i m not getting idea ike how to start from basics
Asking for Preferences
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Great — now I have enough to give you a solid, structured starting roadmap. Here it is:
Starting Physiotherapy from Basics — A Practitioner's Roadmap
Since you're already a practitioner, the goal here isn't to memorize everything from scratch — it's to build a strong conceptual framework so the clinical pieces connect logically. Here's how to structure your learning:
🧱 Layer 1 — The Foundation Sciences (Start Here)
These are what everything in physio sits on top of.
1. Anatomy
Focus on musculoskeletal anatomy first — bones, joints, muscles, ligaments, nerves.
- Key topics: Origin/insertion of muscles, joint structure, nerve innervation, dermatomes/myotomes
- Resources in the library: Gray's Anatomy for Students, THIEME Atlas — General Anatomy and Musculoskeletal System, Netter's Atlas of Human Anatomy
2. Physiology
Understand how muscles and nerves work before you try to rehabilitate them.
- Key topics: Skeletal muscle mechanics, muscle fiber types (Type I vs II), neuromuscular junction, proprioception, motor units
- Resources: Guyton and Hall Textbook of Medical Physiology, Costanzo Physiology 7th Ed
3. Biomechanics
This is where anatomy meets movement.
- Key topics: Range of motion (ROM), joint kinematics, force-couple relationships, lever systems, gait cycle
- Resources: THIEME Atlas has detailed ROM data for each joint; Imaging Anatomy — Bones, Joints covers normal joint biomechanics
🏗️ Layer 2 — Core Physiotherapy Concepts
Once foundation is solid, move into:
| Topic | What to Learn |
|---|---|
| Assessment | Posture analysis, ROM measurement (goniometry), manual muscle testing (MMT), special orthopedic tests |
| Exercise Physiology | FITT principle, strength vs endurance training, progressive overload, VO₂ max |
| Electrotherapy basics | TENS, ultrasound therapy, interferential therapy — indications & contraindications |
| Manual therapy | Joint mobilization grades (Maitland), soft tissue techniques, massage |
| Pain science | Gate control theory, central sensitization, biopsychosocial model |
🔬 Layer 3 — Condition-Based Learning (Apply It)
Once you know the basics, study conditions by region:
- Spine — LBP, cervical spondylosis, disc prolapse, postural syndromes
- Lower limb — knee OA, ACL rehab, ankle sprains, hip fractures
- Upper limb — rotator cuff tears, frozen shoulder (adhesive capsulitis), tennis elbow
- Neuro — stroke rehab, Parkinson's, spinal cord injury
📅 Suggested Weekly Flow to Get Started
| Week | Focus |
|---|---|
| Week 1–2 | Skeletal muscle anatomy + muscle physiology (fiber types, contraction) |
| Week 3–4 | Joint biomechanics + ROM for major joints |
| Week 5–6 | Basic assessment techniques (posture, MMT, goniometry) |
| Week 7–8 | One clinical condition end-to-end (e.g., ACL rehab) |
💡 Practical Tips as a Practitioner
- Don't start with conditions — start with mechanism. Ask "why does this exercise help?" before "which exercise?"
- Use a body region at a time — don't try to learn the whole body simultaneously. Master shoulder → then knee → then spine.
- Active recall beats re-reading — after reading a topic, close the book and write down the key points from memory.
- Link everything to a patient — for every concept you learn, think of a patient case where it applies.
Want me to go deeper on any specific layer — for example, start with muscle physiology, joint biomechanics, or a specific body region or condition?
anatomy how to start like clinical
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Searching Images
musculoskeletal anatomy clinical physiotherapy shoulder knee spine
Here's a complete, clinically-oriented guide to starting anatomy as a physiotherapy practitioner.
Clinical Anatomy for Physiotherapists — How to Start
The biggest mistake people make is studying anatomy the way medical students do — memorising every muscle name in a table. As a physio, you need functional, applied anatomy — understanding what structures do, where to find them, and what goes wrong when they're injured.
The Core Principle: Always Link Structure → Function → Dysfunction
For every structure you study, ask 3 questions:
- What does it do? (function)
- How do I find it on a patient? (surface/palpation anatomy)
- What happens when it fails? (clinical relevance)
Step 1 — Start With a Single Region, Not the Whole Body
Don't try to learn all anatomy at once. Pick one region and go deep.
Best starting region for physios: The Shoulder
Why? It's complex, clinically rich, and you'll immediately apply everything.
Step 2 — The 5-Layer Approach for Each Region
Work through these layers in order for whichever body region you choose:
Layer 1 — Bones & Joint
- Name the bones, identify bony landmarks you can palpate
- Understand the joint type (ball-and-socket, hinge, etc.) and what movements it allows
- Example for shoulder: Humerus, scapula, clavicle → glenohumeral joint (ball-and-socket) → allows flexion, extension, abduction, adduction, IR/ER, circumduction
Layer 2 — Ligaments & Joint Stability
- Which ligaments hold the joint together?
- What stresses injure them?
- Example: Glenohumeral ligaments (superior, middle, inferior) → inferior GHL is the primary restraint to anterior dislocation
Layer 3 — Muscles (Origin → Insertion → Action → Nerve)
- Always learn muscles as functional groups, not individual names
- Example: Rotator cuff = SITS (Supraspinatus, Infraspinatus, Teres Minor, Subscapularis) → dynamic stabilizers of GH joint
Layer 4 — Nerves & Blood Supply
- Which nerve supplies which muscle? (myotomes)
- Which nerve supplies which skin area? (dermatomes)
- Why it matters: A patient with shoulder pain + weak deltoid + numb lateral arm → axillary nerve injury
Layer 5 — Surface Anatomy & Palpation
- Can you find it on a real person?
- What are the bony landmarks? (e.g., coracoid process, acromion, greater tuberosity)
Step 3 — Use Clinical Images, Not Just Diagrams
Here are actual clinical anatomy images relevant to physiotherapy:
MRI cross-sections: shoulder, hip, knee, spine
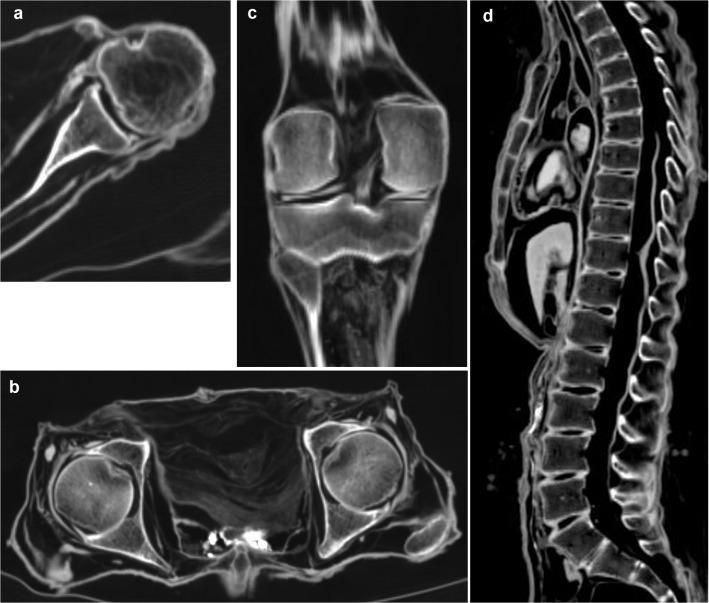 Axial shoulder MRI showing rotator cuff, glenohumeral joint, biceps tendon; coronal knee MRI showing PCL, menisci; sagittal spine MRI
Axial shoulder MRI showing rotator cuff, glenohumeral joint, biceps tendon; coronal knee MRI showing PCL, menisci; sagittal spine MRI
Sitting Knee Extension Test — lumbopelvic motor control
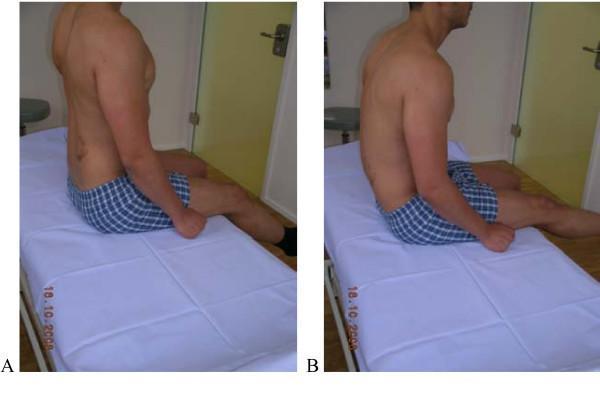 Clinical assessment: correct posture (L) vs compensatory lumbar flexion (R) — anatomy directly driving clinical decision-making
Clinical assessment: correct posture (L) vs compensatory lumbar flexion (R) — anatomy directly driving clinical decision-making
Hamstring flexibility (AKE test) + Lumbar ROM (modified Schober)
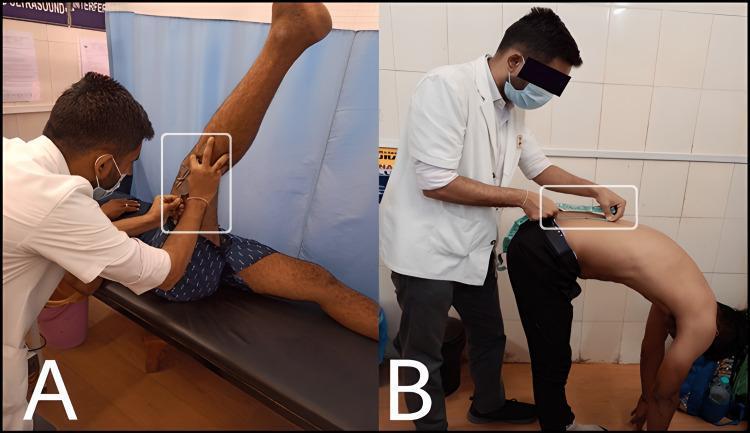 Goniometry and Schober's test — anatomy directly measured in clinical practice
Goniometry and Schober's test — anatomy directly measured in clinical practice
Trapezius dissection + Myofascial Trigger Points
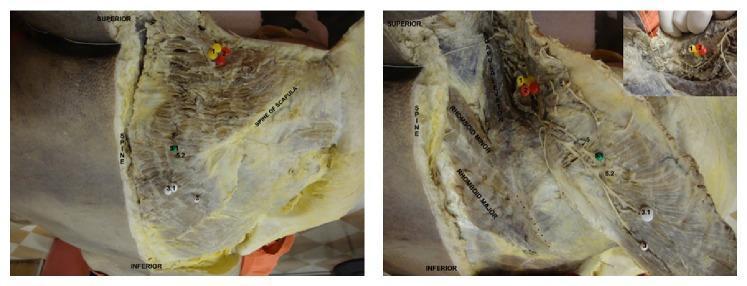 Deep dissection showing spinal accessory nerve branches and clinical trigger points — directly relevant to dry needling and soft tissue work
Deep dissection showing spinal accessory nerve branches and clinical trigger points — directly relevant to dry needling and soft tissue work
Step 4 — Suggested Study Order (Region by Region)
| Week | Region | Key Clinical Application |
|---|---|---|
| 1–2 | Shoulder | Rotator cuff tears, frozen shoulder, impingement |
| 3–4 | Knee | ACL/PCL, meniscus, patellofemoral syndrome |
| 5–6 | Lumbar spine | Disc prolapse, facet joint pain, nerve root compression |
| 7–8 | Hip | OA, labral tears, SIJ dysfunction |
| 9–10 | Cervical spine | Cervicogenic headache, nerve root compression |
| 11–12 | Ankle/Foot | Ligament sprains, Achilles tendinopathy, plantar fasciitis |
| 13–14 | Elbow/Wrist | Tennis elbow, CTS, TFCC injuries |
Step 5 — How to Study Each Session (Practical Method)
- Draw the joint from memory — even badly. It forces recall.
- Palpate on yourself or a colleague — feel the bony landmarks.
- Read one clinical condition related to that anatomy (e.g., after learning the rotator cuff → read about supraspinatus tears).
- Ask: "How would I assess this in a patient?" — connects anatomy to clinical reasoning.
Best Books Available (from your library)
| Book | Best Used For |
|---|---|
| THIEME Atlas — General Anatomy & Musculoskeletal System | Detailed muscle/joint anatomy with illustrations |
| Netter's Atlas of Human Anatomy | Visual reference, best for surface anatomy and orientation |
| Gray's Anatomy for Students | Detailed functional anatomy with clinical boxes |
| Imaging Anatomy — Bones, Joints, Vessels & Nerves | MRI/CT anatomy — great for understanding imaging reports |
| Miller's Review of Orthopaedics | ROM, clinical tests, condition-based anatomy |
Where do you want to go next? Should we start with the shoulder in detail (bones → muscles → nerves → clinical tests), or would you prefer a different region?
This is a shared conversation. Sign in to Orris to start your own chat.