Explain in detail about corri cycle
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
I now have all the information needed for a thorough, well-illustrated explanation. Here is the full detailed answer:
The Cori Cycle (Lactic Acid Cycle)
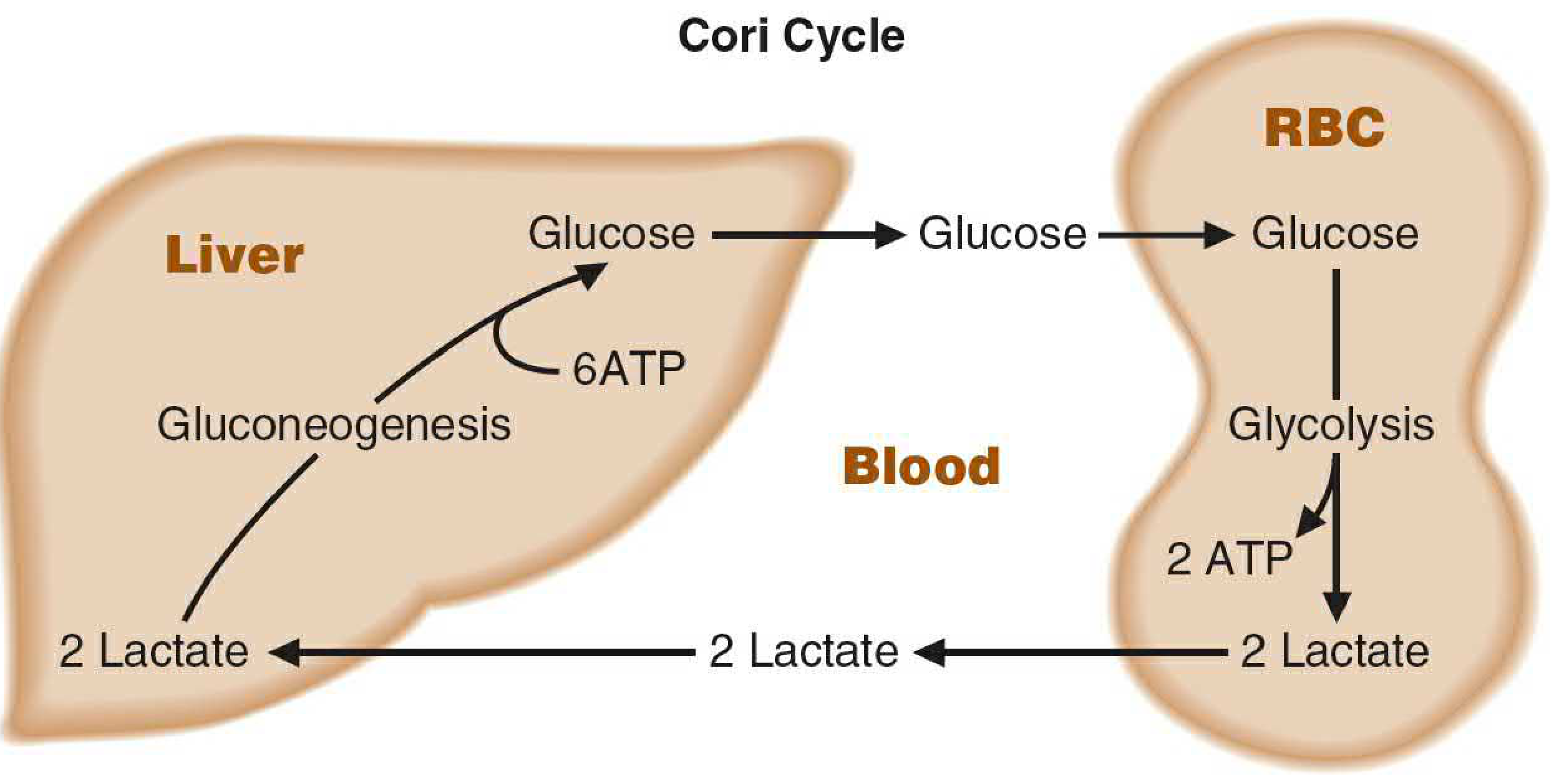
Figure: The Cori cycle. Glucose from the liver is converted by glycolysis in peripheral tissues (e.g., RBCs, muscle) to lactate, which returns to the liver for reconversion to glucose via gluconeogenesis.
1. Definition and Historical Context
The Cori cycle (also called the lactic acid cycle) is a metabolic cycle in which lactate produced by peripheral tissues undergoing anaerobic glycolysis is transported via the bloodstream to the liver, where it is oxidized back to pyruvate and then converted to glucose by gluconeogenesis. The newly synthesized glucose is then released back into the circulation for use by those same peripheral tissues, thus completing the cycle.
It is named after Carl and Gerty Cori, who received the Nobel Prize in Physiology or Medicine in 1947 for discovering the mechanism of glycogen metabolism and describing this interorgan glucose-lactate exchange.
2. Why the Cori Cycle is Necessary
Certain tissues cannot perform aerobic respiration and must rely exclusively or predominantly on anaerobic glycolysis for ATP:
| Tissue | Reason for anaerobic dependence |
|---|---|
| Red blood cells (RBCs) | No mitochondria |
| Kidney medulla | Limited oxygen supply |
| Lens and cornea of the eye | Avascular, low O2 |
| Testes | Limited O2 diffusion |
| Exercising skeletal muscle | O2 demand exceeds supply at high intensity |
| White blood cells | Predominantly glycolytic |
| Skin | Some lactic acid secreted in sweat |
In anaerobic glycolysis, glucose → 2 pyruvate → 2 lactate (via LDH), generating only 2 ATP per glucose. This lactate accumulates and must be cleared. The Cori cycle elegantly recycles it.
3. Step-by-Step Mechanism
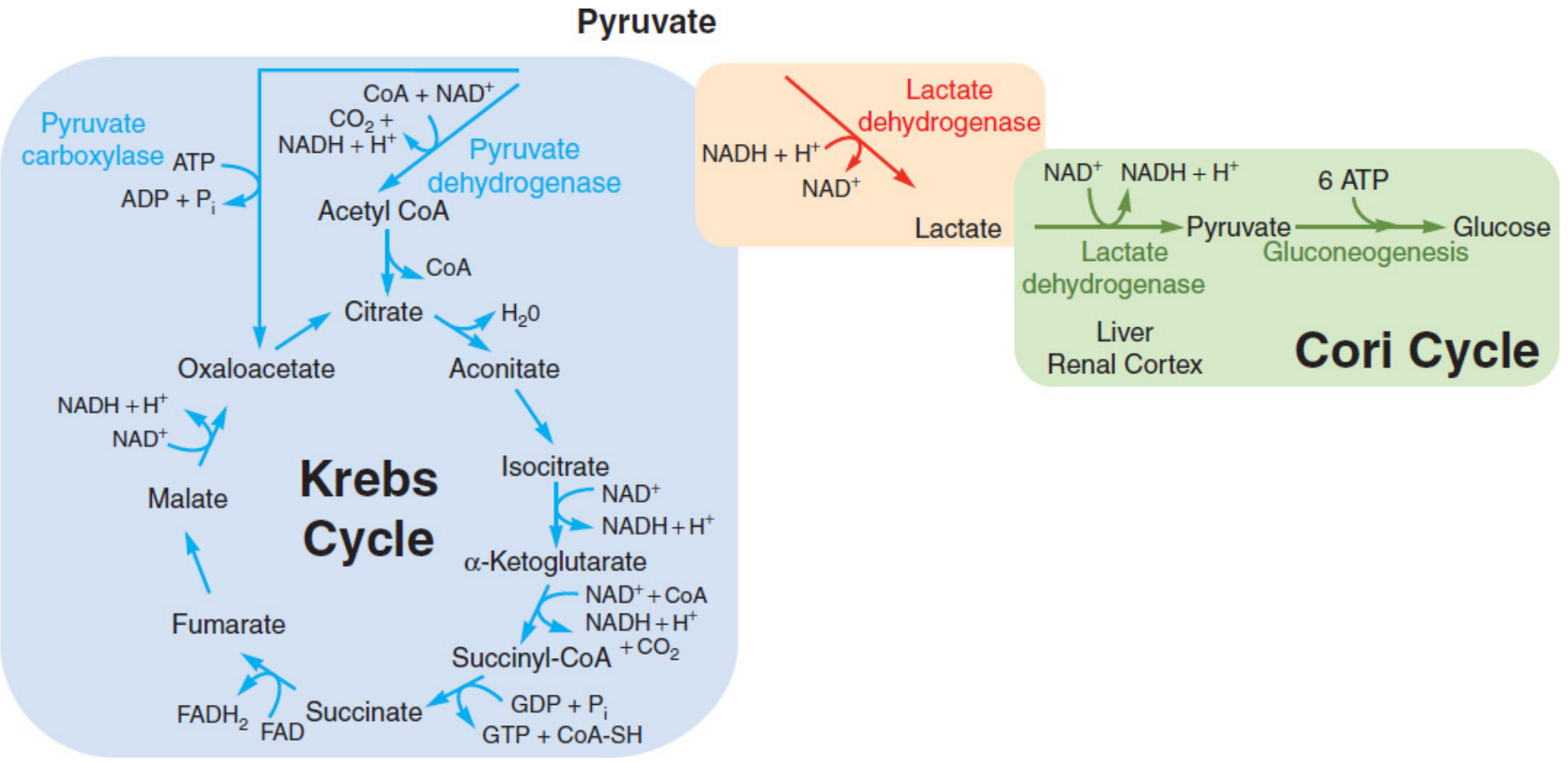
Figure: Pyruvate at the crossroads - under hypoxia, pyruvate is reduced to lactate (red box). The Cori cycle (green box) converts this lactate back to glucose in the liver/renal cortex.
Step 1 - Peripheral Tissue (Muscle/RBC) - Glucose to Lactate
- Glucose enters the cell and undergoes glycolysis in the cytoplasm.
- Glucose → 2 pyruvate + 2 ATP + 2 NADH
- Because there is no oxygen (or not enough), pyruvate cannot enter the mitochondria via pyruvate dehydrogenase.
- Instead, lactate dehydrogenase (LDH) catalyzes:
- Pyruvate + NADH + H⁺ → Lactate + NAD⁺
- This regenerates NAD⁺, which is critical because without it, glycolysis would stop (no oxidized NAD⁺ to accept electrons at glyceraldehyde-3-phosphate dehydrogenase step).
- Lactate and H⁺ are co-transported out of the cell via monocarboxylate transporters (MCTs) into the interstitial fluid and then the bloodstream.
Step 2 - Blood Transport
Lactate circulates in the blood to the liver (and to a lesser extent, the renal cortex). In a resting 70 kg man, approximately 115 g of lactate is produced daily:
- RBCs: ~29 g/day
- Skin: ~20 g/day
- Brain: ~17 g/day
- Skeletal muscle: ~16 g/day
- Renal medulla: ~15 g/day
Step 3 - Liver (and Renal Cortex) - Lactate to Glucose
The liver is exceptionally efficient at clearing lactate when oxygen is available:
- Lactate enters hepatocytes.
- LDH (H4 isoform, favoring lactate → pyruvate):
- Lactate + NAD⁺ → Pyruvate + NADH + H⁺
- Pyruvate enters gluconeogenesis:
- Pyruvate → Oxaloacetate (via pyruvate carboxylase, mitochondria, requires ATP + CO₂)
- Oxaloacetate → Phosphoenolpyruvate (via PEPCK)
- Reverse of glycolysis (using phosphatase steps at fructose-1,6-bisphosphate and glucose-6-phosphate to bypass irreversible glycolytic steps)
- 2 Lactate → 1 Glucose (net)
- The glucose is exported back into the bloodstream.
4. Energy Balance (The Cost of the Cycle)
This is the critical concept often tested:
| Location | Process | ATP |
|---|---|---|
| Peripheral tissue (RBC/muscle) | Glycolysis: Glucose → 2 Lactate | +2 ATP (gained) |
| Liver | Gluconeogenesis: 2 Lactate → Glucose | -6 ATP (consumed) |
| Net for the whole cycle | -4 ATP |
The Cori cycle has a net cost of 4 ATP per cycle. This means:
- The peripheral tissue gains 2 ATP from anaerobic glycolysis.
- The liver spends 6 ATP to reconvert the 2 lactate molecules back into glucose.
- The energy deficit in the liver is paid for by fat oxidation (beta-oxidation) - specifically, fatty acids provide the ATP needed by the liver to run gluconeogenesis.
"The Cori cycle and the glucose-alanine cycle do not yield new carbon skeletons. Rather, both cycles transfer energy - and the glucose-alanine cycle also transfers nitrogen - between muscle and liver. The energy for hepatic glucose synthesis comes from oxidation of fat in the liver." - Medical Physiology
5. Key Enzymes Involved
In Peripheral Tissues:
- Hexokinase / Glucokinase - phosphorylates glucose (traps it in cell)
- Phosphofructokinase-1 (PFK-1) - rate-limiting enzyme of glycolysis
- Pyruvate kinase - produces pyruvate
- Lactate dehydrogenase (LDH - M4 isoform) - converts pyruvate → lactate (favors this direction in skeletal muscle)
In the Liver:
- Lactate dehydrogenase (LDH - H4 isoform) - converts lactate → pyruvate (H4 favors this direction in aerobic tissues)
- Pyruvate carboxylase - pyruvate → oxaloacetate (mitochondria)
- PEPCK (phosphoenolpyruvate carboxykinase) - oxaloacetate → PEP
- Fructose-1,6-bisphosphatase - bypasses PFK-1 (irreversible step)
- Glucose-6-phosphatase - dephosphorylates G6P → free glucose for export (liver and kidney only)
6. LDH Isoforms and the Cori Cycle
LDH is a tetramer made of two subunits - M (muscle/A) and H (heart/B) - giving rise to 5 isoforms:
| Isoform | Location | Direction Favored |
|---|---|---|
| M4 (LDH-5) | Skeletal muscle | Pyruvate → Lactate |
| H4 (LDH-1) | Heart, liver | Lactate → Pyruvate |
| M3H1, M2H2, M1H3 | Intermediate tissues | Intermediate |
This tissue-specific expression is a fine-tuned mechanism: muscle LDH makes lactate; liver/heart LDH clears it.
7. Physiological Contexts
During Exercise
When muscle contracts intensely, O2 supply is insufficient and lactate floods the blood. Post-exercise (the "oxygen debt" / excess post-exercise oxygen consumption - EPOC), the liver uses O2 to clear the lactate load via the Cori cycle. Some lactate is also directly oxidized in the heart and resting muscle (which have H4 LDH and rich mitochondria).
During Fasting/Starvation
In the first hours of fasting, the brain consumes glucose at ~4-5 g/hr. Obligate anaerobic tissues convert glucose to lactate, which the liver recycles via the Cori cycle to regenerate glucose - maintaining blood sugar. This uses fat as the ultimate energy donor.
During prolonged starvation, the kidneys become a major site of gluconeogenesis (contributing ~40% after 48 hours of fasting), participating alongside the liver in the Cori cycle.
In Critical Illness / Shock
Large wounds, burns, sepsis, or hemorrhagic shock produce enormous lactate loads. The liver clears these via the Cori cycle. Elevated serum lactate in critically ill patients reflects both increased production AND impaired hepatic clearance.
"Even patients with cirrhosis do not exhibit elevated lactate levels at baseline, although the rate at which a lactate load is cleared does correlate with liver function." - Mulholland and Greenfield's Surgery
The Kidneys
The kidneys metabolize and/or actively excrete 20-30% of serum lactate. Significant renal dysfunction therefore also impairs lactate clearance. - Mulholland and Greenfield's Surgery
8. The Glucose-Alanine Cycle (Cahill Cycle) - A Parallel
The Cori cycle has an important analog:
- In muscle, alanine aminotransferase transfers an amino group from other amino acids to pyruvate → alanine
- Alanine travels to the liver, where its amino group is removed (urea cycle) and the carbon skeleton is used for gluconeogenesis
- This carries both energy (as carbon) and nitrogen (as amino groups) from muscle to liver
Alanine serves as a carrier of ammonia and of the carbons of pyruvate from skeletal muscle to liver via the Cori cycle analog. The two cycles together represent the major interorgan carbon trafficking during fasting and exercise.
9. Clinical Significance
| Condition | Relevance to Cori Cycle |
|---|---|
| Lactic acidosis | Overproduction of lactate exceeds liver's clearance capacity; blood pH falls |
| Liver failure (cirrhosis, fulminant hepatitis) | Reduced gluconeogenic capacity - impaired lactate clearance |
| Renal failure | Impaired renal lactate excretion/metabolism |
| Type B lactic acidosis (metformin toxicity) | Metformin inhibits hepatic gluconeogenesis, blocking Cori cycle |
| Von Gierke disease (GSD type 1) | Glucose-6-phosphatase deficiency - glucose cannot be released from liver; exaggerated lactate accumulation |
| Septic/hemorrhagic shock | Massive lactate production from hypoperfused tissues |
| Tumor metabolism (Warburg effect) | Large tumors use anaerobic glycolysis even in O2 (producing lactate that nearby cells oxidize - a "mini Cori cycle") |
10. Summary
| Feature | Detail |
|---|---|
| Other names | Lactic acid cycle |
| Discoverers | Carl and Gerty Cori (Nobel 1947) |
| Primary sites | Peripheral tissues (RBC, muscle) ↔ Liver |
| Net reaction in periphery | Glucose → 2 Lactate (+2 ATP) |
| Net reaction in liver | 2 Lactate → Glucose (-6 ATP) |
| Net ATP cost | -4 ATP per cycle |
| Energy source for liver | Beta-oxidation of fatty acids |
| Key enzyme (periphery) | LDH M4 isoform |
| Key enzyme (liver) | LDH H4 + gluconeogenic enzymes |
| Main function | Recycle lactate; maintain blood glucose; transfer energy between tissues |
Sources:
- Biochemistry, 8th ed - Lippincott Illustrated Reviews, p. 129 (Cori cycle in gluconeogenesis)
- Basic Medical Biochemistry - A Clinical Approach, 6e, p. 804-805 (lactate production table, Figure 22.12)
- Medical Physiology (Boron & Boulpaep), p. 1392-1412 (Cori cycle during fasting)
- Mulholland and Greenfield's Surgery, 7e, p. 77-78 (Cori cycle in surgical physiology)
- Sleisenger and Fordtran's GI and Liver Disease (Cori cycle during starvation)
This is a shared conversation. Sign in to Orris to start your own chat.