Management of malignant pleural effusion full details for md exam answer 15 marks
Reading File
Finding Sources
Searching PubMed
"malignant pleural effusion" AND management
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full MD exam answer.
Management of Malignant Pleural Effusion (MPE)
Complete MD Examination Answer (15 Marks)
Definition
A malignant pleural effusion (MPE) is defined as the accumulation of fluid in the pleural space with malignant cells or tumor tissue confirmed on pleural fluid cytology or pleural biopsy in a patient with an underlying malignancy. — Fishman's Pulmonary Diseases and Disorders
Epidemiology & Prognosis
- Affects approximately 15% of all cancer patients
- Accounts for >125,000 hospitalizations/year in the USA
- Median survival: 3–12 months (ranges 3–11 months depending on primary tumor type; ~5 months overall)
- Presence of MPE denotes advanced-stage/disseminated disease with poor overall prognosis
Etiology — Common Primary Malignancies
| Cancer Type | Frequency |
|---|---|
| Lung (most common) | ~38% (adenocarcinoma most frequent) |
| Breast | ~15% |
| Haematologic (lymphoma/leukaemia) | ~11% |
| Gastrointestinal | ~11% |
| Gynaecological (ovarian) | ~9% |
| Unknown primary | ~10% |
The "Big Three" — lung, breast, and lymphoma — account for ~75% of all MPEs.
— Harrison's Principles of Internal Medicine 22E; Fishman's
Pathophysiology
Normal pleural fluid balance depends on net filtration pressure minus lymphatic reabsorption via parietal pleural lymphatic stomata (2–12 μm openings draining toward mediastinal lymph nodes).
MPE forms through:
- Lymphatic obstruction — tumour infiltrates lymphatic channels between parietal pleura and mediastinal nodes, reducing reabsorption
- Increased vascular permeability — plasma leakage through hyperpermeable pleural vasculature (now recognised as the primary driver)
- VEGF-mediated mechanism — VEGF (from tumour and host cells) is a powerful angiogenic factor and potent stimulator of vascular hyperpermeability; levels are markedly higher in MPE vs. non-malignant effusions
- Inflammatory cascade — NF-κB and STAT3 transcriptional programs → release of TNF-α, IL-6, CCL2, osteopontin → further effusion formation
- Direct extension / lymphangitic spread — tumour cells metastasise through pulmonary vasculature → visceral pleura → parietal pleura
— Fishman's Pulmonary Diseases and Disorders, block16
Clinical Features
- Dyspnea (most common; often disproportionate to effusion size)
- Cough, pleuritic chest pain, weight loss
- Dullness to percussion, reduced breath sounds, tracheal deviation (large effusions)
- Effusion is usually unilateral, moderate-to-large, and recurrent
Diagnosis
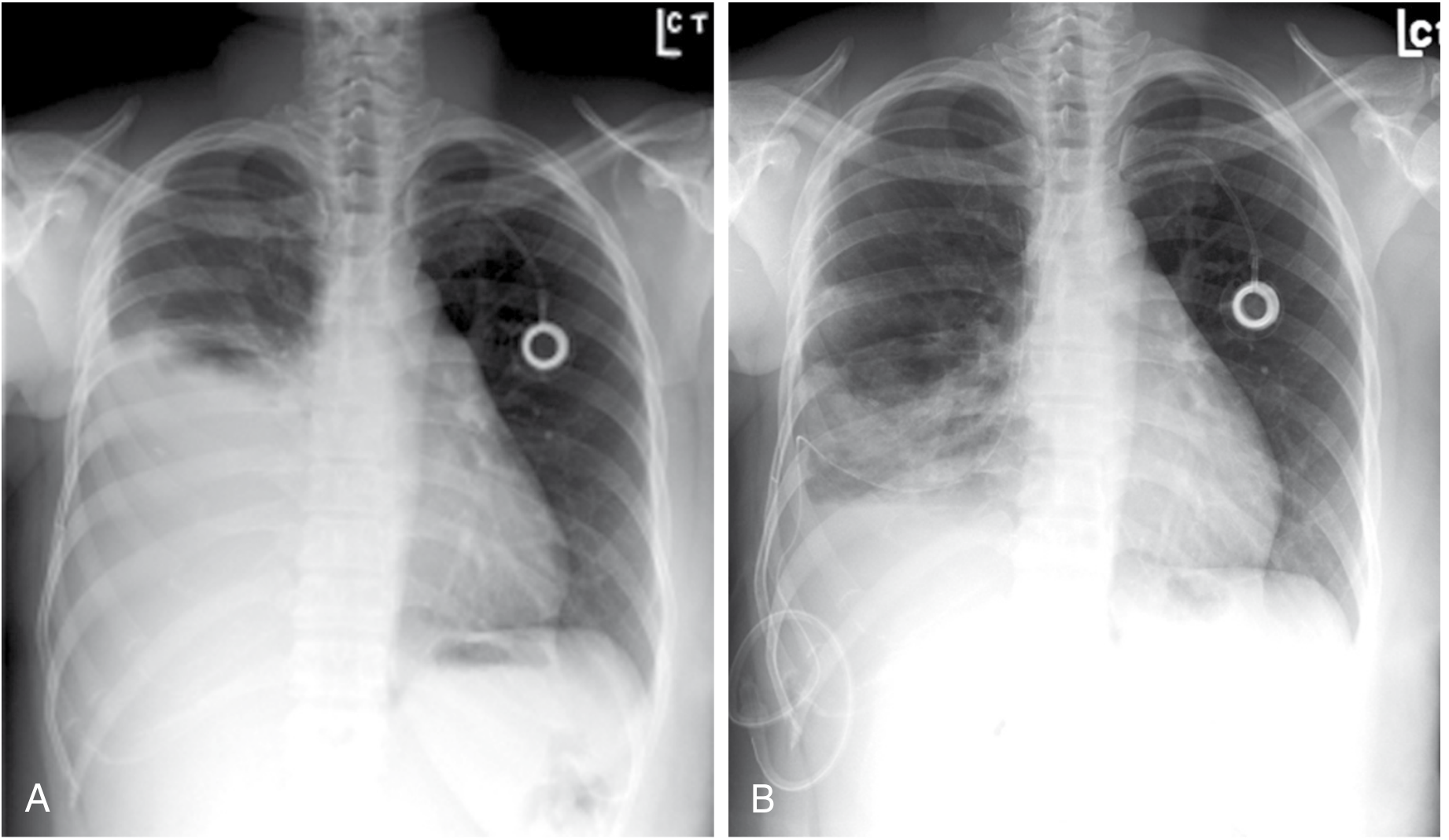
1. Imaging
- Chest X-ray: blunting of costophrenic angle (>300 mL), opacification, mediastinal shift
- CT chest: pleural nodularity, thickening, loculations, primary tumour identification
- Ultrasound: confirms effusion, guides thoracentesis (preferred guidance modality)
2. Pleural Fluid Analysis
- Exudate by Light's criteria (typically): protein >3 g/dL, LDH elevated, pleural:serum protein >0.5, pleural:serum LDH >0.6 — (can rarely be transudative)
- Glucose: may be reduced (<60 mg/dL) with high tumour burden
- Appearance: often haemorrhagic/blood-tinged
- pH: <7.2 portends poor response to pleurodesis
- Cytology: Diagnosis established in ~60% with one thoracentesis; ~80% with repeat thoracentesis
- Sensitivity highest for adenocarcinoma (~70%), lower for mesothelioma (<10%), SCC (~20%), lymphoma (25–50%)
3. Pleural Biopsy
- Image-guided (CT/US) needle biopsy of pleural thickening or nodules if cytology negative
- Medical thoracoscopy / VATS: most definitive — allows direct visualisation and targeted biopsy; sensitivity >90% for malignancy. Indicated if cytology remains non-diagnostic and malignancy strongly suspected
- Cell-free DNA from pleural fluid supernatant can detect driver mutations (e.g., EGFR)
--- Goldman-Cecil Medicine; Murray & Nadel's; Harrison's
Management
General Principles
- Management is palliative — goals are symptom relief (especially dyspnea) and minimising repeat invasive procedures
- Asymptomatic effusions — observation acceptable; treat underlying malignancy if responsive
- Before invasive treatment, confirm dyspnea improves after a therapeutic thoracentesis (test drainage)
- Assess for lung re-expansion post-drainage (CXR, pleural manometry) — crucial for deciding treatment strategy
Algorithm Based on Lung Expandability
MPE confirmed
│
├─ Asymptomatic ──────────────────► Observe / treat primary malignancy
│
└─ Symptomatic
│
├─ Responds to systemic therapy (breast cancer, lymphoma, SCLC)
│ └──► Chemotherapy/hormone therapy first
│
└─ Does not respond / large symptomatic effusion
│
├─ SHORT life expectancy / poor performance status
│ └──► Repeated therapeutic thoracentesis
│
└─ LONGER life expectancy / GOOD PS
│
├─ EXPANDABLE LUNG
│ ├──► Talc pleurodesis (VATS poudrage OR chest tube slurry)
│ └──► Indwelling Pleural Catheter (IPC/TPC)
│
└─ NON-EXPANDABLE "TRAPPED" LUNG
└──► Indwelling Pleural Catheter (IPC) ONLY
— Schwartz's Surgery; Murray & Nadel's; Goldman-Cecil
A. Therapeutic Thoracentesis
- Indication: symptomatic relief in patients with short life expectancy or as a diagnostic step
- Removes 1–1.5 L at a time (limit to avoid re-expansion pulmonary oedema)
- Safe, outpatient procedure under ultrasound guidance
- Limitation: effusion invariably recurs; not definitive for recurrent MPE
B. Chemical Pleurodesis
Goal: obliterate the pleural space to prevent fluid re-accumulation
Pre-requisites:
- Lung must be expandable (trapped lung → pleurodesis will fail)
- Pleural fluid pH >7.2 (pH <7.2 → poor response)
- Patient suitable for procedure
Sclerosing Agents (in order of efficacy):
| Agent | Route | Success Rate | Notes |
|---|---|---|---|
| Talc (best) | VATS poudrage or slurry via chest tube | 60–90% (highest) | Gold standard; 4 g talc in 50 mL saline for slurry |
| Doxycycline | Bedside via chest tube/pigtail | 60–80% | Tetracycline derivative |
| Bleomycin | Bedside via chest tube | ~60% | Expensive |
| Minocycline | Bedside | ~60% |
Methods of Pleurodesis:
- VATS (Video-Assisted Thoracoscopic Surgery) with talc poudrage — preferred: talc aerosolised under direct thoracoscopic vision; allows biopsy simultaneously; highest success rates
- Chest tube (tube thoracostomy) with talc slurry — bedside; insert 12–14 Fr catheter, drain completely, instil 4 g talc in 50 mL NS, clamp for 1–2 hours, rotate patient, then reopen to suction
- Mechanical pleurodesis / pleurectomy — reserved for failed chemical pleurodesis with reasonable life expectancy
Mechanism of pleurodesis: chemical inflammation → fibrous symphysis between parietal and visceral pleura → obliteration of pleural space
— Schwartz's Surgery; Murray & Nadel's; Goldman-Cecil
C. Indwelling (Tunnelled) Pleural Catheter (IPC/TPC)
Primary indications:
- Non-expandable / trapped lung (pleurodesis will fail)
- Patient preference for outpatient management
- Failed previous pleurodesis
- Pleural loculations
- Limited life expectancy (avoids hospitalisation)
- Poor performance status
Device: 15.5-gauge fenestrated silicone catheter tunnelled subcutaneously; connected to one-way valve drainage bottles; drainage performed at home by patient/carer
Technique:
- Position: oblique/decubitus with effusion side up
- Ultrasound-guided: two incisions — pleural insertion site + exit site 5–8 cm lateral and caudal
- Catheter tunnelled subcutaneously from caudal-lateral to cranial-medial incision
- Seldinger technique with J-wire and peel-away introducer
- Placed in 6th–7th intercostal space posterolaterally (serratus anterior–latissimus dorsi junction)
Outcomes:
- Effective symptom control
- ~50% achieve spontaneous pleurodesis (autopleurodesis) over weeks with daily drainage
- Daily drainage > every-other-day for achieving pleurodesis
- Adding intrapleural talc through IPC further increases pleurodesis rates (LCAT trial)
- Dramatically changed end-stage cancer management — avoids hospitalisation
IPC vs. Talc Pleurodesis: equivalent for dyspnea relief (TIME2 trial, AMPLE trial); IPC shortens hospital stay but more adverse effects; choice depends on patient preference and life expectancy
— Schwartz's Surgery; Murray & Nadel's; Fishman's; Goldman-Cecil
D. Treatment of Underlying Malignancy
Effusions related to the following tumours may respond to systemic therapy and avoid need for local drainage:
- Breast cancer — hormone therapy, chemotherapy
- Small cell lung carcinoma (SCLC) — chemotherapy highly effective
- Lymphoma — chemotherapy ± radiotherapy
E. Other / Special Situations
| Situation | Management |
|---|---|
| Loculated MPE | Intrapleural fibrinolytics (tPA + DNase or urokinase) to break loculations; then drainage/pleurodesis |
| Failed pleurodesis with expandable lung | Pleurectomy (surgical) if good performance status |
| Chylothorax from lymphoma | VATS talc pleurodesis or ligation of thoracic duct |
| Mesothelioma | IPC or pleurodesis; cytoreductive surgery + HIPEC in selected cases |
| Paramalignant effusion (non-direct) | Treat underlying cause (PE → anticoagulation; atelectasis → bronchoscopy) |
Post-Procedure Monitoring
- Chest X-ray after drainage to confirm re-expansion
- Monitor for re-expansion pulmonary oedema (do not drain >1.5 L at a time)
- If lung fails to expand → consider pneumothorax ex vacuo, trapped lung → IPC preferred
- IPC complications: infection (~5%), catheter blockage, tumour seeding (rare), cellulitis
Summary Table — Management Options
| Modality | Best For | Key Advantage | Limitation |
|---|---|---|---|
| Therapeutic thoracentesis | Short life expectancy, initial Rx | Simple, outpatient | Recurrence inevitable |
| Talc poudrage (VATS) | Expandable lung, longer life expectancy | Highest pleurodesis success (up to 90%) | General anaesthesia required |
| Talc slurry (chest tube) | Moderate performance status | Bedside, no GA | Slightly lower success than VATS |
| IPC/TPC | Trapped lung, failed pleurodesis, outpatient preference | Outpatient, spontaneous pleurodesis in ~50% | Infection risk, requires nursing |
| Systemic therapy | Chemosensitive tumours (SCLC, breast, lymphoma) | Treats disease | Limited applicability |
| Pleurectomy | Failed all else, good PS | Definitive | Major surgery, morbidity |
Recent Evidence (2023–2025)
- Intrapleural fibrinolytic therapy for loculated MPE shows benefit in recent systematic review [PMID: 40294877, Crit Rev Oncol Hematol 2025]
- Emerging data on intrapleural immunotherapy (intrapleural bio-products)
Key Exam Points to Emphasise:
- MPE = exudate, blood-tinged, recurrent — always confirm diagnosis via cytology/biopsy before definitive management
- Lung expandability is the pivotal decision point: expandable → pleurodesis or IPC; trapped lung → IPC only
- Talc is the best sclerosant (success 60–90%)
- IPC allows outpatient management and achieves autopleurodesis in ~50%
- Pleural fluid pH <7.2 → poor pleurodesis response → prefer IPC
- Management is palliative — goal is quality of life, not cure
Sources: Schwartz's Principles of Surgery 11e; Sabiston Textbook of Surgery; Murray & Nadel's Textbook of Respiratory Medicine; Fishman's Pulmonary Diseases and Disorders; Harrison's Principles of Internal Medicine 22e; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.