Now I have everything needed for a thorough, resident-level guide. Here it is:
Approach to Jaundice - MD Medicine Year 1
1. Definition
Jaundice (from French jaune = yellow) is the yellow-orange discoloration of skin, sclera, and mucous membranes caused by elevated plasma bilirubin. It becomes clinically visible when serum bilirubin exceeds 2.5-3 mg/dL (normal: up to 1.2 mg/dL). The sclera is the most sensitive site to detect early jaundice due to its high elastin content, which binds bilirubin avidly. - Goldman-Cecil Medicine
2. Bilirubin Metabolism - The Backbone
Understanding metabolism is non-negotiable. Every cause of jaundice maps to a step in this pathway.
RBC destruction (spleen/RES)
↓
Heme → Biliverdin → Unconjugated bilirubin (UCB)
[Lipid-soluble, albumin-bound, NOT filtered by kidneys]
↓ (transported to liver)
Hepatocyte uptake → Conjugation with glucuronic acid (UGT1A1 enzyme)
→ Conjugated bilirubin (CB) [Water-soluble]
↓
Excreted into bile → Intestine
→ Urobilinogen (some reabsorbed → urine) → Stercobilin (stool color)
Normal daily bilirubin production: ~4 mg/kg/day; 70-90% from hemoglobin, rest from myoglobin and cytochromes. - Schwartz's Principles of Surgery
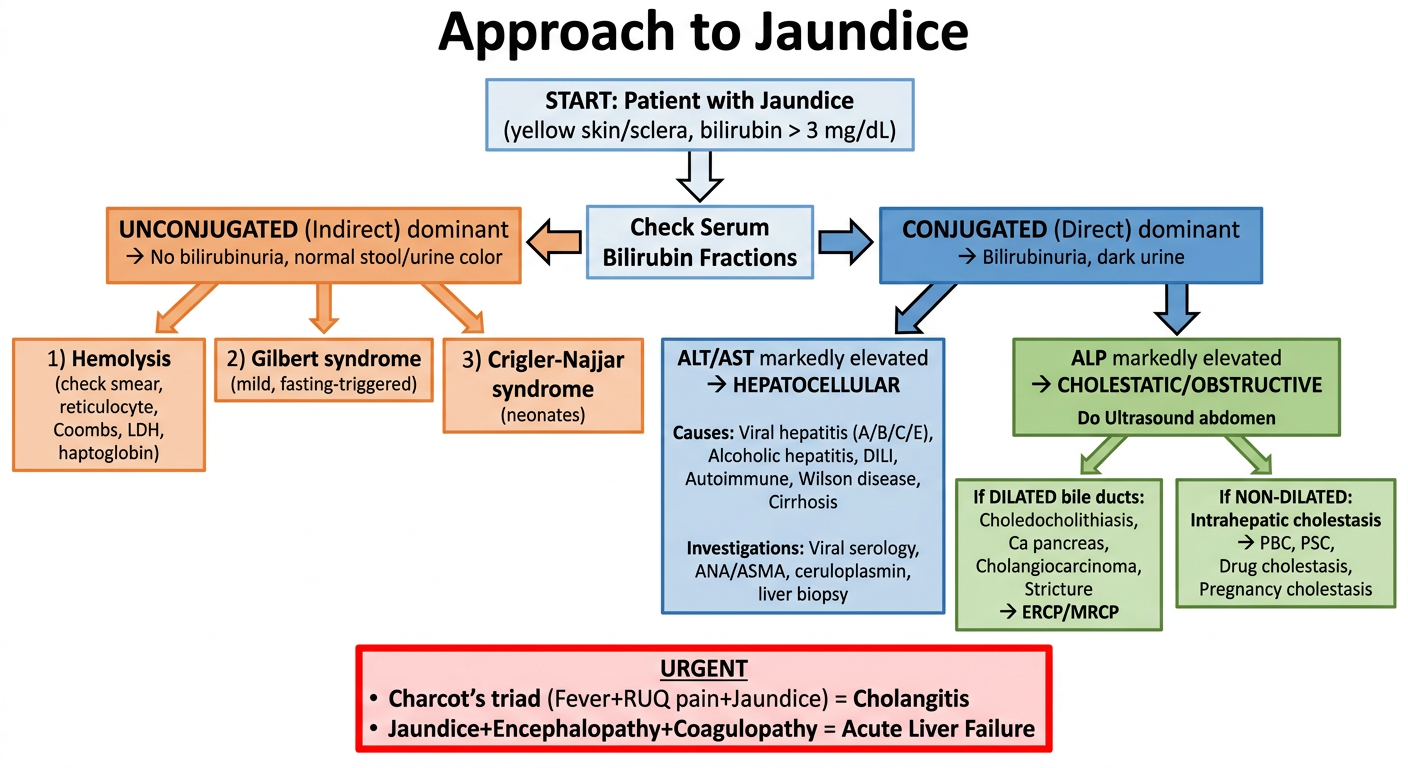
3. Classification of Jaundice
The prehepatic / intrahepatic / posthepatic framework is the foundation of your approach.
A. Prehepatic (Pre-hepatic) - Unconjugated hyperbilirubinemia
The conjugation system is overwhelmed. Bilirubin is unconjugated → NOT water-soluble → no bilirubinuria (urine is normal color), but urobilinogen is increased.
| Cause | Mechanism |
|---|
| Hemolytic anemias (hereditary spherocytosis, G6PD, sickle cell) | Excess RBC destruction |
| Immune hemolysis (autoimmune, transfusion reaction, drug-induced) | Coombs-positive |
| Microangiopathic hemolysis (TTP, HUS, DIC) | Mechanical RBC fragmentation |
| Ineffective erythropoiesis (thalassemia, megaloblastic anemia) | Intramedullary RBC destruction |
| Physiologic jaundice of newborn | Immature conjugation system |
| Gilbert syndrome | UGT1A1 gene polymorphism → mildly reduced conjugation. Bilirubin rises with fasting/stress. Benign, very common (4-7% population) |
| Crigler-Najjar Type 1 & 2 | Complete/partial absence of UGT1A1 |
B. Intrahepatic - Mixed or conjugated hyperbilirubinemia
The liver cell itself is damaged (hepatocellular) or intrahepatic bile flow is impaired (cholestatic).
| Category | Examples |
|---|
| Acute hepatocellular injury | Viral hepatitis (A, B, C, E), alcoholic hepatitis, drug-induced liver injury (DILI), ischemic hepatitis |
| Chronic hepatocellular | Cirrhosis (any cause), autoimmune hepatitis, Wilson disease, hemochromatosis |
| Intrahepatic cholestasis | Primary biliary cholangitis (PBC), Primary sclerosing cholangitis (PSC), intrahepatic cholestasis of pregnancy, drugs (chlorpromazine, anabolic steroids) |
| Infiltrative | Liver metastases, lymphoma, granulomas (TB, sarcoidosis), amyloidosis |
| Hereditary excretion defects | Dubin-Johnson syndrome, Rotor syndrome (conjugated, benign) |
C. Posthepatic (Obstructive / Cholestatic) - Conjugated hyperbilirubinemia
Bile flow is mechanically obstructed. Bilirubin regurgitates into blood. Bilirubin IS water-soluble → bilirubinuria (dark urine). Stool is pale (clay/putty-colored).
| Site | Cause |
|---|
| Choledocholithiasis (stone in CBD) | Most common cause overall |
| Periampullary carcinoma / Ca head of pancreas | Painless progressive jaundice - classic |
| Cholangiocarcinoma | |
| Benign biliary stricture | Post-surgical, post-ERCP |
| Primary sclerosing cholangitis | Multifocal strictures |
| Mirizzi syndrome | Gallstone in cystic duct/infundibulum compressing common hepatic duct |
| Pancreatitis | Edema or pseudocyst compressing CBD |
| Enlarged lymph nodes | Lymphoma, metastases compressing porta hepatis |
4. History - What to Ask
History + physical correctly categorizes jaundice as obstructive vs. non-obstructive in ~75% of cases. - Sleisenger & Fordtran's GI and Liver Disease
Key questions:
A. Nature of jaundice:
- Onset: sudden (stone, hepatitis) vs. gradual and painless (malignancy)?
- Progression: waxing-waning (hemolysis, Gilbert) vs. progressive (malignancy)?
- Duration?
B. Associated symptoms:
| Symptom | Suggests |
|---|
| RUQ pain + fever + jaundice (Charcot's triad) | Cholangitis |
| Painless jaundice | Ca head of pancreas |
| Dark urine + pale stools + pruritus | Obstructive jaundice |
| Anorexia, malaise, myalgia (viral prodrome) + fever | Viral hepatitis |
| Weight loss | Malignancy |
| Itching (pruritus) | Cholestasis |
C. Risk factors / history:
- Alcohol intake (amount, duration)
- Drug history - including OTC, herbal, ayurvedic preparations
- Blood transfusions, IV drug use, tattoos (hepatitis B/C risk)
- Sexual history
- Travel history (hepatitis A/E - feco-oral; malaria)
- Family history of liver disease, jaundice, or hemolytic anemia
- Prior biliary surgery or ERCP
- Occupation (exposure to hepatotoxins)
5. Physical Examination
Always examine in good natural light - artificial light misses early jaundice.
Systematic examination:
Vitals: Fever (hepatitis, cholangitis), hypotension (sepsis, acute liver failure)
Eyes: Scleral icterus (earliest sign), Kayser-Fleischer rings (Wilson disease - slit-lamp needed)
Skin:
- Scratch marks → pruritus → cholestasis
- Spider nevi (>5 on upper body) → chronic liver disease
- Palmar erythema, leukonychia → chronic liver disease
- Xanthelasma / xanthomas → prolonged cholestasis (PBC)
- Caput medusae → portal hypertension
- Purpura/bruising → coagulopathy
Abdomen:
| Finding | Significance |
|---|
| Hepatomegaly - tender, smooth | Hepatitis, congestion |
| Hepatomegaly - hard, nodular | Cirrhosis, metastases |
| Splenomegaly | Portal hypertension, hemolysis, lymphoma |
| Palpable gallbladder (Courvoisier's sign) | Malignant obstruction (Ca pancreas / periampullary) - not from stones (stone = chronic inflammation = non-distensible GB) |
| RUQ tenderness, Murphy's sign | Cholecystitis |
| Ascites | Cirrhosis, malignancy |
| Dilated abdominal veins | Portal hypertension |
CNS: Asterixis (liver flap) → hepatic encephalopathy
General: Cachexia → malignancy
6. Initial Laboratory Investigations
Order these in every jaundiced patient as your first-line workup:
Tier 1 - Mandatory baseline:
| Test | What it tells you |
|---|
| Serum bilirubin - total, direct (conjugated), indirect | Type of hyperbilirubinemia |
| ALT, AST | Hepatocellular injury - aminotransferases |
| ALP (Alkaline phosphatase) | Cholestasis marker |
| GGT | Confirms ALP is hepatobiliary in origin; also elevated in alcohol use |
| Albumin | Synthetic function; low in chronic disease |
| PT/INR | Synthetic function; if PT normalizes with vit K → obstruction |
| CBC | Anemia (hemolysis), leukocytosis (infection), thrombocytopenia (hypersplenism/cirrhosis) |
| Urine bilirubin & urobilinogen | Quick bedside differentiation |
Interpreting the Pattern:
| Pattern | Likely Type |
|---|
| ↑↑ ALT/AST >> ALP | Hepatocellular |
| ↑↑ ALP >> ALT/AST | Cholestatic/Obstructive |
| ↑↑ ALP + ↑ GGT | Confirms biliary source |
| Unconjugated bilirubin, no bilirubinuria | Prehepatic |
| Conjugated bilirubin, bilirubinuria, pale stools | Posthepatic |
| PT normalizes with Vitamin K | Obstruction (fat malabsorption → low vit K) |
| PT does NOT normalize with Vitamin K | Hepatocellular damage (synthetic failure) |
Urine findings at bedside:
| Urine finding | Meaning |
|---|
| Dark urine + bilirubin positive | Conjugated hyperbilirubinemia (obstructive / hepatocellular) |
| Normal colored urine | Unconjugated hyperbilirubinemia (prehepatic) |
| ↑ Urobilinogen | Hemolysis OR hepatitis |
| ↓/absent urobilinogen | Complete biliary obstruction |
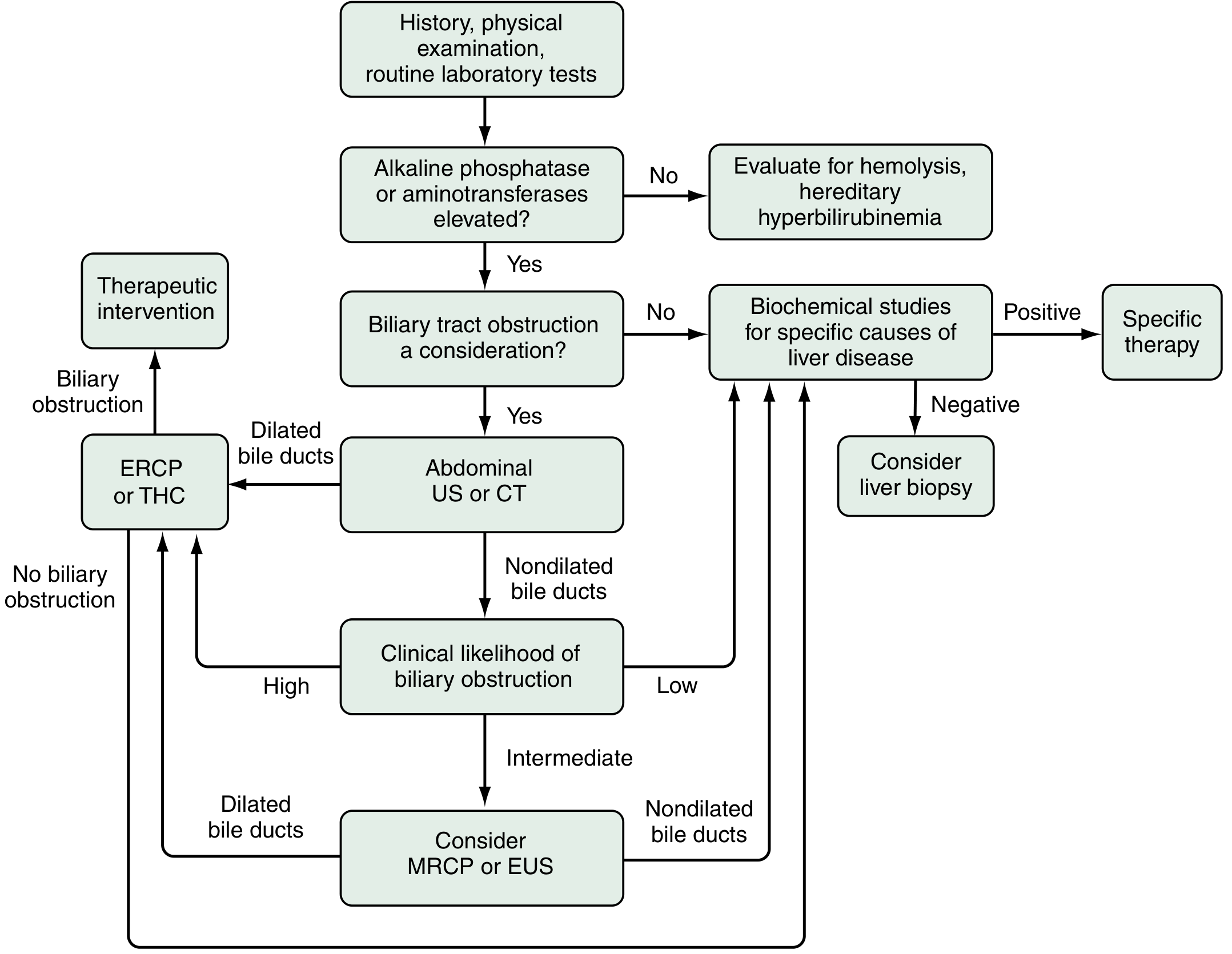
7. Diagnostic Algorithm
(From Sleisenger & Fordtran's - the standard approach)
Step-by-step logic:
-
ALP or aminotransferases elevated?
- No → Evaluate for hemolysis or hereditary hyperbilirubinemia (Gilbert, Crigler-Najjar)
- Yes → Go to step 2
-
Is biliary tract obstruction a consideration clinically?
- No → Send biochemical studies for specific liver disease (viral serology, autoimmune, metabolic)
- Yes → Go to step 3
-
Abdominal Ultrasound or CT (first-line imaging)
- Dilated bile ducts → ERCP or Transhepatic Cholangiography → therapeutic intervention
- Non-dilated bile ducts → assess clinical likelihood of obstruction
-
Clinical likelihood of obstruction?
- Low → Biochemical studies for hepatic disease
- High → ERCP/THC directly
- Intermediate → MRCP or EUS
8. Tier 2 - Specific Investigations (Based on the Working Diagnosis)
For hepatocellular disease:
| Test | Purpose |
|---|
| HBsAg, Anti-HBc, HBeAg | Hepatitis B |
| Anti-HCV, HCV RNA | Hepatitis C |
| Anti-HAV IgM | Hepatitis A |
| Anti-HEV IgM | Hepatitis E (common in India) |
| ANA, ASMA, AMA | Autoimmune hepatitis, PBC |
| Serum ceruloplasmin, urine copper | Wilson disease (young patient!) |
| Serum ferritin, transferrin saturation | Hemochromatosis |
| Serum/urine protein electrophoresis | Infiltrative/myeloma |
| Drug history review | DILI |
For hemolysis:
- Peripheral blood smear (spherocytes, schistocytes, sickle cells)
- Reticulocyte count (elevated in hemolysis)
- Coombs test (direct and indirect)
- LDH (elevated), Haptoglobin (decreased)
- G6PD assay
For obstruction:
- Abdominal USG (first line - CBD dilation, stones, mass)
- MRCP (gold standard non-invasive for biliary anatomy)
- CT abdomen with contrast (mass lesions, lymphadenopathy)
- ERCP (diagnostic + therapeutic - stone extraction, stenting)
- EUS (periampullary lesions, small CBD stones)
- Tumor markers: CA 19-9 (pancreatic/biliary malignancy), CEA, AFP
Liver biopsy indications:
- Persistent unexplained jaundice
- Suspected autoimmune hepatitis, PBC, Wilson disease, hemochromatosis
- Fibrosis staging in chronic liver disease
- NOT routinely needed in acute viral hepatitis
9. Red Flags - Do Not Miss
| Flag | Think of |
|---|
| Painless progressive jaundice in a patient >50 | Ca head of pancreas until proven otherwise |
| Charcot's triad (fever + RUQ pain + jaundice) | Cholangitis - needs urgent antibiotics and biliary drainage |
| Reynolds' pentad (Charcot's triad + hypotension + altered sensorium) | Suppurative cholangitis - surgical emergency |
| Jaundice + encephalopathy + coagulopathy | Acute Liver Failure - ICU admission |
| Jaundice in pregnancy (3rd trimester) | Acute fatty liver of pregnancy, HELLP, intrahepatic cholestasis - obstetric emergency |
| Jaundice + high fever + travel history | Falciparum malaria, leptospirosis |
| Young patient + neuropsychiatric symptoms + Kayser-Fleischer rings | Wilson disease |
10. Management Principles
Prehepatic: Treat underlying hemolysis (steroids for autoimmune, folic acid, avoid triggers in G6PD)
Intrahepatic:
- Stop hepatotoxic drugs
- Antiviral therapy for hepatitis B/C
- Steroids for autoimmune hepatitis
- Abstinence for alcoholic liver disease
- UDCA for PBC, intrahepatic cholestasis of pregnancy
Posthepatic:
- CBD stone: ERCP + sphincterotomy + stone extraction
- Benign stricture: balloon dilation ± stent (ERCP or interventional radiology)
- Malignancy: surgical resection if resectable; biliary stenting for palliation
- Cholangitis: IV antibiotics (cover gram-negatives + anaerobes) + emergency biliary drainage
Supportive in all:
- Low-fat diet in cholestasis
- Fat-soluble vitamins (A, D, E, K) supplementation in prolonged cholestasis
- Antihistamines / cholestyramine for pruritus
- Avoid nephrotoxic drugs
Quick Summary Table
| Feature | Prehepatic | Intrahepatic | Posthepatic |
|---|
| Bilirubin type | Unconjugated | Mixed | Conjugated |
| Urine color | Normal | Dark | Dark |
| Stool color | Normal/dark | Normal/pale | Pale (clay) |
| Urine bilirubin | Absent | Present | Present |
| Urobilinogen | ↑↑ | ↑ or normal | ↓/absent |
| ALT/AST | Normal | ↑↑ | Normal/mild ↑ |
| ALP | Normal | Normal/mild ↑ | ↑↑ |
| Key test | Smear, reticulocyte, Coombs | LFT pattern + serology | USG, MRCP, ERCP |
Sources: Sleisenger & Fordtran's Gastrointestinal and Liver Disease; Goldman-Cecil Medicine; Schwartz's Principles of Surgery