
IMG-20260511-WA0009(1).jpg
Explain the ECG and diagnostic it with full Explain each and every thing
Reading File
Finding Sources
Finding Sources
Searching the Web
ECG interpretation systematic approach ST elevation LBBB ventricular hypertrophy 2024
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Now I have enough information to provide a comprehensive ECG analysis. Let me synthesize everything from the visual assessment of the ECG image and the textbook knowledge.
📋 Complete ECG Analysis & Diagnostic Report
Technical Details (from strip label): Rhythm Strip Lead II | Paper speed: 25 mm/sec | 1 cm/mV gain
STEP 1 — ECG Overview & Systematic Approach
Using Harrison's 14-parameter systematic approach, here is a full read of this 12-lead ECG:
STEP 2 — Rhythm
Lead II rhythm strip (bottom):
- Regular R-R intervals
- P waves are visible before each QRS → Normal sinus rhythm
- Rate approximately 60–75 bpm (regular intervals spanning roughly 4–5 large boxes)
STEP 3 — Heart Rate
- Each large box = 0.2 sec at 25 mm/sec
- R-R interval ≈ 4–5 large boxes → Rate ≈ 60–75 bpm → Normal
STEP 4 — PR Interval
- PR interval measured in Lead II ≈ 3–4 small boxes = 0.12–0.16 sec
- Normal (normal: 0.12–0.20 sec)
- No evidence of first, second, or third-degree AV block
STEP 5 — QRS Duration & Morphology
This is the most critical finding:
Looking at the precordial leads (V1–V6) and limb leads:
| Lead | Morphology | Significance |
|---|---|---|
| V1 | Broad, notched, rS or QS pattern | Consistent with LBBB |
| V2 | Broad QS complex | Consistent with LBBB |
| V3 | Broad, slow transition | LBBB pattern |
| V4 | Broad positive deflection | LBBB |
| V5 | Broad monophasic R or notched R | Classic LBBB lateral pattern |
| V6 | Broad monophasic R | Classic LBBB lateral pattern |
| I | Broad monophasic R (upright) | LBBB |
| aVL | Broad positive R | LBBB |
| II | Small/notched complex | LBBB |
| III | Small negative or QS | LBBB |
| aVF | Small or negative | LBBB |
QRS duration appears ≥ 120 ms (≥ 3 small boxes) → Complete Left Bundle Branch Block (LBBB)
Per Harrison's: "Left bundle branch block alters both early and later phases of ventricular depolarization. The major QRS vector is directed to the left and posteriorly... septal depolarization proceeds from right to left"
STEP 6 — ST Segments
This is where LBBB makes interpretation challenging. In LBBB, discordant ST changes are expected (ST goes opposite to the QRS).
| Lead | Finding | Interpretation |
|---|---|---|
| V1–V3 | ST elevation (discordant to negative QRS) | Expected in LBBB — normal discordance |
| V4–V6 | ST depression or flat (discordant to positive QRS) | Expected in LBBB |
| I, aVL | Subtle ST changes | Expected in LBBB |
| II, III, aVF | Isoelectric or mild changes |
Key assessment: The ST changes appear appropriate/discordant for LBBB — no concordant ST elevation is visible, which would be the hallmark of Sgarbossa criteria for AMI on top of LBBB.
STEP 7 — T Waves
In LBBB, T waves are normally opposite in polarity to the QRS (secondary repolarization changes):
- V1–V3: T waves upright (with negative QRS) → Expected
- V4–V6: T waves inverted (with positive QRS) → Expected
- No primary T-wave changes suggesting additional ischemia
STEP 8 — QT Interval
- QT interval is prolonged relative to baseline due to LBBB (wide QRS contributes to wide QT)
- Corrected QT (QTc) cannot be reliably calculated in the presence of LBBB
STEP 9 — P Waves
- P waves visible before each QRS in lead II
- Morphology: No notching or biphasic pattern suggesting atrial enlargement
- Normal P waves
STEP 10 — Axis
- Lead I: Upright QRS → Left-facing
- Lead II: Small/negative
- aVF: Negative or small
→ Left axis deviation (LAD), approximately –30° to –60°
- This is expected in LBBB (vector directed leftward and posteriorly)
STEP 11 — Voltages / Ventricular Hypertrophy
- The broad, tall R waves in V5–V6, I, aVL raise the question of underlying Left Ventricular Hypertrophy (LVH)
- Per Harrison's: "Multiple voltage criteria for LVH have been proposed based on tall left precordial R waves and deep right precordial S waves (SV₁ + RV₅ or RV₆ > 35 mm)"
- LVH often progresses to incomplete or complete LBBB — this pattern is consistent
- LBBB itself makes independent LVH voltage criteria unreliable
STEP 12 — R-Wave Progression
- Right precordial leads (V1–V3): Small or absent R waves → Poor R-wave progression
- In LBBB this is expected because septal depolarization is reversed
STEP 13 — Abnormal Q Waves
- No pathological Q waves visible in inferior or lateral leads that are not explained by LBBB
- LBBB eliminates the normal septal Q waves in I, V5, V6
🔴 PRIMARY DIAGNOSIS
Complete Left Bundle Branch Block (LBBB)
New or Old — this is the critical clinical question
🩺 FULL DIAGNOSTIC Interpretation
Main Findings:
- Sinus rhythm — ~60–75 bpm
- Normal PR interval — AV conduction intact
- Complete LBBB — QRS ≥ 120 ms, broad monophasic R in I/V5/V6, rS or QS in V1
- Left axis deviation — secondary to LBBB
- Discordant ST-T changes — secondary (expected) in LBBB
- Possible underlying LVH — suggested by high lateral voltages, consistent with LBBB etiology
⚠️ Is This an STEMI Equivalent?
Apply the Sgarbossa Criteria to rule out acute MI:
| Criterion | Score | This ECG |
|---|---|---|
| Concordant ST elevation ≥ 1 mm (any lead where QRS is positive) | 5 pts | Not clearly seen |
| Concordant ST depression ≥ 1 mm in V1–V3 | 3 pts | Not clearly seen |
| Excessively discordant ST elevation ≥ 5 mm | 2 pts | Need clinical correlation |
Score < 3 = low probability of AMI — however, new LBBB in a symptomatic patient must be treated as STEMI-equivalent until proven otherwise.
Differential Diagnosis for LBBB
| Cause | Clinical Clue |
|---|---|
| Hypertensive heart disease / LVH | Most common — chronic hypertension |
| Ischemic cardiomyopathy | Coronary artery disease, prior MI |
| Dilated cardiomyopathy | Reduced EF, cardiac enlargement |
| Aortic valve disease | Murmur, exertional symptoms |
| Cardiomyopathy (any cause) | Heart failure symptoms |
| Acute anterior MI | New LBBB + chest pain = emergency |
| Rate-related (intermittent) | LBBB only at faster heart rates |
📌 Clinical Action Points
| Priority | Action |
|---|---|
| Urgent | Compare with prior ECGs — is this new LBBB? |
| Urgent | If new LBBB + chest pain/dyspnea → activate cath lab (STEMI protocol) |
| Urgent | Troponin I/T serial measurements (0h, 2h, 6h) |
| Important | Echocardiography — assess LV function, wall motion, LVH |
| Important | BP measurement — rule out hypertensive heart disease |
| Routine | Thyroid function, metabolic panel, BNP/NT-proBNP |
| Routine | Holter monitor if intermittent symptoms |
Summary Table
| Parameter | Finding | Normal? |
|---|---|---|
| Rhythm | Sinus | ✅ |
| Rate | ~60–75 bpm | ✅ |
| PR interval | 0.12–0.16 sec | ✅ |
| QRS duration | ≥ 120 ms | ❌ Prolonged |
| QRS morphology | LBBB pattern | ❌ Abnormal |
| Axis | Left axis deviation | ❌ |
| ST segments | Discordant changes | Secondary to LBBB |
| T waves | Discordant | Secondary to LBBB |
| R-wave progression | Poor (V1–V3) | Expected in LBBB |
| Voltages | Possibly elevated (LVH) | Borderline |
| P waves | Normal | ✅ |
| Q waves | None pathological | ✅ |
References:
- Harrison's Principles of Internal Medicine, 22nd Ed. — ECG Interpretation (Chapter 247)
- Tintinalli's Emergency Medicine — STEMI ECG Criteria, Table 49-4
- Sgarbossa EB et al. Electrocardiographic diagnosis of MI in LBBB. NEJM 1996
⚠️ Clinical Disclaimer: ECG interpretation must always be correlated with the patient's clinical presentation, symptoms, history, and serial troponins. A new LBBB in a symptomatic patient is a medical emergency until ruled out.
How is hyperactive myocardial infraction is screen in ecg
Reading File
Finding Sources
Finding Sources
Searching the Web
hyperacute myocardial infarction ECG changes T waves STEMI earliest signs screening
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Now I have everything needed. Here is the full comprehensive answer.
🫀 Hyperacute Myocardial Infarction — ECG Screening & Full Explanation
The correct term is "Hyperacute" MI — referring to the very first minutes to hours of a complete coronary artery occlusion, before classic STEMI changes fully develop. This is the most time-critical window for intervention.
🔬 What Is "Hyperacute" Phase MI?
When a coronary artery suddenly occludes, the myocardium goes through a predictable electrical evolution on ECG. The hyperacute phase is Phase 1 — it lasts only minutes to ~30 minutes and is frequently missed because it can look nearly normal.
Per Harrison's Principles of Internal Medicine (22nd Ed):
"When the acute ischemia is transmural, the ST vector usually is shifted in the direction of the outer (epicardial) layers, producing ST elevations and sometimes, in the earliest stages of ischemia, tall, positive so-called hyperacute T waves over the ischemic zone."
⏱️ The 4 Stages of MI Evolution on ECG
| Stage | Time Frame | ECG Finding | What's Happening |
|---|---|---|---|
| 1. Hyperacute | 0–30 min | Tall, broad, peaked T waves | Acute ischemia → ionic shifts → T-wave inflation |
| 2. Acute (Injury) | 30 min – hours | ST elevation (STEMI pattern) | Epicardial injury current develops |
| 3. Established | Hours – days | Q waves + T-wave inversion | Myocyte necrosis → loss of depolarization forces |
| 4. Chronic/Old | Days – weeks+ | Persistent Q waves ± ST resolution | Scar formation |
🏆 Stage 1 — HYPERACUTE T WAVES (Key Finding to Screen For)
What They Look Like:
| Feature | Normal T Wave | Hyperacute T Wave |
|---|---|---|
| Height | ≤ 6 mm limb leads, ≤ 10 mm precordial | Abnormally tall, disproportionate to QRS |
| Shape | Asymmetric (slow rise, fast descent) | Broad-based, symmetric, fat/inflated |
| Base | Narrow | Wide base |
| Context | No symptoms | Chest pain, diaphoresis |
Real ECG Example from Rosen's Emergency Medicine:
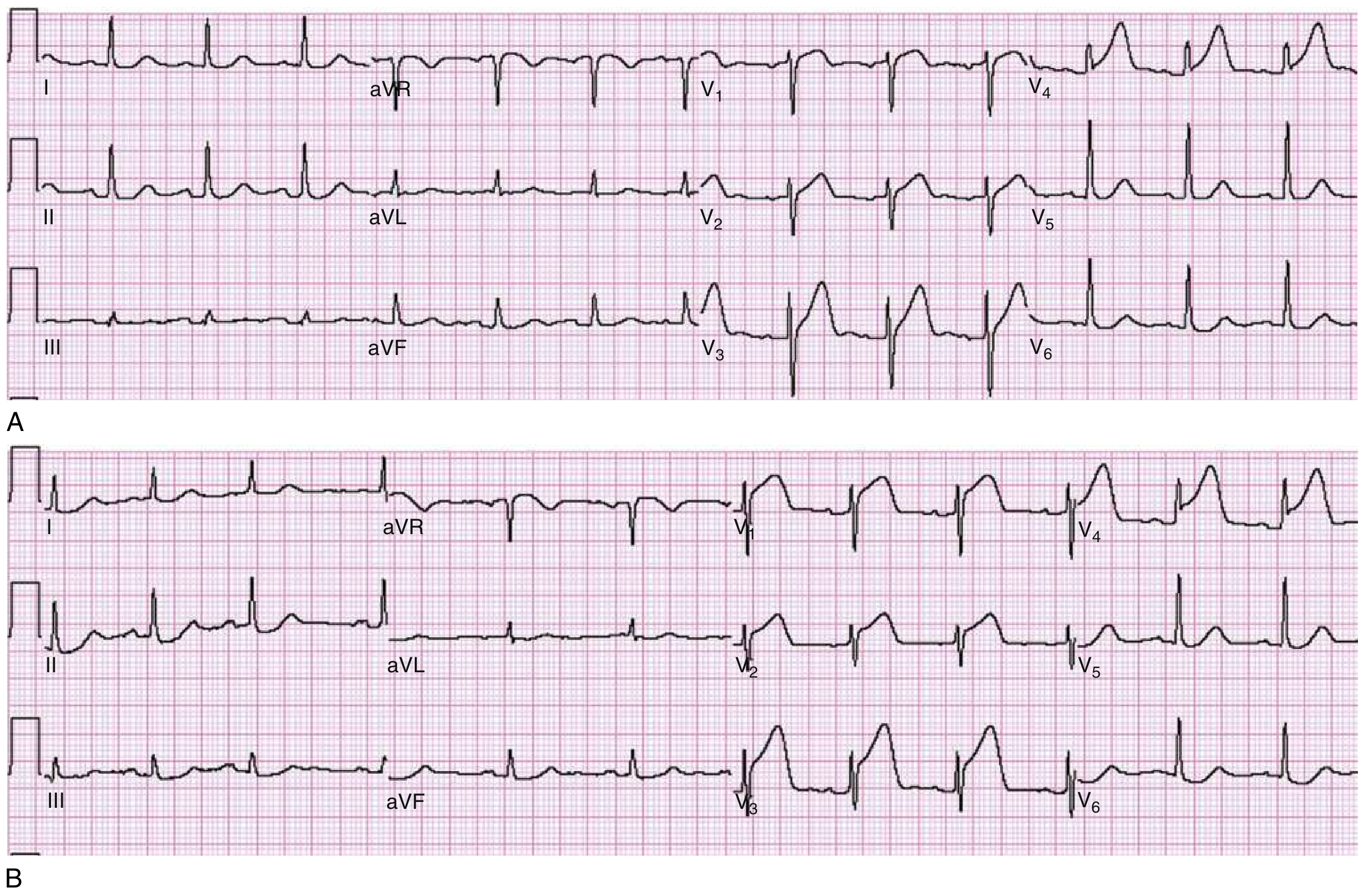
(A) — Broad, tall T waves in V3 and V4 — this is the hyperacute phase. ST is just beginning to rise in V3/V4; V1 and V2 are suspicious.
(B) — Same patient, only 30 minutes later — now shows prominent ST elevation in V1–V4. Full STEMI has evolved.
This is why serial ECGs every 15–30 minutes are mandatory in high-suspicion chest pain — the hyperacute phase can be missed on a single ECG.
🩺 How to SCREEN for Hyperacute MI on ECG — Step by Step
Step 1: Look at T-Wave Proportionality
The best trick: Compare T-wave height to QRS amplitude in the same lead
- Hyperacute T waves are taller than the R wave they follow, or at minimum strikingly disproportionate
- In anterior MI: check V2, V3, V4
- In inferior MI: check II, III, aVF
Step 2: Assess T-Wave Shape
- Hyperacute T waves are symmetric and broad-based
- Normal T waves are asymmetric (slow upstroke, steep downstroke)
- A "fat," "inflated," or "balloon-like" T wave = hyperacute until proven otherwise
Step 3: Look for Early ST Changes
Even subtle ST changes alongside tall T waves are significant:
- Straightening of the ST segment (loss of concavity before frank elevation)
- J-point elevation — even 0.5 mm elevation in the right leads matters
- The ST may still appear borderline while T waves are already hyperacute
Step 4: Check for Reciprocal Changes
A key screening tool:
- Inferior hyperacute MI (RCA/LCx occlusion): hyperacute T waves in II, III, aVF + reciprocal T-wave flattening/inversion in aVL
- Anterior MI (LAD occlusion): tall T in V1–V4 + possible ST depression in inferior leads
Reciprocal changes increase specificity dramatically.
Step 5: ST/T Ratio (New Concept)
The ACC/AHA now formally endorses hyperacute T waves as a "STEMI equivalent" based on the ratio:
T-wave amplitude / R-wave amplitude > 1 in the same lead = highly suspicious for occlusion MI
🧭 ECG Localisation: Where to Look
| Artery Occluded | Leads to Watch for Hyperacute T Waves |
|---|---|
| LAD (Left Anterior Descending) | V1, V2, V3, V4 (anterior) |
| RCA (Right Coronary Artery) | II, III, aVF (inferior) |
| LCx (Left Circumflex) | I, aVL, V5, V6 (lateral) ± inferior |
| Posterior MI | Tall R waves + upright T in V1–V2 (reciprocal to posterior ST elevation) |
⚡ The Current-of-Injury Mechanism (Why It Happens)

Per Harrison's:
"Severe, acute ischemia lowers the resting membrane potential and shortens the duration of the action potential. Such changes cause a voltage gradient between normal and ischemic zones. These currents of injury are represented on the surface ECG by deviation of the ST segment."
- Subendocardial ischemia (NSTEMI): ST vector points inward → ST depression in overlying leads
- Transmural ischemia (STEMI/hyperacute): ST vector points outward → ST elevation + hyperacute T in overlying leads
⚠️ Stage 3 — Q Waves (Established Infarction)
Per Harrison's:
"Necrosis of sufficient myocardial tissue may lead to decreased R-wave amplitude or abnormal Q waves in the anterior or inferior leads. Abnormal Q waves were once considered markers of transmural infarction..."
Pathological Q wave criteria:
- Duration ≥ 0.04 sec (1 small box)
- Depth ≥ 25% of the R wave in the same lead
- Present in at least 2 contiguous leads
❌ Mimics to Exclude (False Positives)
Per Harrison's, the following can mimic hyperacute T waves and must be excluded:
| Mimic | Distinguishing Feature |
|---|---|
| Benign early repolarization | Concave ST elevation, notching at J-point, no symptoms, no evolution |
| Hyperkalemia | Peaked but narrow/tent-shaped T waves, wide QRS, sine wave pattern |
| LVH / LBBB | Expected in those leads, no dynamic change |
| Pericarditis | Diffuse ST elevation (saddle-shaped), PR depression, all leads |
| Cerebrovascular injury | Diffuse deep T inversions, prolonged QT |
🚨 Clinical Screening Protocol (What to Do)
Chest pain patient arrives
↓
ECG within 10 minutes
↓
Look for: hyperacute T waves (tall, broad, symmetric)
↓
Borderline? → Serial ECG every 15–30 min
↓
Dynamic change confirmed?
↓
ACTIVATE CATH LAB — don't wait for full STEMI criteria
↓
Troponin + Serial Troponin (0h, 1h, 2h, 6h)
📋 Quick Reference Summary
| ECG Feature | Hyperacute MI | Normal |
|---|---|---|
| T-wave height | Abnormally tall, > R wave | Proportionate |
| T-wave shape | Broad-based, symmetric | Asymmetric |
| ST segment | Straightening or early elevation | Flat/concave |
| Reciprocal changes | Present in opposite leads | Absent |
| Evolution | Changes on serial ECG | Stable |
| Symptoms | Chest pain, diaphoresis | Asymptomatic |
References:
- Harrison's Principles of Internal Medicine, 22nd Ed. — Chapter 247, Myocardial Ischemia and Infarction
- Rosen's Emergency Medicine — Chapter 64, Electrocardiographic Abnormalities in Acute Coronary Syndromes (Fig. 64.1)
- ACC/AHA Guidelines — Hyperacute T waves as STEMI equivalent (2022)
Key takeaway: Hyperacute MI is screened by recognizing disproportionately tall, broad, symmetric T waves in ≥2 contiguous leads, often with early ST straightening and reciprocal changes — before frank ST elevation appears. Serial ECGs are essential because this phase lasts only minutes to 30 minutes.
This is a shared conversation. Sign in to Orris to start your own chat.