV |
| 1 | Initial repolarization | Fast Na+ channels inactivate; transient K+ outward current (Ito) |
| 2 | Plateau | Inward Ca2+ current (ICa via L-type channels) balanced by outward K+ current - the long plateau is UNIQUE to cardiac muscle; triggers Ca2+-induced Ca2+ release (excitation-contraction coupling) |
| 3 | Repolarization | Ca2+ channels inactivate; K+ conductance (IK) increases → outward K+ current restores resting potential |
| 4 | Resting potential | Stable at ~-85 mV; no spontaneous depolarization in contractile cells |
The plateau (Phase 2) is what makes the cardiac action potential so long (~200-300 ms vs. ~1 ms in nerve). This long duration creates a similarly long refractory period, which prevents tetanic (sustained) contraction - critical for a pump that must relax to fill between beats. - Costanzo Physiology, pp. 140-142
1.4 SA Node Action Potential - Pacemaker Type
The SA node differs fundamentally from ventricular cells:
- Resting potential is less negative (~-65 mV maximum diastolic potential)
- Phases 1 and 2 are absent
- Upstroke (Phase 0) is carried by Ca2+ current (L-type and T-type channels), NOT fast Na+ - hence it is slower and less steep
- Phase 3 - repolarization by outward K+ current
- Phase 4 - slow spontaneous depolarization (pacemaker potential): caused by the "funny current" (If), an inward Na+ current activated by hyperpolarization. As If depolarizes the cell toward threshold, T-type Ca2+ channels open, then L-type Ca2+ channels fire the full upstroke
The rate of Phase 4 depolarization determines heart rate:
- Faster Phase 4 slope → threshold reached sooner → higher heart rate (sympathetic stimulation)
- Slower Phase 4 slope → lower heart rate (parasympathetic/vagal stimulation)
1.5 Gap Junctions and Cell-to-Cell Conduction
Cardiac cells are electrically coupled through gap junctions (electrical synapses). Current flows from one cell to the next according to Ohm's law:
I_AB = ΔV_AB / R_AB
When gap junction resistance is low (cells tightly coupled), depolarizing current spreads freely from cell to cell. This allows the action potential to propagate as a wavefront across the myocardium - making the heart function as a functional syncytium. - Medical Physiology, p. 711
PART 2: CARDIAC HEMODYNAMICS
2.1 Cardiac Output
Cardiac output (CO) is the volume of blood ejected by either ventricle per minute:
CO = Heart Rate (HR) × Stroke Volume (SV)
- Normal resting CO: ~5 L/min in a 70-kg adult
- Cardiac index = CO / body surface area; normal ~3.0 L/(min·m²) - normalizes for body size
- Right and left ventricular outputs are equal in steady state (conservation of mass / continuity principle)
The stroke volume is determined by three factors: - Morgan & Mikhail's Clinical Anesthesiology, p. 657
| Determinant | Definition | Clinical Proxy |
|---|---|---|
| Preload | Ventricular end-diastolic volume | CVP, PCWP, LV-EDP |
| Afterload | Resistance the ventricle must overcome to eject | SVR (left), PVR (right) |
| Contractility | Intrinsic myocardial pump ability, independent of preload/afterload | Ejection fraction, dP/dt |
2.2 Preload and the Frank-Starling Mechanism
Preload = ventricular end-diastolic volume (EDV), reflecting the stretch of myocardial fibers before contraction.
The Frank-Starling law of the heart states that cardiac output increases as preload increases (up to a point), because greater stretch increases the sensitivity of myofilaments to Ca2+ and optimizes overlap of actin-myosin crossbridges.
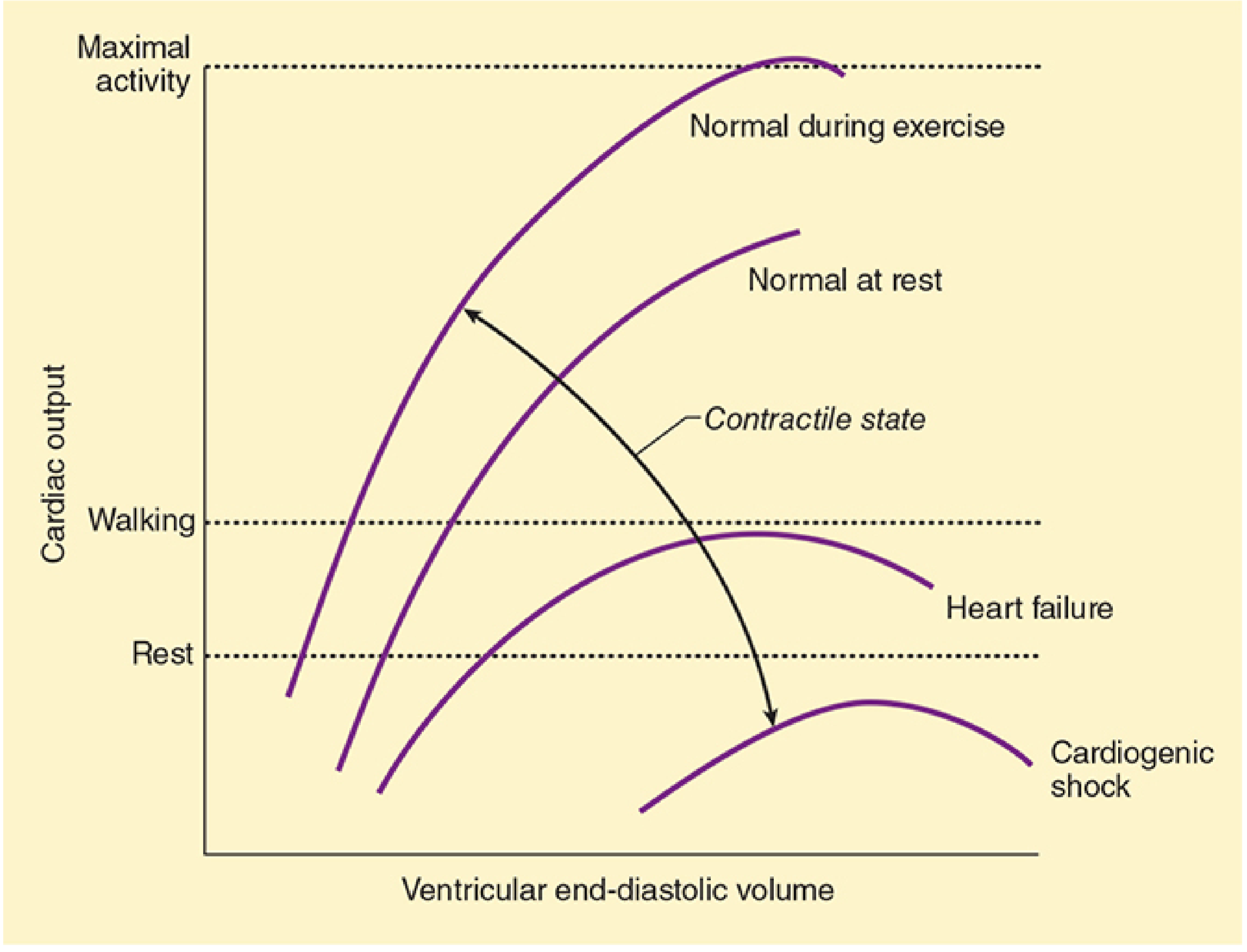
Key points from the Starling curves:
- As EDV increases, CO rises (ascending limb)
- Excessive distension leads to no gain or even a decline in CO (descending limb - seen in heart failure)
- Each contractile state has its own curve; increased inotropy shifts the curve UP and to the LEFT
Factors affecting preload:
- Blood volume, venous tone, body posture, intrathoracic pressure, pericardial pressure, heart rate, atrial contraction (the "atrial kick" contributes ~20-30% of ventricular filling) - Morgan & Mikhail, p. 658
2.3 Afterload
Afterload = the wall tension the ventricle must develop to eject blood. Expressed by the Law of Laplace:
Wall tension = (Pressure × Radius) / (2 × Wall Thickness)
Clinically, left ventricular afterload is approximated by systemic vascular resistance (SVR):
SVR = 80 × (MAP - CVP) / CO [normal: 900-1500 dyn·s·cm⁻⁵]
Right ventricular afterload is approximated by pulmonary vascular resistance (PVR):
PVR = 80 × (PAP - LAP) / CO [normal: 50-150 dyn·s·cm⁻⁵]
Key points:
- CO declines with large increases in afterload
- The RV (thinner-walled) is more sensitive to afterload increases than the LV
- In heart failure or myocardial depression, CO is very sensitive to even small changes in afterload - Morgan & Mikhail, p. 661
2.4 Contractility (Inotropy)
Contractility = the intrinsic ability of the myocardium to generate force, independent of preload and afterload. It is related to the rate of myocardial fiber shortening, which depends on intracellular Ca2+ concentration during systole.
Increases contractility:
- Sympathetic stimulation (norepinephrine, epinephrine via β1-receptors)
- Sympathomimetic drugs (dobutamine, dopamine)
- Cardiac glycosides (digoxin)
- Increased heart rate (Bowditch/treppe effect)
Decreases contractility:
- Hypoxia and acidosis
- Catecholamine depletion
- Loss of functioning myocardium (ischemia, infarction)
- Most anesthetic agents at high doses
- Antiarrhythmic drugs (at large doses) - Morgan & Mikhail, p. 662
2.5 Vascular Resistance and Blood Flow
The relationship between flow, pressure, and resistance in the circulation follows the fluid mechanics equivalent of Ohm's law:
CO = ΔP / R (where ΔP = driving pressure, R = vascular resistance)
Poiseuille's law for flow in a tube:
F = (π r⁴ ΔP) / (8 η L)
Flow is proportional to the fourth power of the radius. This means small changes in arteriolar radius have enormous effects on resistance - arteriolar tone is the dominant regulator of SVR and therefore of afterload. - Medical Physiology, p. 604
Summary Table: Electrophysiology vs. Hemodynamics
| Topic | Electrophysiology | Hemodynamics |
|---|---|---|
| Primary driver | Ionic currents (Na+, Ca2+, K+) | Pressure gradients, vascular resistance |
| SA node role | Primary pacemaker; sets HR | HR directly multiplies stroke volume → CO |
| AV node role | Delay ensures atrial-ventricular coordination | Maintains optimal ventricular filling time |
| Plateau (Phase 2) | Prevents tetany via long refractory period | Enables coordinated contraction for efficient ejection |
| Sympathetic effect | ↑ Phase 4 slope → ↑ HR (chronotropy); ↑ conduction velocity | ↑ Contractility (inotropy), ↑ HR → ↑ CO |
| Parasympathetic effect | ↓ Phase 4 slope → ↓ HR; slows AV node | ↓ HR, mildly ↓ CO |
Sources:
- Costanzo Physiology 7th Ed., pp. 137-142
- Medical Physiology (Boron & Boulpaep), pp. 604, 711
- Morgan & Mikhail's Clinical Anesthesiology 7th Ed., pp. 657-662
This is a shared conversation. Sign in to Orris to start your own chat.