Grattage test
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
grattage test psoriasis dermatology signs steps
Reading File
Reading Web Page
https://ijdvl.com/scaly-signs-in-dermatology
Loading Image
Grattage Test (Psoriasis)
The grattage test (from French gratter = to scratch) is a bedside clinical maneuver used in the diagnosis of psoriasis. It involves gently scraping the surface of a psoriatic plaque with a fingernail, edge of a glass slide, or spatula, in a light tangential manner. It is especially useful when scaling is not clinically obvious.
The Three-Step Sequence
When a psoriatic plaque is scraped progressively, three characteristic findings appear in sequence:
| Step | Finding | Name |
|---|---|---|
| 1 | Scales become whiter and more silvery as air is introduced at the keratin interfaces | Candle-grease sign (signe de la tache de bougie) |
| 2 | Scales are completely removed, exposing a moist, red, smooth, glossy surface (the basement membrane) | Membrane of Bulkeley (also called the terminal lamella) |
| 3 | Further removal tears the thin suprapapillary epidermis, exposing dilated papillary capillaries - producing multiple pinpoint bleeding spots | Auspitz sign |
Details of Each Step
Step 1 - Candle-grease sign:
Gentle scratching produces silvery-white, coherent, dry scales that peel off in layers, resembling shavings from a wax (tallow) candle. This reflects the parakeratotic, loosely adherent scale of psoriasis.
Step 2 - Membrane of Bulkeley:
Continued scraping strips away all scales to reveal a smooth, moist, red, glossy membrane. This is the thinned stratum mucosum (stratum spinosum) over elongated dermal papillae, also called the terminal lamella or Bulkeley membrane.
Step 3 - Auspitz sign:
Further scraping tears the thin suprapapillary epithelium overlying the dilated, tortuous capillaries at the tips of elongated dermal papillae, producing multiple punctate bleeding points. This is the Auspitz sign.
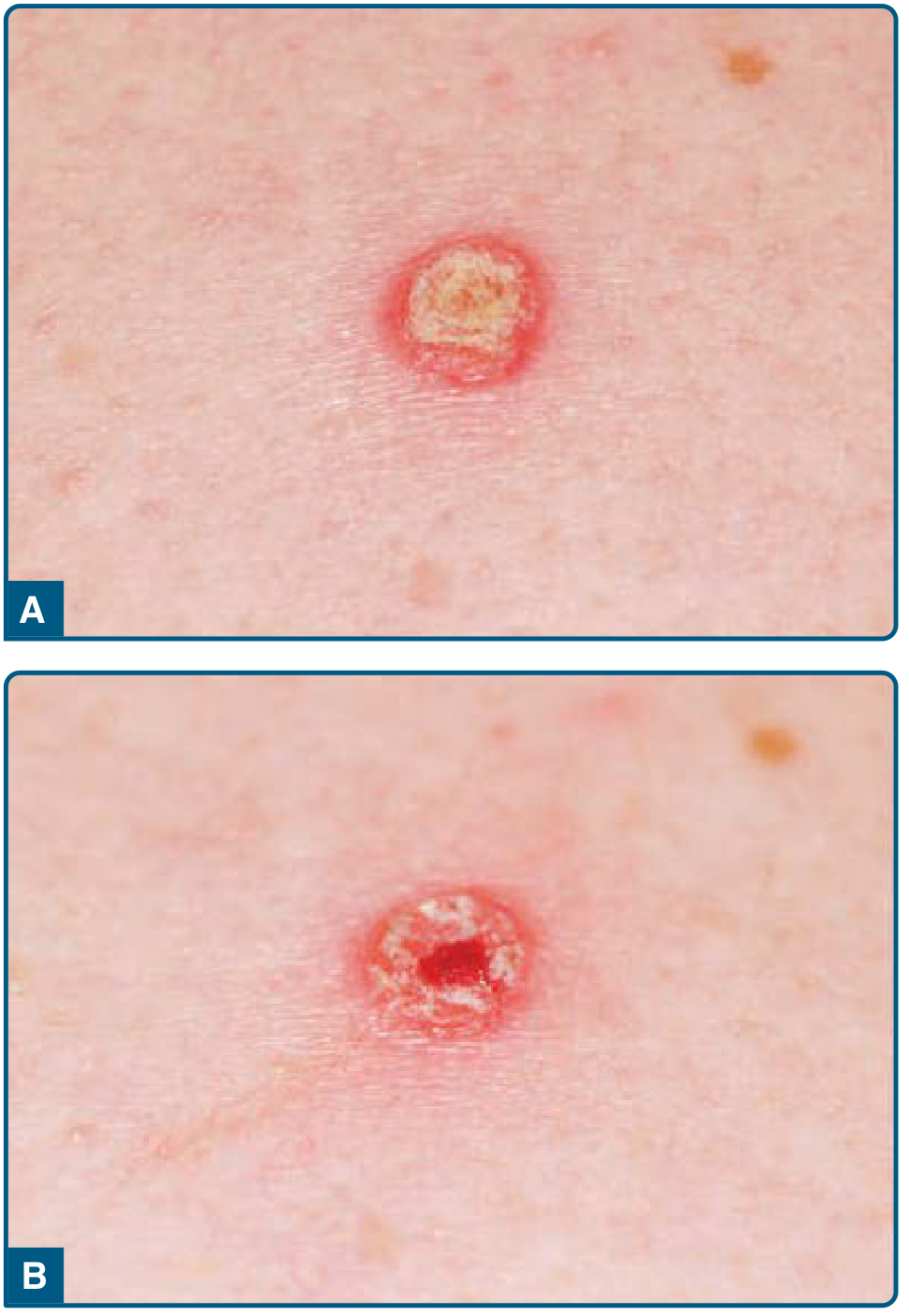
Figure: A - Psoriatic plaque with overlying scale. B - Auspitz sign: pinpoint bleeding after scale removal. (From Fitzpatrick's Dermatology)
Histological Basis
The grattage findings are explained by the characteristic histopathology of psoriasis:
- Parakeratosis - retention of nuclei in the stratum corneum, producing cohesive silvery scale
- Suprapapillary thinning of the stratum malpighii - the epidermis over dermal papillae is only 2-3 cell layers thick
- Elongation of dermal papillae (acanthosis)
- Dilatation and tortuosity of papillary capillaries - these are easily torn by scraping
Clinical Notes
- The grattage test is particularly useful when scaling is not readily apparent clinically; light scratching induces visible scale.
- It is considered pathognomonic of psoriasis by some authors (Hellgren et al.), but both the grattage findings and the Auspitz sign are present only in untreated patients - partial treatment may ablate these signs.
- Auspitz sign is not fully specific: it can also be seen in Darier disease and actinic keratosis. It is also absent in certain psoriasis subtypes (inverse, erythrodermic, pustular, guttate).
- The test is distinct from but closely related to Auspitz sign; grattage is the procedure that elicits both the candle-grease appearance and the Auspitz sign as its end result.
Sources: Fitzpatrick's Dermatology (8e), p.488; Andrews' Diseases of the Skin; Scaly signs in dermatology - IJDVL; Clinicohistopathological correlation in psoriasis - IJDVL
Koebners phenomenon
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Koebner Phenomenon (Isomorphic Response)
Definition: The Koebner phenomenon is the appearance of new skin lesions, identical to the patient's primary dermatosis, at sites of cutaneous trauma in previously uninvolved skin. It was first described by Heinrich Koebner in 1877 in patients with psoriasis.
It is also called the isomorphic response - "iso" (same) + "morphic" (shape) - because the induced lesions take the same morphology as the original disease.
Diseases That Classically Show the Koebner Phenomenon
| Disease | Notes |
|---|---|
| Psoriasis | Most classic example; ~25% of patients; all-or-none phenomenon |
| Lichen planus | Linear arrays of violaceous papules at trauma sites |
| Vitiligo | Linear depigmentation at sites of skin injury; more common in active/progressive disease |
| Lichen nitidus | Tiny flesh-colored papules induced at trauma sites |
| Cutaneous small vessel vasculitis | Trauma can precipitate lesions |
| Still disease | Salmon-colored evanescent plaques at pressure sites |

Figure: Koebner phenomenon in psoriasis. A - Psoriatic plaques appearing in keratome biopsy sites 4 weeks after biopsy. B - Flare of psoriasis after sunburn, with sparing of the sun-protected area under a bandage. (From Fitzpatrick's Dermatology)
Key Features
Types of trauma that can trigger it:
- Scratches, cuts, abrasions
- Surgical incisions, biopsies
- Burns (including sunburn)
- Tattoos and needle pricks
- Pressure and friction
- Viral exanthems (e.g. pityriasis rosea can act as a trigger for psoriasis)
- Phototherapy burns (over-dosing UV)
Timing: The lag time between trauma and lesion appearance is typically 2-6 weeks (Dermatology 2-Volume Set 5e); Fitzpatrick's quotes 7-14 days for psoriasis specifically.
All-or-none rule (psoriasis): If psoriasis occurs at one site of injury, it will occur at all sites of comparable injury. A patient may be "Koebner-negative" at one time and "Koebner-positive" at another - positivity often correlates with active, flaring disease.
Frequency in psoriasis: 25-75% of patients experience Koebner phenomenon at some point during their disease.
Lichen Planus - Mechanism
In lichen planus, the Koebner reaction is now explained by trauma-induced exposure of plasmacytoid dendritic cells to endogenous peptides (such as cathelicidin LL-37), triggering the cytotoxic T-cell response that underlies LP.
Related but Distinct Phenomena
| Phenomenon | Description |
|---|---|
| Pseudo-Koebner phenomenon | Autoinoculation of infective lesions at trauma sites - seen with verrucae (warts) and molluscum contagiosum |
| Wolf isotopic response | A second, unrelated skin disease appears at the site of a previously healed skin disease (e.g. granuloma annulare developing at a healed herpes zoster scar) |
| Pathergy | Exaggerated skin response to minor trauma (e.g. needle prick causing a pustule) - classic in Behcet disease |
| Reverse Koebner | Spontaneous clearance of skin lesions at a trauma site (reported in psoriasis) |
Clinical Significance
- Explains the distribution of psoriasis on elbows, knees, and scalp - areas of repeated mechanical trauma
- Relevant to surgical planning - incisions/biopsies in psoriatic/vitiligo patients can worsen disease
- Suggests psoriasis behaves as a generalized skin disease that can be triggered locally at any site
- Presence of Koebner phenomenon implies active disease and may indicate poor prognosis
Sources: Fitzpatrick's Dermatology (8e), p.488; Dermatology 2-Volume Set 5e (Bolognia), p.11
This is a shared conversation. Sign in to Orris to start your own chat.