Make a note about Acute cholecystitis
Reading File
Finding Sources
Searching PubMed
"acute cholecystitis"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, well-structured note. Here it is:
Acute Cholecystitis
Definition & Epidemiology
Acute cholecystitis is inflammation of the gallbladder caused by obstruction of the cystic duct followed by bacterial invasion and overgrowth. It is the primary complication of gallstones and the most common reason for emergency cholecystectomy.
- Calculous (90%): obstruction by gallstone at the neck or cystic duct
- Acalculous (10%): occurs in critically ill patients; pathophysiology is transmural ischemia
Pathophysiology
Calculous
Obstruction of the cystic duct by a stone triggers chemical irritation. Mucosal phospholipases hydrolyze lecithins to toxic lysolecithins, the protective mucus layer is disrupted, and bile salts exert a direct detergent effect on the epithelium. Prostaglandins released within the distended gallbladder wall worsen inflammation, and elevated intraluminal pressure compromises mucosal blood flow. Bacterial superinfection follows later in the course and amplifies inflammation. Particularly common in diabetic patients with symptomatic gallstones.
Acalculous
The cystic artery is an end-artery with no collateral circulation. Ischemia, gallbladder stasis (biliary sludge, viscous bile, mucus), and wall edema combine to obstruct outflow without stones. It occurs in hospitalized patients with:
- Sepsis with hypotension / multi-organ failure
- Major trauma and burns
- Immunosuppression
- Diabetes mellitus
- Systemic infections
Morphology (Pathology)
| Severity | Gross Findings |
|---|---|
| Mild | Wall thickening, edema, hyperemia; lumen with turbid bile |
| Moderate | Fibrinous/fibrinopurulent serosal exudate |
| Empyema | Lumen filled with virtually pure pus |
| Gangrenous | Green-black necrotic wall with perforations; blotchy violaceous to green-black discoloration |
| Emphysematous | Gas-forming organisms (clostridia, coliforms) invade the wall; gas visible on imaging |
Histologically: early changes include edema, congestion, and mucosal erosion; neutrophils are sparse unless superinfection occurs.
Clinical Features
Symptoms:
- Progressive RUQ or epigastric pain lasting >6 hours (key differentiator from biliary colic)
- Nausea, vomiting, anorexia
- Mild fever, tachycardia, diaphoresis
Signs:
- RUQ tenderness; Murphy's sign (inspiratory arrest on palpation of the RUQ)
- Most patients are not jaundiced - hyperbilirubinemia suggests CBD obstruction
Labs:
- Leukocytosis (mild to moderate)
- Mildly elevated ALP
- May have elevated bilirubin if Mirizzi syndrome or choledocholithiasis
Natural history: Without intervention, 75% of attacks subside within 7-10 days. However, up to 25% of patients develop progressively severe symptoms requiring urgent surgery. Recurrence is common without definitive treatment.
Acalculous presents more insidiously (symptoms masked by underlying illness); higher rates of gangrene and perforation; requires a high index of suspicion.
Diagnosis
1st line - RUQ Ultrasound:
- Sensitivity 88-94%, specificity 78-80%
- Findings: gallstones, gallbladder wall thickening (>4mm), pericholecystic fluid, sonographic Murphy's sign
2nd line - HIDA Scan (cholescintigraphy):
- Indicated when US is inconclusive or discordant with clinical picture
- Non-visualization of the gallbladder = acute cholecystitis
- Sensitivity 96%, specificity 90%
CT Scan:
- Indicated for suspected complications: emphysematous cholecystitis, pericholecystic abscess, perforation, peritonitis
Severity Grading (Tokyo Guidelines)
| Grade | Definition |
|---|---|
| Grade I (Mild) | Mild inflammation; no organ dysfunction; fit patient |
| Grade II (Moderate) | WBC >18,000/mm³, palpable RUQ mass, duration >72h, marked local inflammation (gangrenous, emphysematous, pericholecystic abscess) |
| Grade III (Severe) | Organ dysfunction (cardiovascular, neurological, respiratory, renal, hepatic, hematologic) |
Higher grades are associated with worse outcomes, longer stays, and higher conversion to open surgery.
Management
Initial (All Patients)
- IV hydration and electrolyte correction
- NPO
- Analgesia
- IV antibiotics:
- Mild-moderate: Cefoxitin (cephalosporin) or similar
- Severe: Piperacillin-tazobactam or 3rd-generation cephalosporin + metronidazole
- Gangrenous/emphysematous: Add anaerobic coverage (e.g., metronidazole)
Common pathogens: aerobic gram-negative bacilli (E. coli, Klebsiella, Enterobacter, Proteus) and gram-positive organisms (Enterococcus, Streptococcus). Anaerobes in ~15% of isolates.
Definitive - Surgery
Early laparoscopic cholecystectomy (within 24-72 hours of admission) is the standard of care for most patients. Evidence from 7 randomized trials:
| Timing | Mortality | Total Hospital Stay | Treatment Failure |
|---|---|---|---|
| Early surgery | 0% | 9.6 days | N/A |
| Delayed (6-8 wks) | 2.0% | 17.8 days | 26% |
- Early cholecystectomy is significantly superior - shorter total stay, lower mortality, eliminates the risk of interval complications.
- Laparoscopic approach is feasible in most cases. Intraoperative cholangiography is especially valuable to confirm ductal anatomy.
- If severe pericholecystic inflammation obscures the hepatocystic triangle, subtotal fenestrating cholecystectomy or conversion to open may be necessary.
High-Risk / Poor Surgical Candidates
- Percutaneous cholecystostomy (gallbladder drainage) is the preferred bridge; decompresses the gallbladder until elective cholecystectomy can be done
- Endoscopic transmural gallbladder drainage (EUS-guided) is as effective as percutaneous drainage in patients unfit for surgery; note: contraindicated if future surgery remains a possibility
Special Populations
- Diabetics: Higher infectious complications (sepsis, empyema, gangrene); perform cholecystectomy expeditiously
- Elderly: Deceptively benign presentation but high rates of occult severe disease; early cholecystectomy warranted
- Gangrenous/emphysematous risk factors: Male sex, diabetes mellitus, cardiovascular disease, WBC >15,000/mm³
Postoperative Antibiotics
- Not indicated after source control in mild-moderate cholecystitis
- Continue postoperatively in: severe infection, intraoperative gallbladder perforation, or gangrenous cholecystitis
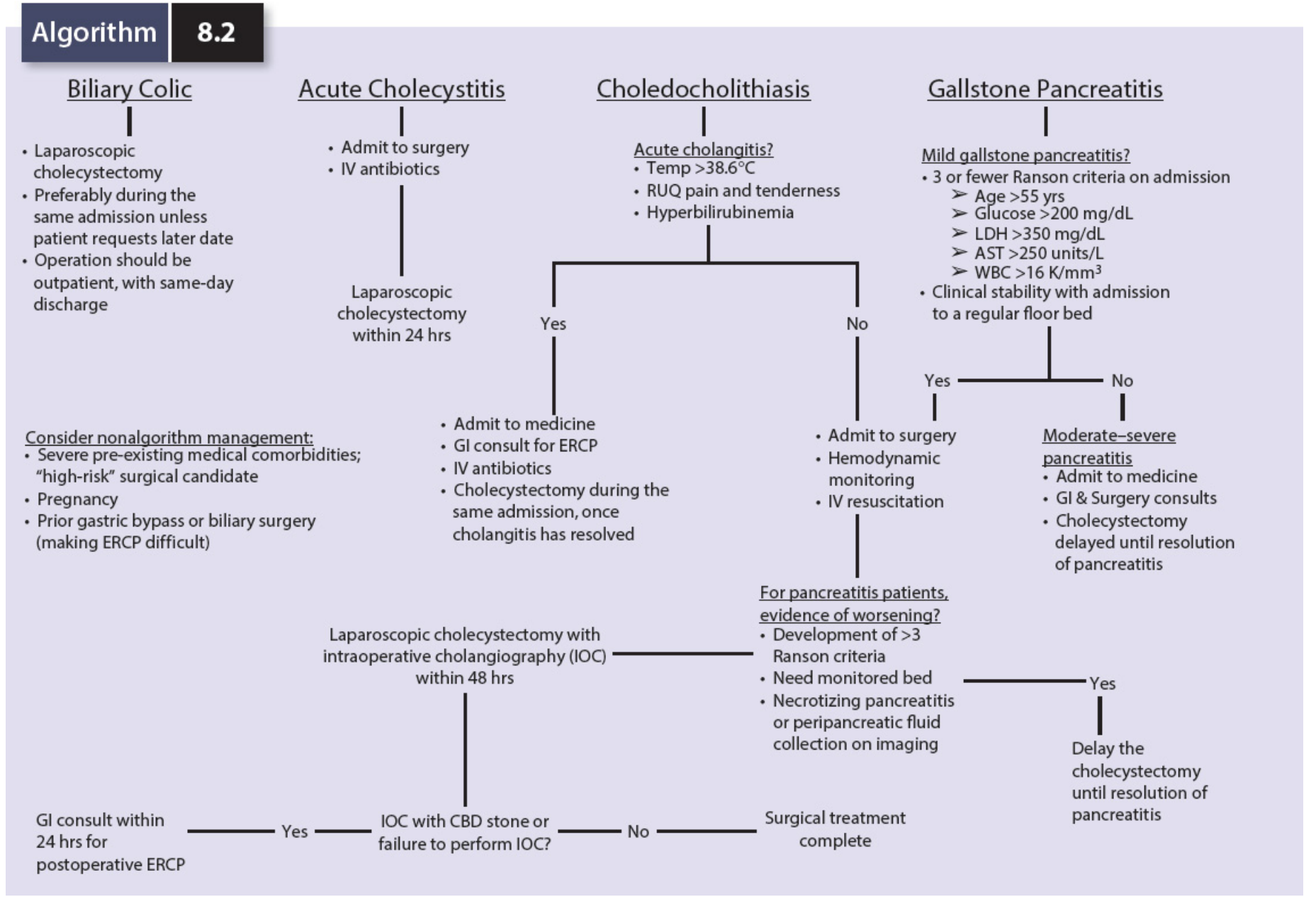
Diagnostic & Treatment Algorithm
Complications
| Complication | Notes |
|---|---|
| Empyema | Gallbladder filled with pus; requires urgent drainage |
| Gangrenous cholecystitis | Necrotic wall; high perforation risk; male, diabetic, cardiovascular disease, WBC >15k |
| Emphysematous cholecystitis | Gas in gallbladder wall by CT/X-ray; clostridial or coliform infection |
| Perforation | Localized (pericholecystic abscess) or free perforation with peritonitis |
| Mirizzi syndrome | Stone in cystic duct compresses CBD causing obstructive jaundice |
| Cholecystoenteric fistula | Stone erodes into bowel; can cause gallstone ileus |
Key Differentials
- Biliary colic (no fever/leukocytosis, pain <6 hours)
- Cholangitis (Charcot's triad: fever + jaundice + RUQ pain)
- Peptic ulcer disease / perforated ulcer
- Acute pancreatitis
- Hepatitis
- Right lower lobe pneumonia (referred pain)
- Appendicitis (if high-lying appendix)
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease, 10e; Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Mulholland and Greenfield's Surgery, 7e
Make a note on normal labour in obstretiic
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive material from multiple authoritative sources. Let me compile the complete note:
Normal Labour (Obstetrics)
Definition
Labour is defined as the presence of sufficient uterine contractions in frequency, intensity, and duration to bring about effacement and dilation of the cervix, ultimately expelling the fetus and placenta. True labour at term commences at 40 ± 2 weeks following the last menstrual period.
Initiation of Labour
The exact mechanism is multifactorial and not fully understood. Key factors include:
- Uterine distension with advancing gestation
- Increased myometrial oxytocin sensitivity - the number of oxytocin receptors rises sharply (circulating oxytocin levels may not increase at onset)
- Prostaglandin synthesis - PGE₂ and PGF₂α play key roles; produced by fetal membranes and decidual tissues
- Fetal cortisol (via HPA axis maturation) signals readiness for delivery
Prodromal Events (2-4 Weeks Before Labour)
| Event | Description |
|---|---|
| Lightening | Fetal presenting part settles into the pelvis; fundal height drops; pelvic pressure increases; may be sudden or gradual over weeks |
| Braxton Hicks contractions | Irregular, painless uterine tightenings; increase in frequency and intensity as term approaches; help with cervical preparation |
| Cervical ripening | Softening, effacement, and anterior positioning of cervix; driven by collagen remodeling and prostaglandins |
| Bloody show | Passage of blood-tinged mucus plug; occurs ~1 week to 1 hour before true labour; most women enter labour within 3 days |
Heavy bleeding (like a menstrual period) is NOT normal - must evaluate for placenta praevia, abruption, etc.
True vs False Labour
| Feature | True Labour | False Labour (Braxton Hicks) |
|---|---|---|
| Contractions | Regular, progressive | Irregular, inconsistent |
| Intensity | Builds progressively | Does not increase |
| Cervical change | Present (effacement + dilation) | None |
| Effect of sedation | No effect on active phase | May abolish contractions |
| Location of pain | Back radiating to front | Usually anterior only |
Active labour contractions: every 2-3 minutes, last ~1 minute, intensity ~40 mmHg. Adequate relaxation between contractions is essential for fetal oxygenation via intervillous blood flow.
Stages of Labour
By convention, labour is divided into four stages:
| Stage | Start | End |
|---|---|---|
| First (Latent + Active) | Onset of true labour | Complete cervical dilation (10 cm) |
| Second | Full dilation | Delivery of the baby |
| Third | Delivery of baby | Delivery of placenta |
| Fourth | Delivery of placenta | 1 hour postpartum (contracted uterus) |
First Stage of Labour
The Friedman Curve (Sigmoid curve of labour)
Labour progression plotted as cervical dilation vs. time follows a sigmoid (S-shaped) curve, with:
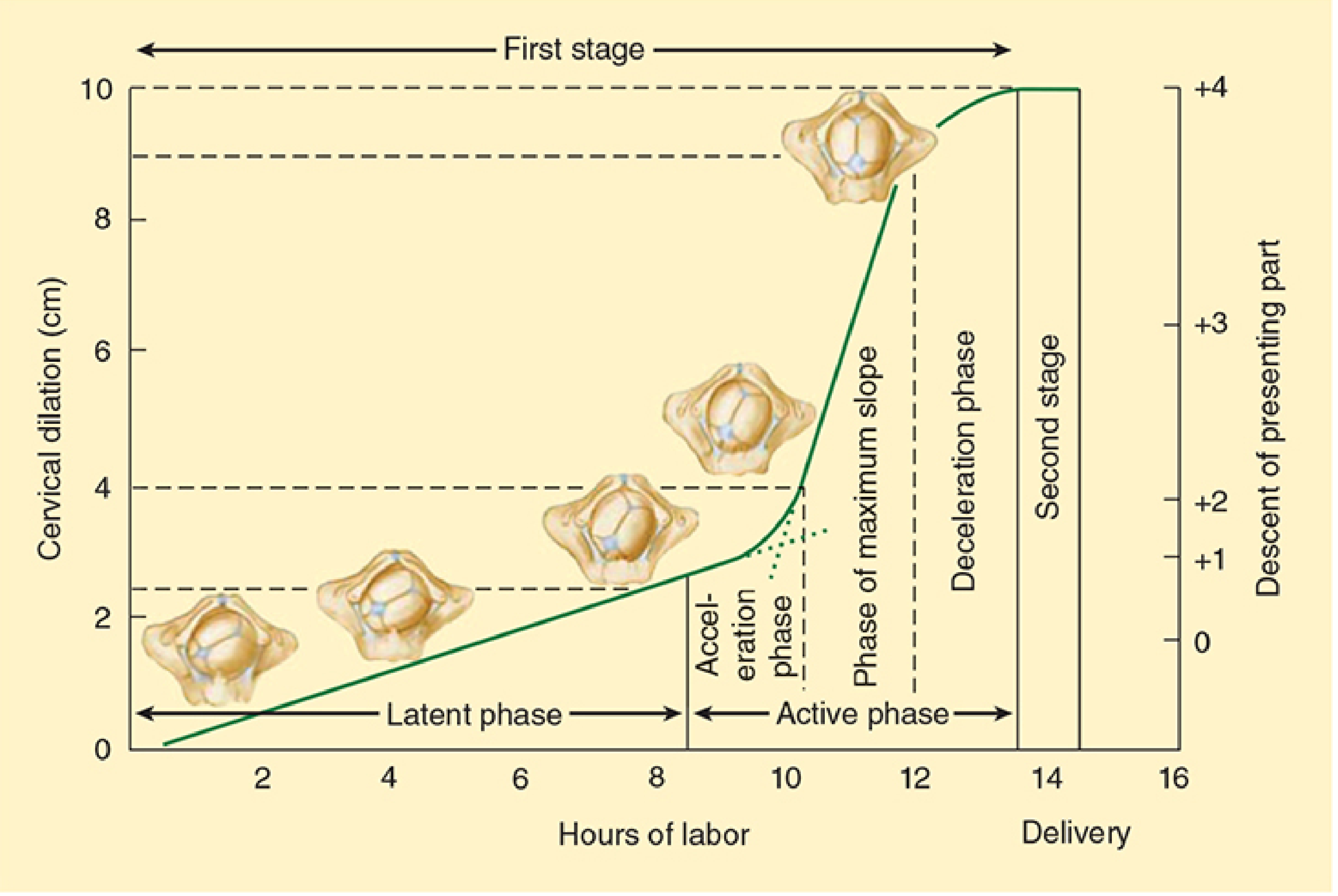
Latent Phase
- Start: Onset of regular contractions
- End: Beginning of rapid dilation (~3-4 cm)
- Cervical change: Effacement, softening, anterior positioning; minimal dilation
- Duration: Up to 20 hours (nullipara) / up to 14 hours (multipara)
- Little effect of analgesia on this phase progression
- Best managed at home with clear liquids
- Prolonged latent phase can be treated with morphine in hospital - often accelerates transition to active phase
Active Phase
The active phase is subdivided into 3 sub-phases (Friedman):
- Acceleration phase - gradual pick-up in dilation rate
- Phase of maximum slope - most rapid dilation
- Deceleration phase - slowing just before full dilation
Rate of dilation:
- Nullipara: ≥ 1.2 cm/hr (Friedman) - more recent data (Zhang 2002) shows slower contemporary rates are normal
- Multipara: ≥ 1.5 cm/hr
Note: Contemporary research (Zhang et al., 2002) has challenged Friedman's curves: modern active labour averages 5.5 hours rather than 2.5 hours; there is a gradual (not abrupt) transition from latent to active phase; no deceleration phase is consistently seen; and ≥2 hours without dilation may occur normally in active phase.
Expected cervical dilation rates in nulliparas (Zhang, 2002):
| Dilation | Median Time | 95th Percentile |
|---|---|---|
| 2→3 cm | 3.2 hr | 15.0 hr |
| 3→4 cm | 2.7 hr | 10.1 hr |
| 4→5 cm | 1.7 hr | 6.6 hr |
| 5→6 cm | 0.8 hr | 3.1 hr |
| 6→7 cm | 0.6 hr | 2.2 hr |
| 7→10 cm | ~0.4-0.5 hr/cm | - |
Progress depends on:
- Strength and frequency of uterine contractions
- Size, position, and attitude of the fetal head
- Size and shape of the bony pelvis
Total First Stage Duration:
- Nullipara: ~8-12 hours (mean 11 hours)
- Multipara: ~5-8 hours (mean 7 hours)
Cardinal Movements of Labour (Second Stage)
The fetal head must negotiate the different diameters of the pelvic inlet, midplane, and outlet. The 7 cardinal movements are:
| # | Movement | Description |
|---|---|---|
| 1 | Engagement | Widest diameter of presenting part passes below the pelvic inlet; station 0 |
| 2 | Descent | Progressive downward movement; begins before 2nd stage, maximal during 2nd stage |
| 3 | Flexion | Head flexes, chin to chest; presents smallest AP diameter (suboccipitobregmatic ~9.5 cm instead of occipitofrontal ~11 cm) |
| 4 | Internal Rotation | Occiput rotates anteriorly from transverse/posterior to OA position to align with AP diameter of outlet |
| 5 | Extension | Head extends under the pubic symphysis; delivers face, nose, mouth, chin in sequence |
| 6 | External Rotation (Restitution) | Head returns to alignment with fetal shoulders |
| 7 | Expulsion | Anterior shoulder delivered first (with gentle downward traction), then posterior shoulder (gentle upward traction), then trunk |
Second Stage of Labour
- Start: Full cervical dilation (10 cm)
- End: Complete delivery of fetus
- Contractions: every 1.5-2 minutes, lasting 1-1.5 minutes
- Maternal bearing-down augments intrauterine pressure and aids expulsion
- Duration:
- Nullipara: average 50 min (up to 2 hrs without epidural / 3 hrs with epidural)
- Multipara: average 20 min
- FHR monitored every 15 min (low-risk) or every 10 min (high-risk)
Delivery sequence:
- Head delivers by extension - suction mouth, pharynx, nose
- Check for nuchal cord; reduce if possible; clamp and cut if too tight
- Anterior shoulder: gentle downward traction + maternal pushing
- Posterior shoulder: gentle upward traction (mother pushes gently)
- Body follows; baby placed on maternal abdomen
- Cord clamped (timing is debated; delayed clamping now preferred)
Third Stage of Labour
- Start: Delivery of baby
- End: Delivery of placenta
- Duration: Typically 15-30 minutes
Signs of placental separation:
- Lengthening of the umbilical cord
- Gush of blood
- Change in contour of the uterine fundus (becomes globular and rises)
- Uterus becomes firm
Mechanism: As the post-delivery uterus contracts, shearing forces separate the placenta from the decidua; the implantation site contracts to arrest bleeding.
Active management of third stage (preferred over expectant management):
- Oxytocin 10 IU IM after delivery of the anterior shoulder or within 1 minute of birth
- Controlled cord traction (Brandt-Andrews manoeuvre)
- Uterine massage after placental delivery
Fourth Stage of Labour
- First hour after placental delivery
- Vigilant monitoring for:
- Excessive vaginal bleeding / postpartum haemorrhage
- Boggy uterus (uterine atony)
- Haemodynamic instability
Management of atony:
- Uterine fundal massage
- Oxytocin 20-40 units in IV fluid or 20 IU IM
- Methylergonovine 0.2 mg IM (contraindicated in hypertension)
- PGF₂α (Carboprost/Hemabate) 250 mcg IM every 15-20 min up to 3 doses
- Misoprostol 200-1000 mcg (oral/sublingual/vaginal/rectal)
Monitoring During Labour
| Parameter | Method | Frequency |
|---|---|---|
| Fetal heart rate | Intermittent auscultation or continuous EFM | Every 30 min (active phase, low risk); every 15 min (higher risk) |
| Cervical dilation & fetal station | Vaginal examination | Every 2-4 hours (or as clinically indicated) |
| Uterine activity | Tocodynamometer (external) or intrauterine pressure catheter (IUPC) | Continuous or periodic |
| Maternal vitals | BP, pulse, temperature | Hourly or more frequently |
Fetal station: Level of presenting part relative to ischial spines in centimetres (negative = above spines; 0 = at spines; positive = below spines). Descent begins well before the second stage.
Maternal Physiological Changes During Labour
- Minute ventilation increases up to 300% during intense contractions
- Oxygen consumption increases ~60% above third-trimester values
- PaCO₂ may fall below 20 mmHg with excessive hyperventilation, causing maternal and fetal respiratory alkalosis
- Cardiac output increases ~50% in first stage and up to 80% in second stage
- Pain from 1st stage: visceral - carried by T10-L1 (uterine body, cervix)
- Pain from 2nd stage: somatic - carried by S2-S4 (perineum, vagina)
Abnormal Labour Patterns to Know
| Pattern | Definition |
|---|---|
| Prolonged latent phase | >20 hr (nullipara) or >14 hr (multipara) |
| Protracted active phase | <1.2 cm/hr dilation (nullipara) or <1.5 cm/hr (multipara) by Friedman criteria |
| Arrest of active phase | No cervical dilation for ≥2 hours in active phase |
| Prolonged 2nd stage | >2 hr without epidural or >3 hr with epidural (nullipara); >1 hr / 2 hr (multipara) |
Sources: Creasy & Resnik's Maternal-Fetal Medicine, Principles and Practice; Textbook of Family Medicine, 9e; Morgan & Mikhail's Clinical Anesthesiology, 7e
This is a shared conversation. Sign in to Orris to start your own chat.