fully detailed structred notes on descending tracts ( use standard physiology books like Guyton and hall and Ganong etc. as your source)try to add some diagrams and also flowcharts
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive, high-quality content from multiple authoritative textbooks plus several excellent diagrams. Let me now compile the full structured notes with all diagrams and flowcharts.
DESCENDING TRACTS OF THE SPINAL CORD
Fully Detailed Structured Notes
Sources: Guyton & Hall Textbook of Medical Physiology (14e), Ganong's Medical Physiology (Medical Physiology - Boron & Boulpaep), Gray's Anatomy for Students (5e), Neuroscience: Exploring the Brain (5e), Bradley & Daroff's Neurology in Clinical Practice, Neuroanatomy through Clinical Cases (3e)
PART 1: OVERVIEW AND CLASSIFICATION
1.1 Definition and Purpose
Descending tracts are bundles of axons in the white matter of the spinal cord that carry signals from the brain downward to influence motor neurons and interneurons in the spinal cord gray matter. They regulate:
- Voluntary movements
- Postural adjustments and balance
- Coordination of head, neck, and eye movements
- Autonomic outflow
- Modulation of sensory input
1.2 Upper Motor Neuron (UMN) vs. Lower Motor Neuron (LMN)
Every descending tract has two-neuron structure:
| Feature | Upper Motor Neuron (UMN) | Lower Motor Neuron (LMN) |
|---|---|---|
| Location of cell body | Cerebral cortex or brainstem | Anterior horn of spinal cord (or cranial nerve nuclei) |
| Axon travels through | Descending tract in white matter | Peripheral nerve to muscle |
| Neurotransmitter | Glutamate | Acetylcholine |
| Effect on LMN | Excitatory + inhibitory modulation | Direct muscle contraction |
| Lesion sign | Spasticity, hyperreflexia, Babinski+ | Flaccid paralysis, hyporeflexia, fasciculations |
(Guyton & Hall, Ch. 56; Bradley & Daroff's Neurology, Ch. 97)
1.3 Two-System Classification
The most clinically important classification divides descending tracts into two functional systems:
DESCENDING MOTOR TRACTS
|
┌────────────────┴────────────────┐
│ │
LATERAL SYSTEM VENTROMEDIAL SYSTEM
(Lateral column) (Anterior column)
│ │
Fine voluntary movement Posture, balance,
of distal muscles locomotion, axial muscles
(Cortical control) (Brainstem control)
│ │
┌──────┴──────┐ ┌───────────┼───────────┐
│ │ │ │ │
Lateral Rubro- Vestibulo- Reticulo- Tecto-
Cortico- spinal spinal spinal spinal
spinal tract tracts tracts tract
tract
(Neuroscience: Exploring the Brain, 5e, Ch. 14)
PART 2: THE LATERAL SYSTEM
2.1 LATERAL CORTICOSPINAL TRACT (LCST)
Also called: Pyramidal tract
The most important and most studied descending pathway.
Spinal cord cross-section showing all descending tract positions:
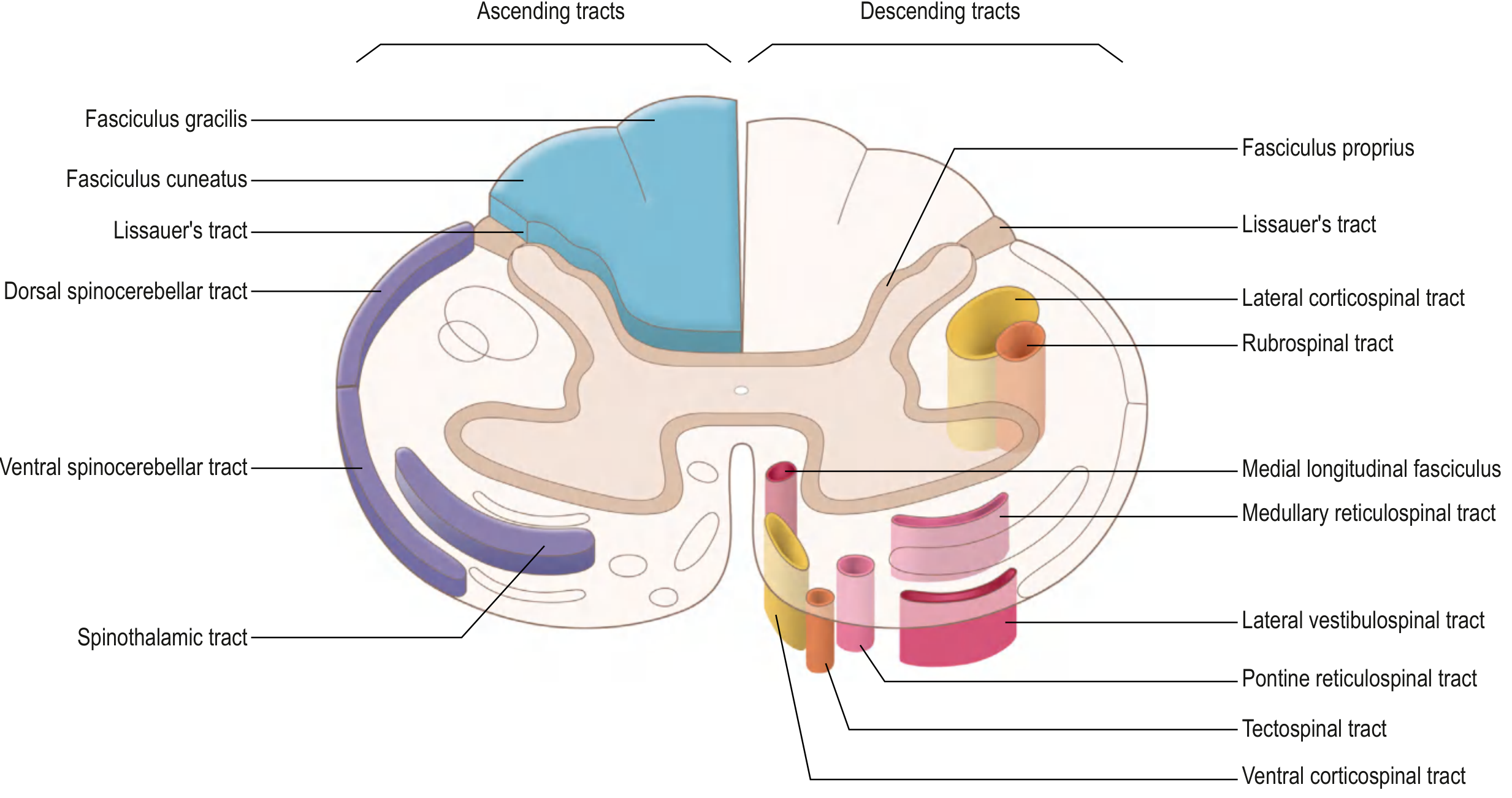
Gray's Anatomy for Students (eFig. 9.42): Cross-section of spinal cord showing descending tracts on right and ascending tracts on left. Lateral corticospinal and rubrospinal tracts occupy the lateral column; ventromedial tracts occupy the anterior column.
2.1.1 Origin
- 30% from primary motor cortex (Area 4, Brodmann) - Betz cells (giant pyramidal cells) in Layer V
- 30% from premotor cortex and supplementary motor area (Area 6)
- 40% from somatosensory cortex (Areas 3, 1, 2) - these fibers modulate sensory input
- Total fibers: >1 million per tract
- Betz cell fibers (largest, ~16 µm diameter): only ~34,000 = 3% of total; conduct at 70 m/sec
- Remaining 97% are small (<4 µm), conducting tonic background signals
(Guyton & Hall, Ch. 56)
2.1.2 Course - Complete Pathway
Primary Motor Cortex (Area 4) + Premotor/SMA (Area 6) + Somatosensory Cortex
↓
Converge in CORONA RADIATA
↓
POSTERIOR LIMB of INTERNAL CAPSULE
(between caudate nucleus and putamen)
↓
CRUS CEREBRI (Cerebral Peduncle) - midbrain, middle 3/5
↓
LONGITUDINAL FASCICLES of PONS
(dispersed by transverse pontocerebellar fibers)
↓
PYRAMID of MEDULLA OBLONGATA
(re-forms into compact bundle on ventral surface)
↓
PYRAMIDAL DECUSSATION (cervicomedullary junction)
~85% of fibers cross to contralateral side
↓
LATERAL CORTICOSPINAL TRACT
(lateral column of spinal cord, entire length)
↓
Synapse on INTERNEURONS in intermediate gray matter
and lateral aspect of ANTERIOR HORN
→ Lower motor neurons → Skeletal muscle
(predominantly cervical and lumbosacral enlargements)
The uncrossed 15% descend ipsilaterally as the anterior (ventral) corticospinal tract, and most eventually cross in the cord at cervical/upper thoracic levels via the anterior white commissure.
(Guyton & Hall, Ch. 56; Gray's Anatomy for Students, eFig. 9.45)
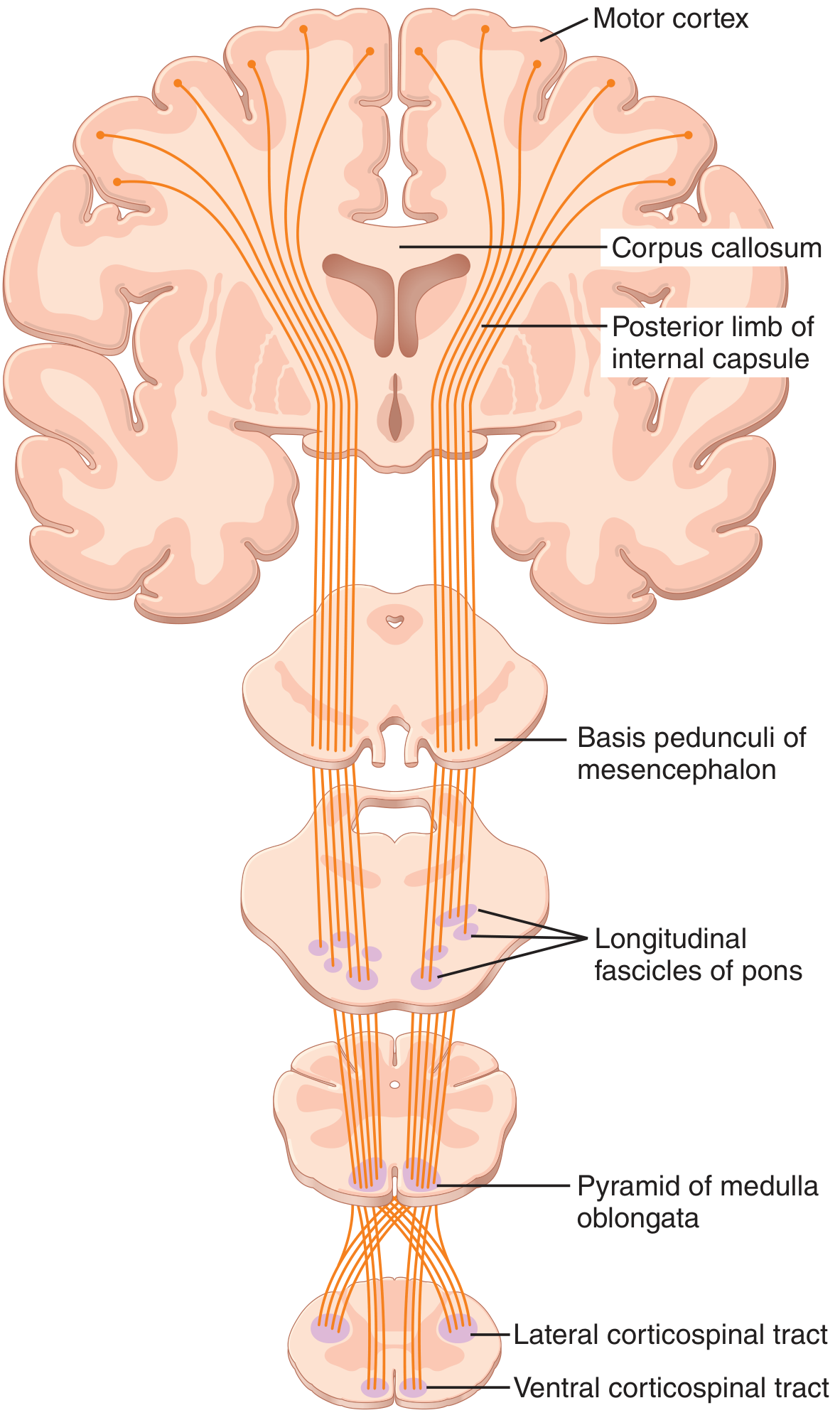
Corticospinal tract diagram (Guyton & Hall, Figure 56.4):
Lateral pathways - corticospinal and rubrospinal tract course and termination:
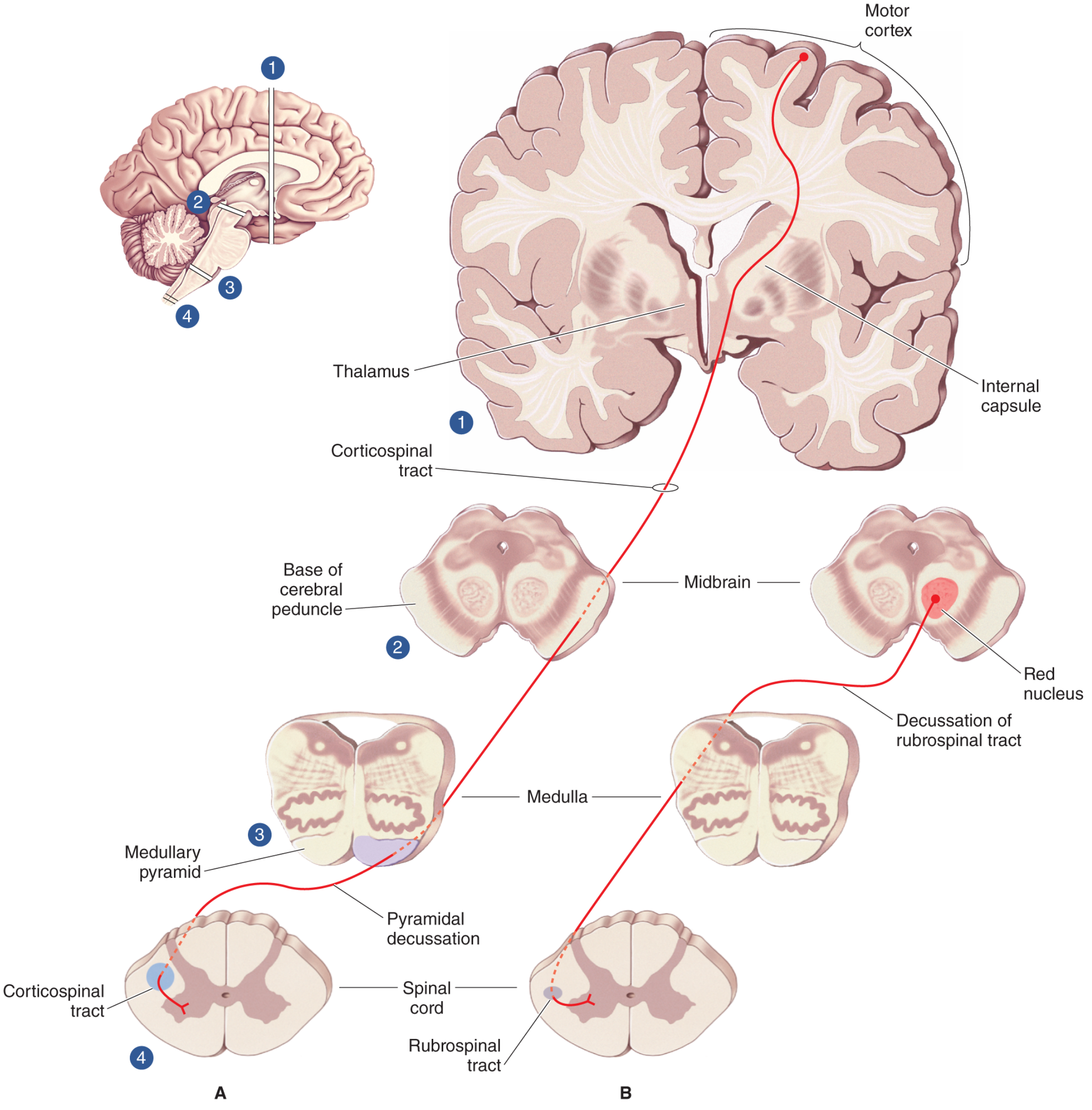
Neuroscience: Exploring the Brain (Fig. 14.4): Origins and terminations of the corticospinal tract (A) and rubrospinal tract (B).
2.1.3 Somatotopic Organization in Internal Capsule
In the posterior limb of the internal capsule, fibers are arranged somatotopically:
- Head and neck: anterior-most
- Upper limb: middle
- Lower limb: most posterior (near genu)
This explains why small internal capsule strokes (e.g., lacunar infarcts) can cause selective limb weakness.
2.1.4 Termination and Function
- Terminates mainly on interneurons in the intermediate zone (Rexed laminae IV-VII)
- Some fibers terminate directly on alpha motor neurons (Rexed lamina IX) - more so at cervical levels for fine hand control
- A few terminate on dorsal horn neurons to modulate sensory transmission
Primary Function: Control of fine, skilled, voluntary movement of contralateral distal limb muscles (especially hand and finger movements). The hand and speech areas account for >50% of primary motor cortex representation.
(Guyton & Hall, Ch. 56)
2.2 ANTERIOR (VENTRAL) CORTICOSPINAL TRACT
| Feature | Detail |
|---|---|
| Origin | Same as LCST - primary motor cortex + SMA |
| Decussation | Does NOT cross in medulla; crosses at each segmental level via anterior white commissure |
| Location in cord | Anterior (ventral) column, medial |
| Levels | Cervical and upper thoracic only |
| Termination | Medial anterior horn - bilateral |
| Function | Bilateral control of axial and girdle muscles (postural) |
(Gray's Anatomy for Students, eTable 9.6)
2.3 RUBROSPINAL TRACT
2.3.1 Origin and Course
RED NUCLEUS (magnocellular division)
in Midbrain Tegmentum
↓
Immediate DECUSSATION
(Ventral Tegmental Decussation in midbrain)
↓
LATERAL COLUMN of spinal cord
(just anterior to LCST)
↓
Terminates at CERVICAL CORD only
(synapse on interneurons → anterior horn)
2.3.2 Function
- Facilitates flexor muscle activity of upper limbs
- Inhibits extensor muscles
- In humans, the red nucleus is smaller and the rubrospinal tract is less developed - its functional significance in humans is uncertain
- In lower mammals it is important; in primates, the corticospinal tract dominates
- The motor cortex sends fibers to the red nucleus (corticorubral fibers) so the rubrospinal tract may act as an auxiliary motor pathway
(Gray's Anatomy for Students; Neuroscience: Exploring the Brain, Ch. 14; Guyton & Hall, Ch. 56)
PART 3: THE VENTROMEDIAL SYSTEM
These four tracts originate in the brainstem and use sensory information about balance, body position, and the visual environment to maintain posture and coordinate gait.
Key rule: Lateral pathways = voluntary distal movement (cortical control); Ventromedial pathways = postural/axial control (brainstem control). - Neuroscience: Exploring the Brain
Ventromedial pathways in spinal cord cross-section:
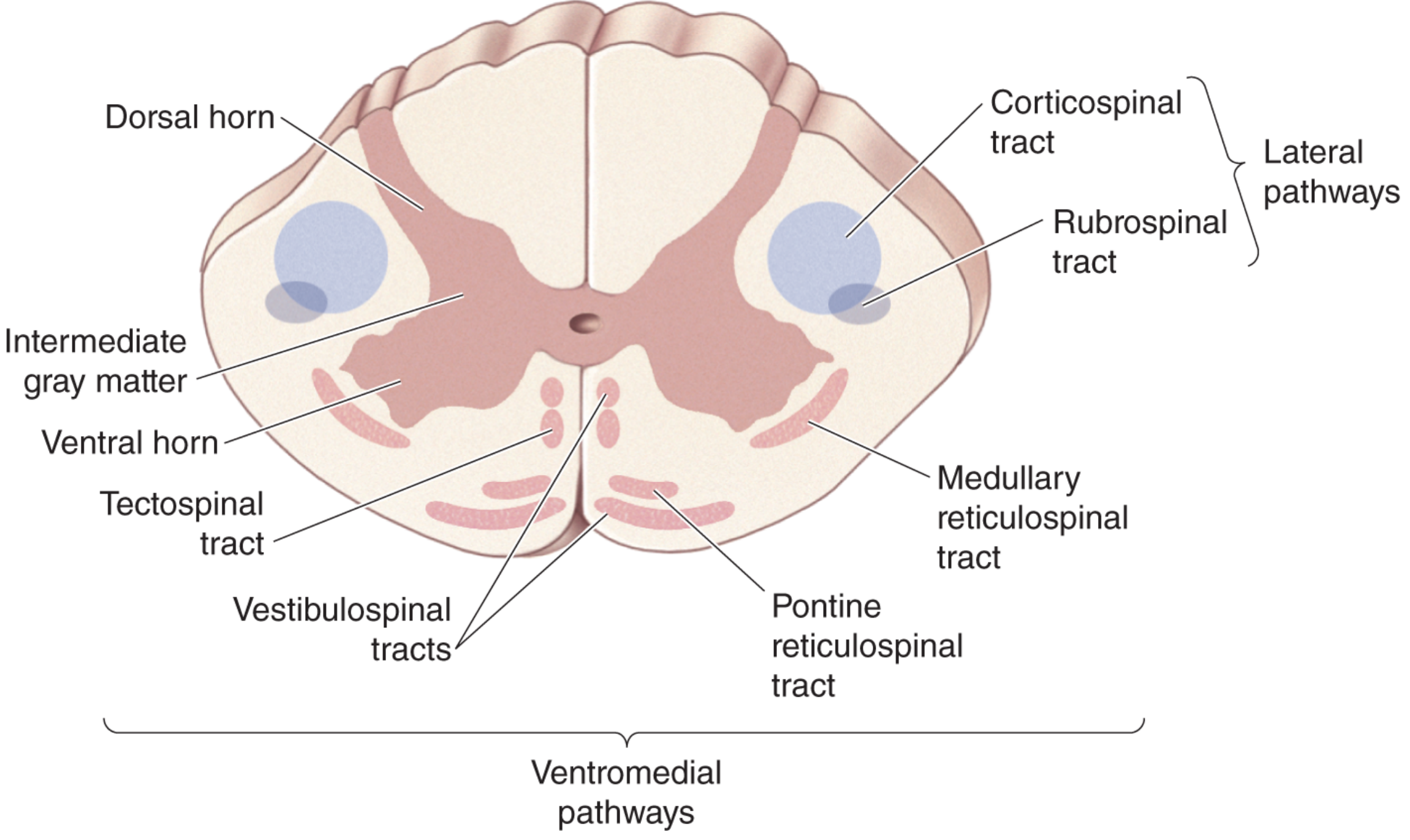
Neuroscience: Exploring the Brain (Fig. 14.3): Lateral pathways (blue) control fine distal movements; ventromedial pathways (pink) control postural muscles.
3.1 VESTIBULOSPINAL TRACTS (VST)
Two subdivisions:
3.1.1 Lateral Vestibulospinal Tract (LVST)
| Feature | Detail |
|---|---|
| Origin | Lateral vestibular nucleus (Deiters' nucleus) in pons/medulla |
| Input to origin | Vestibular hair cells via CN VIII; cerebellum (vermis) |
| Decussation | None - descends ipsilaterally |
| Location in cord | Anterior/ventral column |
| Extent | Entire length of spinal cord (to lumbar) |
| Termination | Interneurons in anterior horn - medial |
| Function | Facilitates extensors (antigravity muscles), inhibits flexors; maintains upright posture and balance |
3.1.2 Medial Vestibulospinal Tract (MVST)
| Feature | Detail |
|---|---|
| Origin | Medial and inferior vestibular nuclei |
| Decussation | Projects bilaterally |
| Extent | Cervical and upper thoracic cord only |
| Function | Head and neck muscle positioning; keeps head stable during body movement; coordinates with MLF for vestibuloocular reflex |
(Gray's Anatomy for Students, eTable 9.6; Neuroscience: Exploring the Brain, Ch. 14)
VESTIBULOSPINAL TRACT PATHWAY:
Semicircular canals + Otolith organs (CN VIII)
↓
Vestibular nuclei (pons/medulla)
↓
┌───────────────────────┐
│ │
Lateral VST Medial VST
(ipsilateral) (bilateral)
│ │
↓ ↓
Entire cord Cervical/upper thoracic
│ │
↓ ↓
Extensor facilitation Head/neck positioning
(balance, posture)
Vestibulospinal and tectospinal tract diagrams:
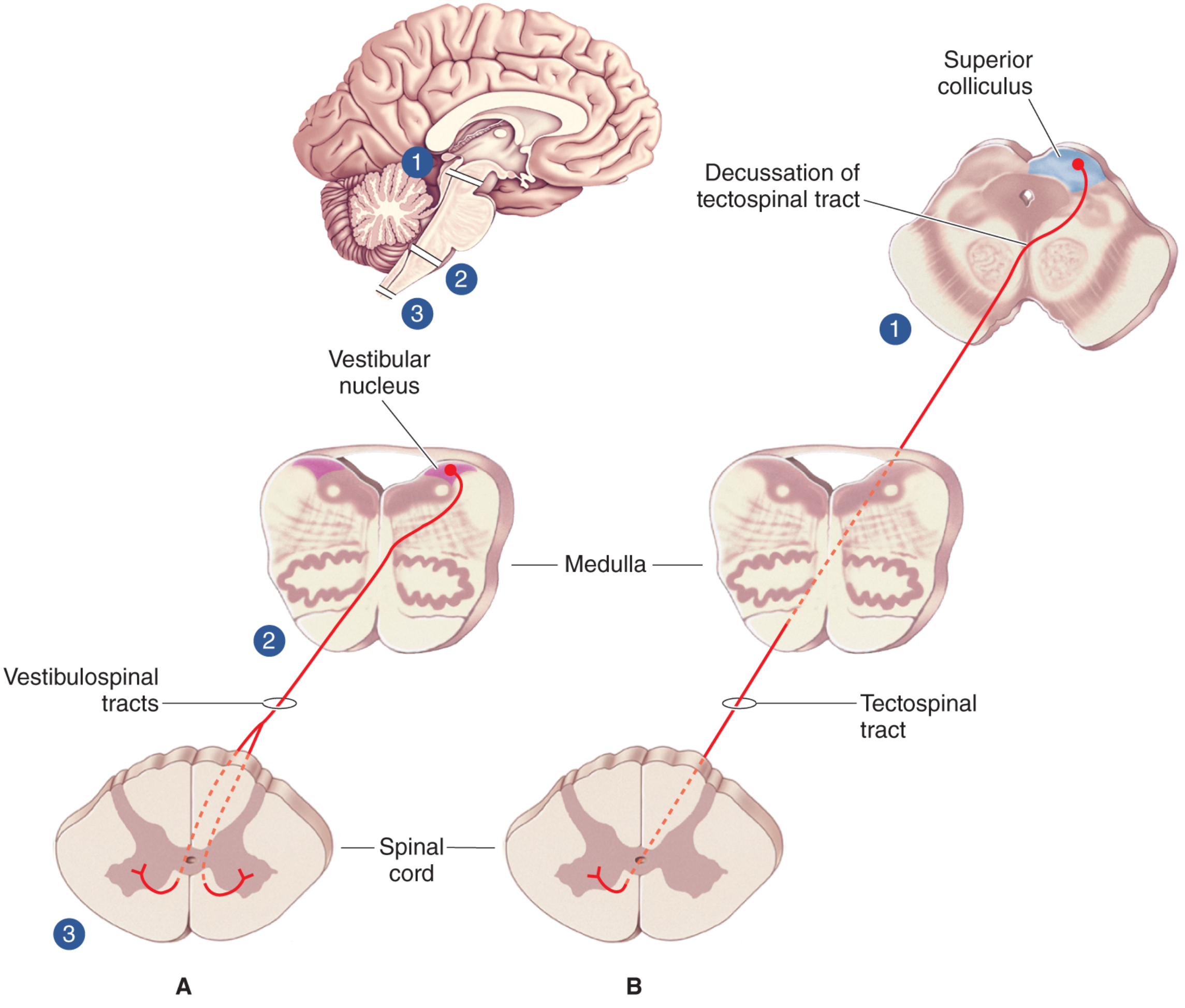
Neuroscience: Exploring the Brain (Fig. 14.5): Vestibulospinal (A) and tectospinal (B) tracts.
3.2 RETICULOSPINAL TRACTS
Two functionally distinct components arising from the reticular formation of the brainstem:
3.2.1 Pontine (Medial) Reticulospinal Tract
| Feature | Detail |
|---|---|
| Origin | Pontine reticular formation (nucleus reticularis pontis caudalis and oralis) |
| Decussation | None - descends ipsilaterally |
| Location | Anterior column (ventromedial) |
| Extent | Entire cord |
| Termination | Medial anterior horn interneurons |
| Effect | Facilitates extensor tone; facilitates antigravity muscles |
| Neurotransmitter | Glutamate (excitatory) |
3.2.2 Medullary (Lateral) Reticulospinal Tract
| Feature | Detail |
|---|---|
| Origin | Medullary reticular formation (nucleus reticularis gigantocellularis) |
| Decussation | None - descends ipsilaterally (some bilateral projections) |
| Location | Lateral part of anterior column |
| Extent | Entire cord |
| Effect | Inhibits extensor tone; inhibits antigravity muscles |
| Neurotransmitter | Glycine/GABA (inhibitory) |
Clinical significance: When the corticospinal tract is damaged (e.g., stroke), the reticulospinal (and vestibulospinal) tracts are released from cortical inhibition and become overactive, producing:
- Upper limb flexor posturing (medullary reticulospinal released)
- Lower limb extensor posturing (pontine reticulospinal + LVST released)
This explains the classic "decerebrate/decorticate posturing" and spasticity seen in UMN lesions.
(Guyton & Hall, Ch. 56; Bradley & Daroff's Neurology, Ch. 97)
RETICULOSPINAL TRACT OVERVIEW:
RETICULAR FORMATION
/ \
PONTINE RF MEDULLARY RF
(Excitatory) (Inhibitory)
↓ ↓
Pontine RST Medullary RST
(ipsilateral) (ipsilateral/bilateral)
↓ ↓
Facilitates extensors Inhibits extensors
↓ ↓
Entire cord Entire cord
Both receive input from:
• Motor cortex (corticoreticular fibers)
• Cerebellum
• Sensory afferents
3.3 TECTOSPINAL TRACT
| Feature | Detail |
|---|---|
| Origin | Superior colliculus of dorsal midbrain |
| Input to origin | Retina; visual/auditory/somatosensory cortex; CN VIII (via IC) |
| Decussation | Dorsal tegmental decussation immediately after leaving nucleus |
| Location in cord | Anterior column (ventromedial) |
| Extent | Cervical cord only (C1-C4) |
| Termination | Interneurons in medial anterior horn |
| Function | Coordinates reflex head and eye turning toward novel visual/auditory stimuli (orienting response); function uncertain in humans |
(Neuroscience: Exploring the Brain, Ch. 14; Gray's Anatomy for Students)
PART 4: CORTICOBULBAR TRACT
Often covered alongside descending tracts as it travels with the corticospinal tract to brainstem cranial nerve nuclei:
| Feature | Detail |
|---|---|
| Origin | Lower primary motor cortex (face area) + premotor cortex |
| Course | Internal capsule (genu) → cerebral peduncle → brainstem |
| Termination | Motor cranial nerve nuclei (V, VII, IX, X, XI, XII) |
| Decussation | Mostly bilateral (CN V, IX, X, XI, XII) except lower face (CN VII) which is contralateral only |
| Function | Voluntary control of face, jaw, pharynx, larynx, tongue |
| Clinical note | Unilateral cortical lesion → spares upper face (bilateral supply), affects lower face contralaterally (UMN VII palsy vs. LMN VII palsy) |
PART 5: COMPREHENSIVE SUMMARY TABLE
| Tract | Origin | Decussation | Column in Cord | Levels | Primary Function |
|---|---|---|---|---|---|
| Lateral CST | Primary motor cortex, premotor, SMA | Pyramidal decussation (medulla) | Lateral | Entire cord | Fine voluntary movement, contralateral distal muscles |
| Anterior CST | Primary motor cortex, SMA | At each cord segment | Anterior | Cervical + upper thoracic | Bilateral axial/girdle muscle control |
| Rubrospinal | Red nucleus (midbrain) | Ventral tegmental decussation (midbrain) | Lateral | Cervical only | Flexor facilitation of upper limb (uncertain in humans) |
| Lateral VST | Lateral vestibular nucleus | None (ipsilateral) | Anterior | Entire cord | Extensor facilitation, balance, posture |
| Medial VST | Medial/inferior vestibular nuclei | Bilateral | Anterior | Cervical + upper thoracic | Head/neck positioning |
| Pontine RST | Pontine reticular formation | None (ipsilateral) | Anterior | Entire cord | Facilitation of extensors |
| Medullary RST | Medullary reticular formation | None (ipsilateral) | Anterior | Entire cord | Inhibition of extensors |
| Tectospinal | Superior colliculus (midbrain) | Dorsal tegmental decussation (midbrain) | Anterior | Cervical only (C1-C4) | Reflex head-turning to stimuli |
| Corticobulbar | Lower motor cortex | Mostly bilateral at brainstem | Not in cord | Brainstem only | Voluntary cranial nerve motor function |
PART 6: CLINICALLY IMPORTANT FLOWCHART - UMN SYNDROME
LESION ABOVE ANTERIOR HORN CELL
(Corticospinal tract + other UMN fibers damaged)
↓
UMN SYNDROME
↓
┌─────────────────────────────────────────┐
│ │
│ IMMEDIATE (Spinal Shock Phase): │
│ • Flaccid paralysis │
│ • Loss of reflexes │
│ • Lasts hours to days │
└────────────┬────────────────────────────┘
↓ (after resolution)
┌─────────────────────────────────────────┐
│ ESTABLISHED UMN SYNDROME: │
│ • Weakness (predominantly distal) │
│ • SPASTICITY (velocity-dependent │
│ resistance to passive stretch) │
│ • HYPERREFLEXIA │
│ • Clasp-knife rigidity │
│ • BABINSKI sign (extensor plantar) │
│ • Loss of dexterity │
│ • CLONUS (rhythmic reflex contractions)│
│ • Absent superficial abdominal reflexes│
└─────────────────────────────────────────┘
↓
Mechanism of Spasticity:
Corticospinal damage → disinhibits VST + RST
→ excess excitatory input (serotonin, NE, glutamate)
to alpha and gamma motor neurons
→ increased muscle spindle activity
→ velocity-dependent resistance to stretch
(Bradley & Daroff's Neurology, Ch. 97; Guyton & Hall, Ch. 56)
PART 7: LOCALIZATION OF LESIONS
7.1 Lesion Level Flowchart
CONTRALATERAL HEMIPLEGIA
(face + arm + leg)
↓
INTERNAL CAPSULE lesion
(most common = lacunar stroke)
CONTRALATERAL HEMIPLEGIA
(arm + leg, face spared or mild)
↓
CORTICAL lesion
(specific homunculus area)
IPSILATERAL LIMB WEAKNESS
+ CONTRALATERAL FACE WEAKNESS
(crossed syndrome)
↓
BRAINSTEM lesion
(above decussation of CST
but affects CN nucleus ipsilaterally)
BILATERAL MOTOR SIGNS
Below level + no cranial nerve signs
↓
SPINAL CORD lesion
(complete transection → bilateral UMN below)
IPSILATERAL UMN signs (arm + leg)
+ IPSILATERAL sensory loss (vibration/proprioception)
+ CONTRALATERAL pain/temp loss
↓
HEMISECTION of spinal cord
(Brown-Séquard syndrome)
7.2 Internal Capsule - Somatotopic Arrangement
| Region | Fibers |
|---|---|
| Anterior limb | Frontopontine fibers, thalamocortical fibers |
| Genu | Corticobulbar fibers (face) |
| Posterior limb (anterior part) | Corticospinal (arm) |
| Posterior limb (middle part) | Corticospinal (leg) |
| Posterior limb (posterior part) | Sensory radiations |
PART 8: POSTURE AND THE CORTICOSPINAL TRACT - INTEGRATION
VOLUNTARY MOVEMENT HIERARCHY:
(Neuroscience: Exploring the Brain, Ch. 14)
STRATEGY (what to do)
Association cortex + Basal ganglia
↓
TACTICS (how to do it - sequences)
Motor cortex + Cerebellum
↓
EXECUTION (final commands)
Alpha motor neurons + Spinal interneurons
↓
MUSCLE CONTRACTION
Key integrating concept from Guyton & Hall (Ch. 56):
When the brain sends a "move" command, it does not have to separately command each synergist, antagonist, and stabilizer. The spinal cord's own interneuron circuits (stretch reflex, reciprocal inhibition, Renshaw cell inhibition) automatically coordinate these details. The corticospinal tract "delegates" the fine-tuning to spinal circuitry.
PART 9: FIBER STATISTICS AND ANATOMY DETAILS
| Tract | Fiber Count | Fiber Size | Conduction Speed |
|---|---|---|---|
| Lateral CST - Betz cell fibers | ~34,000/side | 16 µm | ~70 m/sec |
| Lateral CST - total | >1,000,000/side | Mostly <4 µm | Variable |
| Rubrospinal | Small | Small myelinated | Moderate |
| Vestibulospinal | Moderate | Myelinated | Fast |
(Guyton & Hall, Ch. 56)
PART 10: EFFECTS OF LESIONS IN SPECIFIC TRACTS
10.1 Isolated Corticospinal (Pyramidal) Tract Lesion
(Rare - usually coexists with other pathway damage)
- Loss of fine distal motor control (especially hand/finger dexterity)
- Hypotonia (not spasticity - because reticulospinal/vestibulospinal intact)
- Weakness of distal muscles
- Babinski sign positive (extensor plantar response)
- The classic "pure pyramidal syndrome" produces flaccidity and weakness, NOT spasticity
10.2 Combined CST + Reticulospinal Lesion (Typical Stroke)
- Spasticity (RST disinhibited - excess excitatory tone)
- Upper limb flexion posture (medullary RST)
- Lower limb extension posture (pontine RST + LVST)
- Hyperreflexia + Babinski
- This is the typical UMN syndrome seen clinically
10.3 Spinal Cord Transection
- Spinal shock initially: flaccid paralysis, loss of all reflexes below
- Recovery: UMN syndrome below the level
- Autonomic dysreflexia (above T6)
(Guyton & Hall, Ch. 56; Bradley & Daroff's Neurology, Ch. 97)
PART 11: QUICK REVISION FLOWCHART - All Tracts
ALL DESCENDING TRACTS
|
┌────┴─────┐
│ │
PYRAMIDAL EXTRAPYRAMIDAL
(CST) (All others)
│ │
Voluntary ┌──┴──┐
skilled Post. Brainstem
movement tracts tracts
│ │
Rubro- VST, RST,
spinal Tectospinal
ORIGIN SITES:
• Motor cortex → Corticospinal, Corticobulbar
• Red nucleus → Rubrospinal
• Vestibular nuclei → Vestibulospinal
• Reticular formation → Reticulospinal
• Superior colliculus → Tectospinal
DECUSSATION SITES:
• Lower medulla → Lateral CST (pyramidal decussation)
• Midbrain (ventral) → Rubrospinal
• Midbrain (dorsal) → Tectospinal
• At cord level → Anterior CST
• NONE → Vestibulospinal, Reticulospinal (mostly ipsilateral)
WHAT EACH CONTROLS:
Lateral CST → Contralateral fine hand/finger movement
Anterior CST → Bilateral axial/trunk muscles
Rubrospinal → Contralateral arm flexors (uncertain in humans)
Lat. VST → Ipsilateral extensor/antigravity muscles
Med. VST → Bilateral head/neck muscles
Pontine RST → Ipsilateral extensor facilitation
Medullary RST → Ipsilateral extensor inhibition
Tectospinal → Bilateral head-turning reflexes (cervical only)
PART 12: MEMORY AIDS
"CLUE for Lateral System":
Corticospinal (contralateral, crosses in medulla) + RubroSpinal (crosses in midbrain) = CRS - Crosses, Runs in lateral column, Skilled movement
"VRTM for Ventromedial System":
Vestibulospinal - Reticulospinal - Tectospinal - Anterior corticospinalMedial = All in anterior/ventromedial column, most don't cross
Decussation mnemonic:
- Pyramidal tract crosses at Pyramidal decussation = PoleLower medulla (below)
- Rubrospinal crosses in Midbrain (tegmentum, ventral) - think Midbrain = Muscle (Red)
- Tectospinal crosses in Midbrain (dorsal) - think Tecto = Top (dorsal)
SOURCES
- Guyton and Hall Textbook of Medical Physiology, 14th Edition, Chapter 56 (Cortical and Brain Stem Control of Motor Function), pp. 687-695
- Ganong's / Medical Physiology (Boron & Boulpaep), Chapter 10 (Organization of the Nervous System), pp. 419-420
- Gray's Anatomy for Students, 5th Edition, Chapter 9 (Neuroanatomy), eTables 9.5 and 9.6, pp. 1329-1335
- Neuroscience: Exploring the Brain, 5th Edition, Chapter 14 (Brain Control of Movement), pp. 1323-1330
- Bradley and Daroff's Neurology in Clinical Practice, Chapter 97 (Upper Motor Neurons and Descending Tracts), Box 97.1, pp. 4026-4076
- Neuroanatomy through Clinical Cases, 3rd Edition, Chapter 6 (Corticospinal Tract and Motor Pathways)
Notes are complete. Here is a summary of what is covered:
- Classification into lateral (pyramidal + rubrospinal) vs. ventromedial (VST, RST, tectospinal) systems
- Lateral Corticospinal Tract - full pathway, fiber statistics, somatotopy, function, lesion effects
- Anterior Corticospinal Tract - origin, course, bilateral function
- Rubrospinal Tract - red nucleus origin, midbrain decussation, cervical termination
- Vestibulospinal Tracts - both lateral (LVST) and medial (MVST) subdivisions
- Reticulospinal Tracts - pontine vs. medullary, excitatory vs. inhibitory effects
- Tectospinal Tract - superior colliculus origin, orienting reflex
- Corticobulbar Tract - brainstem motor control
- UMN syndrome flowchart - spasticity mechanism explained
- Lesion localization - internal capsule, brainstem, spinal cord patterns
- Summary tables from Gray's Anatomy for Students (eTables 9.5 and 9.6)
- Multiple diagrams from Guyton & Hall and Neuroscience: Exploring the Brain
This is a shared conversation. Sign in to Orris to start your own chat.