Mammogram
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Searching PubMed
"mammography" AND "breast cancer" AND "diagnosis"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
I now have rich content from multiple authoritative sources. Let me compile the comprehensive answer.
Mammography in Breast Cancer Diagnosis
What Is Mammography?
Mammography is a low-dose X-ray technique specifically designed for imaging the breast. The breast is compressed between two plates to reduce tissue thickness, separate adjacent structures, and improve spatial resolution. Two standard views are taken of each breast: the mediolateral oblique (MLO) and the craniocaudal (CC) views. Radiation dose is approximately 1 mGy per film - Grainger & Allison's Diagnostic Radiology, p. 1648.
Special X-ray tubes with a molybdenum target produce low-energy radiation (peaks at 17.5 and 19.6 keV), providing high tissue contrast. This is necessary to detect subtle density differences, including microcalcifications as small as 100 µm.
Indications
- Women >40 years presenting with breast symptoms (mass, skin thickening, nipple retraction, discharge, nipple eczema)
- Screening of asymptomatic women (primary screening tool)
- Follow-up after previously treated breast cancer
- Guidance for biopsy and preoperative localization
- Sabiston Textbook of Surgery, p. 1375
Types of Mammography
| Type | Description |
|---|---|
| 2D Digital Mammography | Standard; digital images stored and manipulated electronically; superior to film-screen mammography for dense breasts |
| Digital Breast Tomosynthesis (DBT / 3D Mammography) | Multiple sectional images from different angles reconstructed into 3D; better separates overlapping tissue; detects more cancers than 2D alone (STORM-2 trial) |
| Contrast-Enhanced Spectral Mammography (CESM) | IV iodine contrast given before mammography; exploits tumor neoangiogenesis; approaches accuracy of MRI |
| Computer-Assisted Diagnosis (CAD) | AI/machine learning software that flags abnormalities; enhances sensitivity alongside radiologist review |
- Sabiston Textbook of Surgery, p. 1375; Grainger & Allison's Diagnostic Radiology, p. 1648
Breast Density and BI-RADS Classification
The mammographic report begins with a density assessment using the ACR BI-RADS lexicon:
| BI-RADS Density | Description | Notes |
|---|---|---|
| A (1) | Almost entirely fatty | Lowest cancer-masking risk |
| B (2) | Scattered fibroglandular density | |
| C (3) | Heterogeneously dense | Supplemental imaging considered |
| D (4) | Extremely dense | 4-6x increased cancer risk; mammography sensitivity reduced |
Dense breasts (C/D) are both a risk factor for breast cancer AND reduce mammographic accuracy. About 10-15% of clinically evident cancers have no mammographic abnormality at all - Grainger & Allison's Diagnostic Radiology, p. 1648.
Mammographic Features of Breast Cancer
The two main categories of abnormality are:
1. Masses / Densities
- Malignant features: irregular shape, spiculated margins, architectural distortion, asymmetric density
- Benign features: well-defined, round/oval shape, lucent halo (e.g., cyst - Fig. 63.9 in Grainger)
2. Microcalcifications
- Clustered microcalcifications are a hallmark finding for in-situ and invasive cancer
- High-grade tumors (especially DCIS) frequently show calcifications
- On biopsy, microcalcifications in at least 3 separate cores are needed to confirm representative sampling
Ancillary signs of advanced malignancy include: lymphadenopathy, breast edema, skin thickening/retraction, areolar changes - Bailey & Love's Surgery, p. 9999.
BI-RADS Reporting Categories (Assessment)
| Category | Assessment | Management |
|---|---|---|
| 0 | Incomplete | Additional imaging needed |
| 1 | Negative | Routine screening |
| 2 | Benign | Routine screening |
| 3 | Probably benign | Short-interval follow-up (6 months) |
| 4 | Suspicious | Tissue biopsy recommended |
| 5 | Highly suggestive of malignancy | Biopsy - treat as malignant |
| 6 | Known biopsy-proven malignancy | Surgical planning |
Biopsy is required for definitive diagnosis in BI-RADS 4 and 5 lesions - Bailey & Love's Surgery.
Triple Assessment - The Gold Standard
Mammography alone is not diagnostic. The expected standard for breast diagnosis is the triple assessment:
- Clinical examination
- Imaging (mammography ± ultrasound ± MRI)
- Needle biopsy (core biopsy or fine-needle aspiration)
All three components must be concordant. A benign imaging finding does not exclude cancer if clinical examination is suspicious - Grainger & Allison's Diagnostic Radiology, p. 1648.
Adjunct Modalities
Ultrasound (US)
- Distinguishes solid from cystic lesions
- Malignant features on US: irregular, spiculated, hypoechoic, taller-than-wide, acoustic shadowing, central penetrating vessels on Doppler
- Best for axillary staging (lymph node biopsy guidance) and image-guided biopsies
- Not recommended as a standalone screening tool (operator-dependent)
MRI
- Highest sensitivity for invasive breast cancer
- Recommended annually for high-risk patients (BRCA mutation carriers, significant family history, >20% lifetime risk, previous breast cancer, dense breasts)
- Used when 2D mammography and US are discordant, or for extent-of-disease staging before surgery
Imaging Findings (Multi-Modality)
The image below shows mammography, ultrasound, and MRI findings in breast disease:
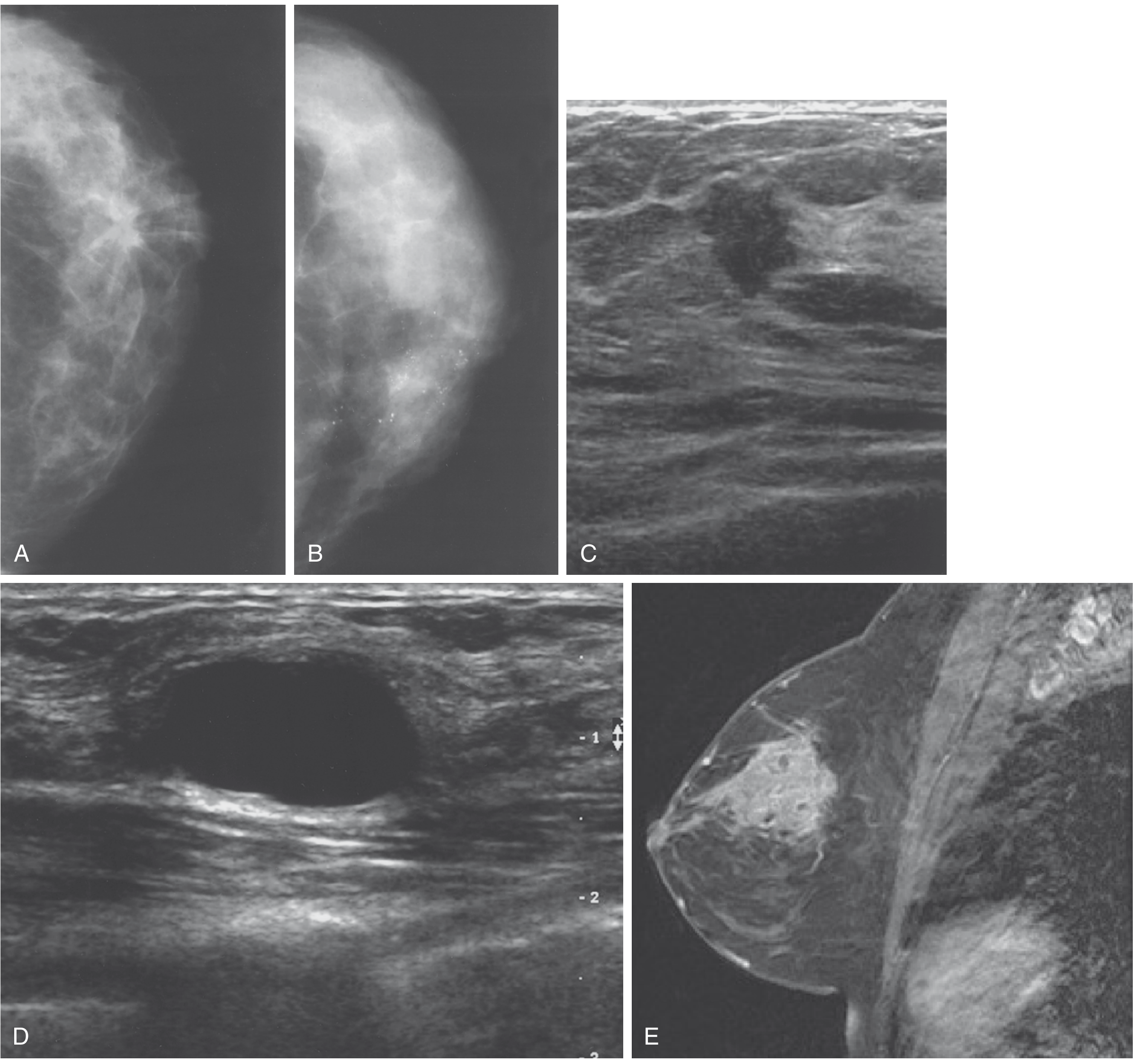
Panels A-B: Mammographic views; C: Ultrasound showing irregular hypoechoic malignant mass; D: Cyst on ultrasound; E: MRI of breast lesion - Sabiston Textbook of Surgery, Fig. 68.7
Screening Guidelines Summary
Per Sabiston Textbook of Surgery (p. 1375):
- Discuss breast cancer risk with all women in their 20s
- Average-risk women: Annual mammography starting at age 40, continued as long as the patient is a surgical candidate
- High-risk women (BRCA+, strong family history, dense breasts, >20% lifetime risk): Annual MRI in addition to mammography
- Supplemental US or MRI adds ~5 extra cancers detected per 1,000 exams, but increases recall rate >10% and biopsy rate
Recent Evidence
A 2025 systematic review (PMID 40047905) covering 28 systematic reviews confirmed that mammography screening significantly reduces breast cancer mortality, though questions remain about over-diagnosis. The evidence base supports annual screening from age 40 in average-risk women.
Key takeaway: Mammography remains the primary tool for breast cancer screening and initial diagnosis. Findings are classified using BI-RADS, and all suspicious findings (BI-RADS 4-5) require histological confirmation via biopsy. No imaging modality alone is sufficient - triple assessment (clinical + imaging + biopsy) is the diagnostic standard.
This is a shared conversation. Sign in to Orris to start your own chat.