Hypersensitivity Reactions * Classification * Mechanism * Mediators * Examples 10 Marks university long answer for advance pharmacology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile this into a thorough, exam-quality answer.
Hypersensitivity Reactions
Advanced Pharmacology - University Long Answer (10 Marks)
Introduction
Hypersensitivity reactions are exaggerated or inappropriate immune responses to antigens (allergens, drugs, microbes, or self-antigens) that result in tissue damage and disease. The term was coined to describe situations where the same immune mechanisms that normally protect the host instead cause harm. In 1963, British pathologists P.G.H. Gell and R.R.A. Coombs classified these reactions into four types (Types I-IV) based on the effector mechanisms involved - a classification system still widely used today.
The effectors for Types I, II, and III hypersensitivity are antibody molecules; Type IV is mediated by antigen-specific effector T cells.
- Goldman-Cecil Medicine, Table 36-1
Classification (Gell and Coombs)
| Type | Name | Mediator | Onset |
|---|---|---|---|
| I | Immediate / Anaphylactic | IgE | Minutes |
| II | Cytotoxic / Cytolytic | IgG, IgM | Hours |
| III | Immune Complex (Arthus) | IgG complexes | 6-12 hrs |
| IV | Delayed-type / Cell-mediated | T lymphocytes | 24-72 hrs |
A Type V (stimulatory) and innate hypersensitivity have been proposed as additions to the original Gell-Coombs classification.
- Roitt's Essential Immunology, 13th Ed.
TYPE I - Immediate (Anaphylactic) Hypersensitivity
Mechanism
Type I is mediated by IgE antibodies and occurs in two phases:
Phase 1 - Sensitization:
- First exposure to the allergen stimulates B cells to produce IgE antibodies (via Th2 cells and IL-4, IL-13).
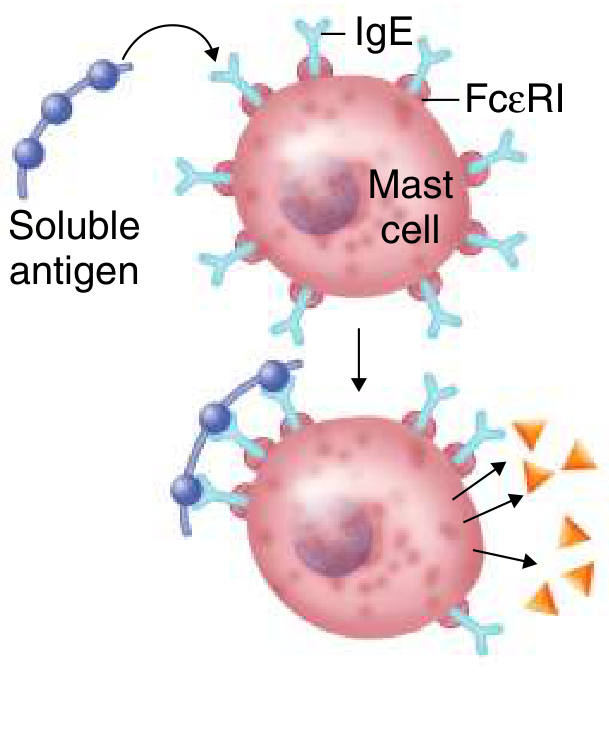
- IgE binds via its Fc portion to FcεRI receptors on mast cells and basophils - these cells become "sensitized."
Phase 2 - Elicitation (Re-exposure):
3. On re-exposure, the allergen cross-links two or more IgE molecules on the mast cell surface.
4. This cross-linking triggers mast cell degranulation - release of preformed mediators from granules.
5. A late-phase response follows (2-24 hours later), driven by eosinophils, basophils, and Th2 lymphocytes.
Mediators of Type I
Preformed (granule-stored) mediators - released immediately:
- Histamine - vasodilation, increased vascular permeability, smooth muscle contraction, increased mucus secretion
- Proteolytic enzymes (tryptase, chymase, carboxypeptidase)
- Heparin - anticoagulant
Newly synthesized mediators (generated after activation):
- Leukotrienes (LTC4, LTD4, LTE4) - potent bronchospasm (1000x more potent than histamine), increased vascular permeability
- Prostaglandins (PGD2) - bronchoconstriction, vasodilation
- Platelet-Activating Factor (PAF) - platelet aggregation, bronchoconstriction
- Cytokines: IL-4, IL-5 (eosinophil activation), IL-13, TNF-α, GM-CSF
- Chemokines: IL-8 (neutrophil recruitment)
- Major basic protein (from eosinophils) - toxic granular protein causing epithelial damage
Clinical Examples
- Systemic anaphylaxis (bee sting, penicillin, peanuts)
- Bronchial asthma (inhaled allergens causing bronchoconstriction)
- Allergic rhinitis / hay fever (pollen)
- Urticaria and angioedema (food, drugs)
- Atopic dermatitis / eczema
- Food allergies (GI tract: diarrhea, vomiting)
"The main targets of this type of reaction are the GI tract (food allergies), the skin (urticaria and atopic dermatitis), the respiratory system (rhinitis and asthma), and the vasculature (anaphylactic shock)."
- Goodman & Gilman's The Pharmacological Basis of Therapeutics
TYPE II - Cytotoxic (Cytolytic) Hypersensitivity
Mechanism
- An antigen is present on a cell surface (either naturally, or a drug hapten bound to a cell surface).
- IgG or IgM antibodies are produced against these cell-surface or matrix-associated antigens.
- Antibody binding triggers cell destruction via three mechanisms:
- Complement activation (classical pathway) → membrane attack complex (MAC) → cell lysis
- Opsonization and phagocytosis - C3b and IgG coat the cell; FcγR+ macrophages phagocytose it
- Antibody-Dependent Cell-mediated Cytotoxicity (ADCC) - NK cells with FcγRIII (CD16) kill antibody-coated targets
- Target cells are mainly in the circulatory system (RBCs, platelets, WBCs).
Mediators
- IgG / IgM antibodies
- Complement proteins (C1q, C3b, C5-C9 - MAC)
- FcγR-bearing cells: macrophages, NK cells
Clinical Examples
- Penicillin-induced hemolytic anemia - penicillin binds RBC surface as a hapten → IgG forms → complement-mediated lysis
- Quinidine-induced thrombocytopenic purpura
- Sulfonamide-induced granulocytopenia
- Rh incompatibility - Rh-negative mother develops anti-Rh IgG against Rh-positive fetal RBCs
- ABO transfusion reactions - preformed IgM antibodies lyse incompatible donor RBCs
- Autoimmune hemolytic anemia
- Myasthenia gravis (antibodies to acetylcholine receptors - blocking subtype)
- Goodpasture's syndrome (anti-GBM antibodies)
"Type II allergies are mediated by both IgG and IgM antibodies and usually are attributed to their capacity to activate the complement system."
- Goodman & Gilman's
TYPE III - Immune Complex (Arthus) Hypersensitivity
Mechanism
- Soluble antigen-antibody (IgG) immune complexes are formed in circulation.
- Under normal conditions, complexes are cleared; in Type III, excessive complexes overwhelm the clearance system.
- Complexes are deposited in vascular endothelium (kidneys, joints, skin, blood vessels).
- Deposited complexes activate complement → C3a and C5a (anaphylatoxins) are generated.
- C5a acts as a chemoattractant for neutrophils (PMNs) to the site.
- Neutrophils attempt phagocytosis of complexes but release lysosomal enzymes (proteases, collagenase) and reactive oxygen species into the surrounding tissue, causing inflammation and damage.
- Platelet aggregation and mast cell activation also contribute.
Mediators
- IgG immune complexes
- Complement fragments (C3a, C5a - anaphylatoxins)
- Neutrophil lysosomal enzymes (proteases, collagenase)
- Reactive oxygen species
Clinical Examples
- Serum sickness (e.g., antiserum administration, some drugs) - urticaria, arthralgia, lymphadenopathy, fever; lasts 6-12 days
- Arthus reaction - local immune complex deposition after repeated intradermal injections of antigen
- Subacute bacterial endocarditis - circulating bacterial antigen-antibody complexes deposit in kidneys, joints
- Post-streptococcal glomerulonephritis
- Systemic lupus erythematosus (SLE) - widespread immune complex deposition in kidneys, skin, joints
- Rheumatoid arthritis (partially)
- Hypersensitivity pneumonitis (Farmer's lung, pigeon fancier's lung)
"Type III allergic reactions are mediated predominantly by IgG; the mechanism involves generation of antigen-antibody complexes that subsequently fix complement. The complexes are deposited in the vascular endothelium, where a destructive inflammatory response called serum sickness occurs."
- Goodman & Gilman's
TYPE IV - Delayed-type (Cell-mediated) Hypersensitivity
Mechanism
Type IV is unique - it is NOT antibody-mediated but rather mediated by sensitized T lymphocytes. Onset is characteristically delayed (24-72 hours).
Phase 1 - Sensitization:
- Antigen is processed and presented on MHC class II by antigen-presenting cells (APCs) to CD4+ T cells (or MHC class I to CD8+ T cells).
- T cells become sensitized and expand into memory T cells.
Phase 2 - Elicitation (Re-exposure):
3. On re-exposure, antigen-specific CD4+ Th1 cells are activated.
4. Th1 cells release lymphokines (cytokines): chiefly IFN-γ, TNF-β (lymphotoxin), IL-2, IL-3.
5. IFN-γ activates macrophages to release further inflammatory mediators.
6. Recruitment of neutrophils and macrophages creates a delayed granulomatous inflammatory response.
CD8+ CTL subtype: Cell-associated antigens (virus-infected cells, transplanted tissue) are recognized directly, and cytotoxic CD8+ T cells perform direct cytotoxicity (perforin-granzyme pathway).
Roitt's classification of Type IV subtypes:
- Th1-mediated - contact dermatitis, tuberculin reaction (macrophage activation)
- Th2-mediated - chronic allergic inflammation (eosinophil activation)
- Th17-mediated - contact/atopic dermatitis, rheumatoid arthritis (neutrophil/macrophage activation)
- CTL-mediated - direct cytotoxicity (virus-infected cells, graft rejection)
Mediators
- IFN-γ - activates macrophages
- TNF-α / TNF-β (lymphotoxin) - inflammatory; recruits leukocytes
- IL-2 - T cell proliferation
- IL-17 (Th17) - neutrophil recruitment
- Perforin / Granzyme B (CTLs) - direct cell killing
- Activated macrophages release: IL-1, IL-6, reactive oxygen species, lysosomal enzymes
Clinical Examples
- Allergic contact dermatitis - poison ivy/oak (urushiol), nickel, latex
- Tuberculin reaction (Mantoux test) - PPD injection → indurated reaction at 48-72 hours
- Granulomatous hypersensitivity - tuberculosis, sarcoidosis, leprosy (Hansen's disease), schistosomiasis
- Graft rejection (organ/skin transplant)
- Type 1 diabetes mellitus - CD8+ CTLs destroy pancreatic beta cells
- Multiple sclerosis - Th1/Th17 attack on myelin
"These reactions are mediated by sensitized T lymphocytes and macrophages. When sensitized cells come in contact with an antigen, an inflammatory reaction is generated by the production of lymphokines and the subsequent influx of neutrophils and macrophages."
- Goodman & Gilman's
TYPE V - Stimulatory Hypersensitivity (Addition to Gell-Coombs)
A fifth type has been added by some authorities (notably Roitt's) in which antibodies act as agonists for cell surface receptors rather than destroying cells:
- Graves' disease - anti-TSH receptor antibodies stimulate thyroid overactivity (hyperthyroidism)
- Neonatal Graves' disease - maternal IgG crosses placenta
Summary Comparison Table
| Feature | Type I | Type II | Type III | Type IV |
|---|---|---|---|---|
| Mediator | IgE | IgG, IgM | IgG complexes | T cells |
| Complement | No | Yes | Yes | No |
| Onset | Seconds-minutes | Hours | 6-12 hrs | 24-72 hrs |
| Antigen | Soluble, environmental | Cell surface/matrix | Soluble (circulating) | Cell-associated/soluble |
| Effector | Mast cells, basophils | Complement, NK, Mφ | PMNs, Mφ | Th1/Th17 cells, CTLs |
| Transfer | Serum (IgE) | Serum (IgG) | Serum (complexes) | Cells (not serum) |
| Key mediators | Histamine, leukotrienes, prostaglandins | Complement (MAC), C3b | C3a, C5a, lysosomal enzymes | IFN-γ, TNF-α, IL-2, perforin |
| Drug examples | Penicillin anaphylaxis | Penicillin hemolytic anemia | Serum sickness (antibiotics) | Contact dermatitis (nickel) |
Pharmacological Relevance
- Antihistamines (H1-blockers) - target histamine in Type I (urticaria, allergic rhinitis)
- Epinephrine - first-line for Type I anaphylaxis; reverses bronchoconstriction and vasodilation via β2 and α1 receptors
- Corticosteroids - suppress inflammation in all types; particularly Type IV
- Leukotriene receptor antagonists (Montelukast) - block CysLT1 receptors, used in asthma (Type I late phase)
- Anti-IgE (Omalizumab) - binds free IgE, prevents FcεRI binding; approved for severe asthma/urticaria (Type I)
- Immunosuppressants (Cyclosporine, Tacrolimus) - suppress T cell activation, used in Type IV graft rejection
- NSAIDs - block prostaglandin synthesis (Type I mediators)
- Corticosteroids in serum sickness (Type III) - reduce immune complex-mediated inflammation
Conclusion
Hypersensitivity reactions represent a spectrum of immune-mediated tissue injury. Types I-III are antibody-mediated while Type IV is cell-mediated. Understanding the specific effector mechanism of each type is essential for:
- Identifying the etiology of adverse drug reactions
- Selecting appropriate pharmacological interventions (antihistamines, steroids, epinephrine, biologics)
- Predicting cross-reactivity patterns in drug hypersensitivity
The Gell-Coombs classification, though developed in 1963, remains the standard framework in both clinical practice and pharmacology examinations.
References:
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, Chapter 9
- Goldman-Cecil Medicine (International Edition), Chapter 36
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Ed.
- Janeway's Immunobiology, 10th Ed., Chapter 14
- Roitt's Essential Immunology, 13th Ed., Chapter 14
This is a shared conversation. Sign in to Orris to start your own chat.