Anatomy of shoulder
Reading File
Finding Sources
Searching the Web
shoulder joint anatomy overview glenohumeral rotator cuff
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Excellent images retrieved. Now I have everything needed for a comprehensive answer.
Anatomy of the Shoulder
The shoulder is the most mobile joint in the body. Its mobility comes at the cost of stability, which is why it is also the most commonly dislocated joint. The "shoulder" is not one joint but a complex of four distinct joints working together.
1. Bones of the Shoulder Girdle
Three bones form the shoulder:
- Clavicle - the only bony connection between the upper limb and the axial skeleton
- Scapula - a flat, triangular bone with key landmarks:
- Glenoid cavity (fossa) - shallow, oval depression that articulates with the humeral head
- Acromion - projects superolaterally, forms roof of the shoulder
- Coracoid process - projects anteriorly, serves as attachment for muscles and ligaments
- Spine of scapula - prominent ridge on the posterior surface
- Scapular notch - transmits the suprascapular nerve (artery passes above the ligament)
- Humerus - the proximal end has:
- Head - articulates with the glenoid (4:1 surface area ratio - head is much larger)
- Anatomical neck
- Surgical neck - common fracture site; the axillary nerve runs here
- Greater tubercle - insertion of supraspinatus, infraspinatus, teres minor
- Lesser tubercle - insertion of subscapularis
- Intertubercular (bicipital) groove - lodges the long head of biceps tendon
2. The Four Joints of the Shoulder Complex
| Joint | Type | Articulation |
|---|---|---|
| Glenohumeral | Ball-and-socket synovial | Head of humerus + glenoid fossa of scapula |
| Acromioclavicular (AC) | Plane synovial | Acromion + lateral end of clavicle |
| Sternoclavicular (SC) | Saddle synovial | Manubrium sterni + medial end of clavicle |
| Scapulothoracic | Physiological (not a true synovial joint) | Scapula glides on serratus anterior / rib cage |
The SC joint is the only true bony articulation between the upper limb and the axial skeleton.
3. The Glenohumeral Joint - Key Features
Glenoid Labrum
A fibrocartilaginous rim that deepens the shallow glenoid cavity, increasing contact area and stability. It also serves as the attachment for the glenohumeral ligaments and the long head of biceps tendon (at the supraglenoid tubercle).
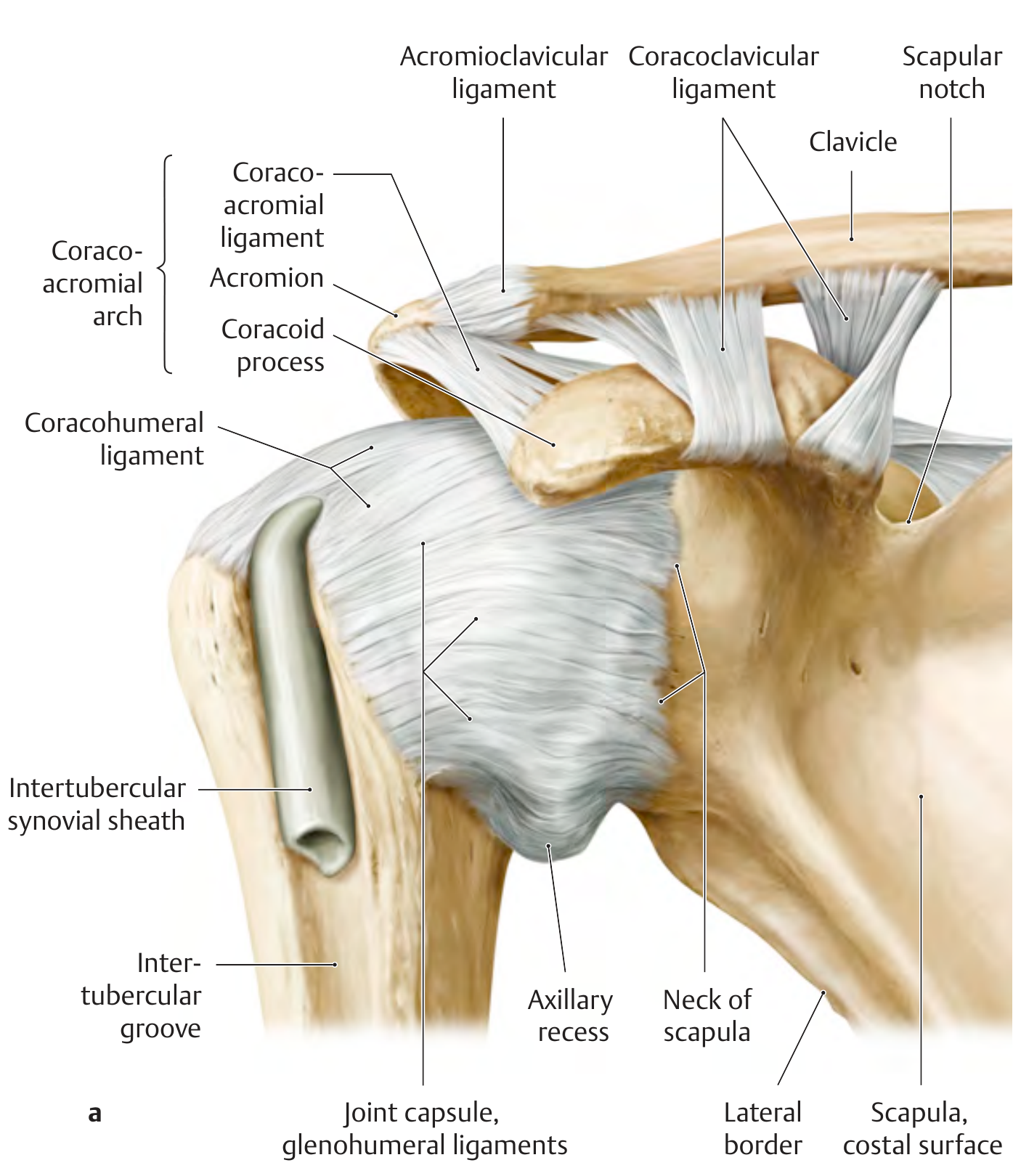
Joint Capsule
- Fibrous sheath attaching from the anatomical neck of the humerus to the rim of the glenoid fossa
- Very loose and redundant - the axillary recess forms inferiorly when the arm hangs at rest; this allows full abduction range of motion
- The capsule is thin and unprotected posteriorly (no ligament reinforcement)
- The subtendinous bursa of subscapularis and the subcoracoid bursa communicate with the joint cavity
- The synovial sheath of the long head of biceps also communicates with the joint cavity via the intertubercular groove
4. Ligaments
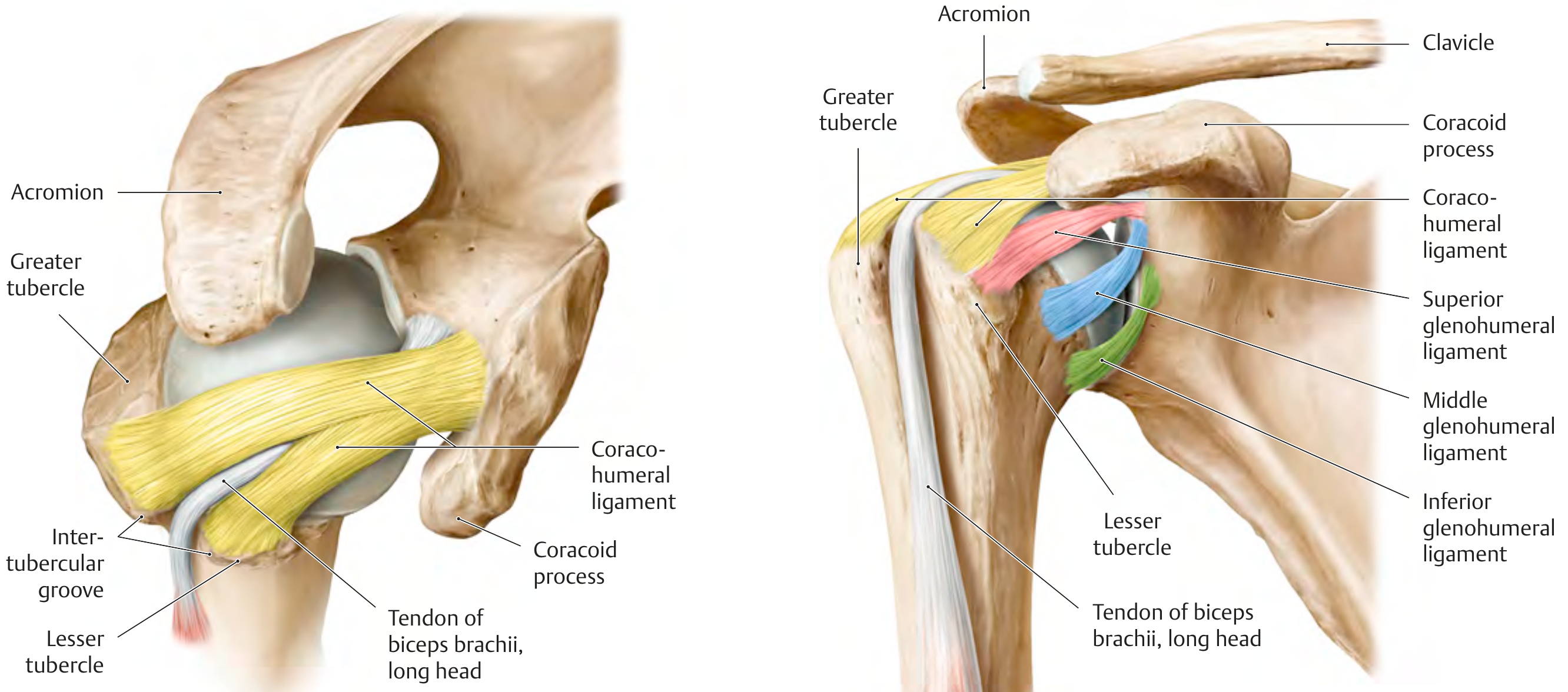
Glenohumeral Ligaments (reinforce the anterior capsule)
Three distinct thickenings of the anterior joint capsule:
- Superior glenohumeral ligament (SGHL) - prevents inferior subluxation when arm is adducted
- Middle glenohumeral ligament (MGHL) - limits external rotation and anterior translation
- Inferior glenohumeral ligament (IGHL) - the most important stabilizer; its anterior band is the primary restraint against anterior dislocation when the arm is abducted and externally rotated (the "AMBRI/TUBS position")
Coracohumeral Ligament
- Arises from the base of the coracoid process; splits into two bands attaching to the greater and lesser tubercles
- Reinforces the superior capsule; stabilizes the long head of biceps tendon in the rotator interval
Coracoacromial Ligament
- Spans from coracoid process to the undersurface of the acromion
- Together with the acromion and coracoid, forms the coracoacromial arch - a rigid roof over the rotator cuff that protects the humeral head superiorly but is also the site of rotator cuff impingement
Coracoclavicular Ligament
- Connects the clavicle to the coracoid process (two parts: conoid and trapezoid)
- Critical for AC joint stability; rupture = grade III AC separation (Rockwood III)
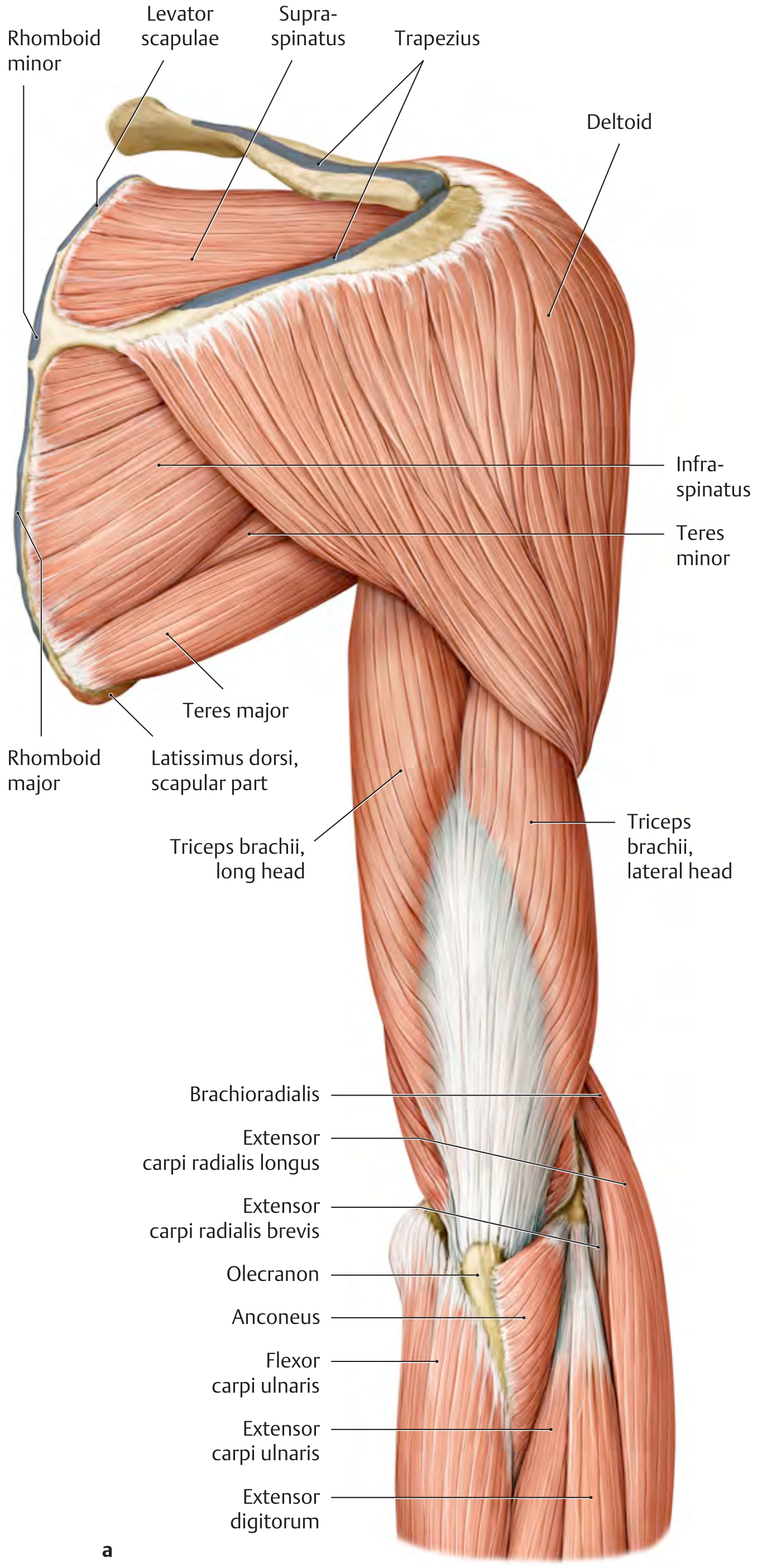
5. Rotator Cuff (SITS Muscles)
The four rotator cuff muscles form a musculotendinous sleeve around the humeral head, providing dynamic stability and controlling movement.
| Muscle | Origin | Insertion | Nerve | Action |
|---|---|---|---|---|
| Supraspinatus | Supraspinous fossa | Greater tubercle (superior facet) | Suprascapular (C5-C6) | Initiates abduction (first 15°), stabilizes humeral head |
| Infraspinatus | Infraspinous fossa | Greater tubercle (middle facet) | Suprascapular (C5-C6) | External rotation, posterior stability |
| Teres minor | Lateral border of scapula | Greater tubercle (inferior facet) | Axillary (C5-C6) | External rotation, adduction |
| Subscapularis | Subscapular fossa (anterior scapula) | Lesser tubercle | Upper + lower subscapular (C5-C7) | Internal rotation, anterior stability |
The supraspinatus passes under the coracoacromial arch and is the most commonly torn rotator cuff tendon (especially at its "critical zone" - a relatively avascular area near its insertion).
6. Other Muscles Acting on the Shoulder
Deltoid - the most powerful abductor; three parts (anterior, middle, posterior); innervated by the axillary nerve (C5-C6). Runs over the rotator cuff.
Scapular stabilizers (important for proper shoulder mechanics):
- Trapezius (upper, middle, lower) - elevates, retracts, and depresses the scapula
- Serratus anterior - protracts the scapula and holds it against the chest wall; innervated by the long thoracic nerve (C5-C7); injury causes "winged scapula"
- Rhomboids (major and minor) - retract and elevate the scapula; innervated by dorsal scapular nerve
- Levator scapulae - elevates and medially rotates the scapula
Other prime movers:
- Pectoralis major - flexion, adduction, internal rotation
- Latissimus dorsi - extension, adduction, internal rotation
- Teres major - adduction and internal rotation
- Biceps brachii (long head) - assists in shoulder flexion; stabilizes the humeral head by compressing it into the glenoid
7. Bursae
Several bursae reduce friction around the shoulder:
- Subacromial bursa - the largest and most clinically important; lies between the deltoid/acromion and the supraspinatus tendon; inflammation causes subacromial impingement syndrome
- Subdeltoid bursa - often fuses with the subacromial bursa
- Subcoracoid bursa - communicates with the joint cavity
- Subtendinous bursa of subscapularis - communicates with the joint cavity
8. Neurovascular Supply
Nerve Supply
The shoulder is supplied predominantly by branches of the brachial plexus (C5-C6 root values dominant):
- Axillary nerve (C5-C6) - supplies deltoid and teres minor; vulnerable in shoulder dislocation and surgical neck fractures; tested by sensation over the "regimental badge" area (lateral upper arm)
- Suprascapular nerve (C5-C6) - supplies supraspinatus and infraspinatus; can be compressed at the scapular notch
- Subscapular nerves (upper C5-C6, lower C5-C6) - supply subscapularis; lower subscapular also supplies teres major
- Long thoracic nerve (C5-C7) - supplies serratus anterior; injury = winged scapula
Blood Supply
- Anterior and posterior circumflex humeral arteries - branches of the axillary artery; form an anastomotic ring around the surgical neck
- Suprascapular artery - supplies supraspinatus and infraspinatus
- Thoracoacromial artery - supplies the acromioclavicular region
9. Stabilizers - Summary
| Mechanism | Components |
|---|---|
| Static | Bony shape (glenoid concavity, labrum), glenohumeral ligaments, joint capsule, negative intraarticular pressure |
| Dynamic | Rotator cuff (SITS), long head of biceps, periscapular muscles, rotator interval |
The inferior glenohumeral ligament (anterior band) is the single most important static stabilizer, particularly against anterior dislocation in the abducted and externally rotated position.
10. Range of Motion
| Movement | Normal Range |
|---|---|
| Flexion | 0-180° |
| Extension | 0-60° |
| Abduction | 0-180° (glenohumeral: 0-120°; additional 60° from scapulothoracic rotation) |
| Internal rotation | 0-70° |
| External rotation | 0-90° |
| Circumduction | 360° |
The scapulohumeral rhythm is 2:1 - for every 3° of shoulder abduction, 2° occurs at the glenohumeral joint and 1° at the scapulothoracic joint.
Sources: THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System; Miller's Review of Orthopaedics 9th Edition; Imaging Anatomy Text and Atlas Vol. 3
This is a shared conversation. Sign in to Orris to start your own chat.