Visual acuity
Reading File
Finding Sources
Searching the Web
visual acuity definition measurement Snellen chart ophthalmology
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have rich content from multiple authoritative sources. Here is the full answer:
Visual Acuity
Definition
Visual acuity (VA) is the ability of the eye to resolve fine spatial detail - specifically, the minimum angle of separation (subtended at the nodal point of the eye) between two objects that allows them to be perceived as distinct. It reflects the clarity or sharpness of vision and depends on both optical factors (the quality of the eye's refractive system) and neural factors (the health of the retina, optic pathways, and visual cortex).
Physiological Basis
The fovea centralis is the site of maximum VA. It is a rod-free, cone-dense region of the retina where each cone synapses on a single bipolar cell, which in turn synapses on a single ganglion cell - providing a direct, one-to-one pathway to the brain. There are very few overlying cells and no blood vessels, minimizing optical interference.
When a point of light is focused on the retina, the resulting spot has a minimum diameter of about 11 micrometers due to optical imperfections in the lens system. The foveal cones average ~1.5 micrometers in diameter. Because the light spot is brightest centrally and fades at its edges, two separate points can just be resolved when their retinal images are ~2 micrometers apart - slightly wider than one foveal cone.
Expressed as an angle, normal VA corresponds to ~25 seconds of arc - meaning two bright point sources 10 meters away can just be distinguished when they are 1.5-2.0 mm apart. Outside the foveal area, VA falls off rapidly - more than 10-fold - because progressively more rods and cones share each optic nerve fiber in the periphery.
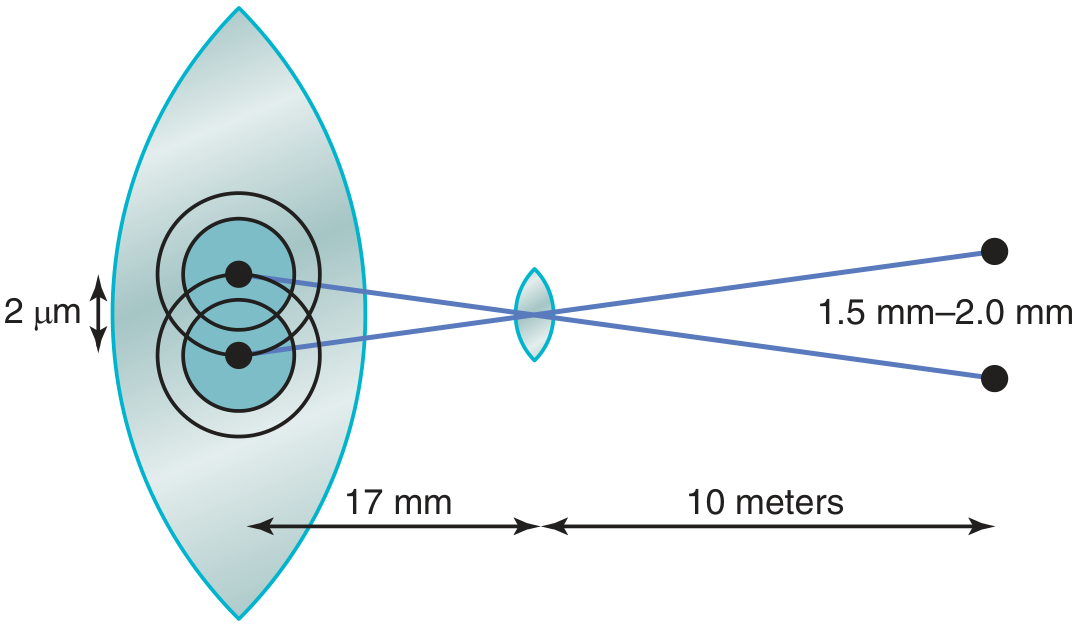
Figure: Two point sources 10 m away, separated by 1.5-2.0 mm, produce retinal images ~2 μm apart at the fovea. - Guyton & Hall Textbook of Medical Physiology
Measurement
Snellen Chart (Distance VA)
The most widely used clinical tool, developed by Herman Snellen in 1862. It consists of progressively smaller black letters (optotypes) on a white background, read from a standard distance of 6 meters (20 feet).
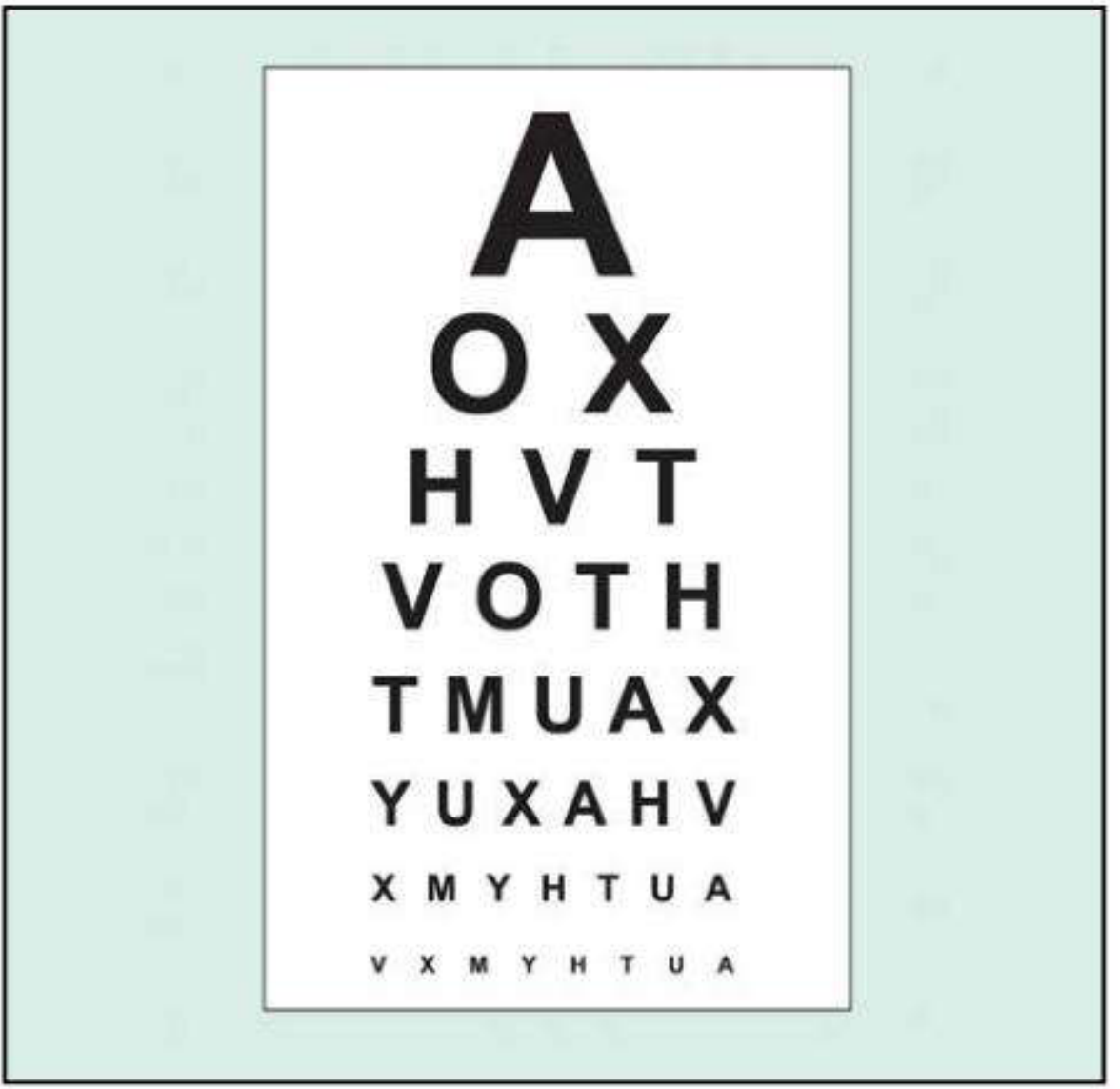
Fig. 1.1 Snellen visual acuity chart. - Kanski's Clinical Ophthalmology
Each optotype is designed so that its critical detail (stroke width) subtends 1 minute of arc at the designated distance. The full letter subtends 5 minutes of arc.
Notation
VA is expressed as a fraction:
| Notation | Meaning |
|---|---|
| 6/6 (metric) or 20/20 (imperial) | Normal VA: sees at 6 m what a normal eye sees at 6 m |
| 6/12 | Sees at 6 m what a normal eye sees at 12 m (reduced VA) |
| 6/60 | Sees at 6 m what a normal eye sees at 60 m (severe reduction) |
| 20/200 | Sees at 20 ft what a normal eye sees at 200 ft |
Normal corrected VA in young adults is often better than 6/6.
Best-corrected VA (BCVA): VA measured with optimal refractive correction (glasses/contact lenses).
Testing Protocol
- Test each eye separately, starting with the worse eye, while occluding the other
- First measure with the patient's own refractive correction (glasses/contacts)
- Push the patient to read every possible letter - do not accept premature stopping
- If VA is less than 6/6, repeat using a pinhole
Pinhole VA
A pinhole aperture (~1 mm diameter) reduces the blur circle of defocused light, effectively compensating for refractive error. If VA improves with the pinhole, the deficit is likely refractive (correctable). If VA does not improve or worsens, the cause is likely pathological (e.g., macular disease, posterior lens opacity).
Grading Very Poor VA
When VA is too poor for the Snellen chart, these descriptors are used (in descending order):
| Grade | Abbreviation | Description |
|---|---|---|
| Counting fingers | CF | Patient counts fingers held at a specified distance (usually 1 m) |
| Hand movements | HM | Patient distinguishes whether examiner's hand is moving |
| Perception of light | PL | Patient detects presence of a light only |
| No perception of light | NPL | Complete blindness |
Near VA
Near VA is measured with a near reading chart (e.g., Jaeger notation or N-point notation) held at standard reading distance (~33 cm). It is important for assessing presbyopia, macular function, and reading ability.
VA in Special Populations
Children (Pre-verbal)
Quantitative testing uses preferential looking tests (e.g., Teller/Keeler acuity cards, Cardiff acuity cards). These exploit the fact that infants prefer patterned stimuli over uniform fields. Qualitative assessment includes fixation-and-follow behavior, response to occlusion of each eye, and (for infants with strabismus) fixation grading and the rotation test. Pattern visual evoked potentials (VEP) can also estimate spatial acuity electrophysiologically.
Binocular vs. Monocular VA
Binocular VA is usually slightly superior to the better monocular VA, provided both eyes have roughly equal vision. This binocular summation effect is reduced or lost when there is a significant inter-eye VA difference.
Factors Affecting VA
| Factor | Effect |
|---|---|
| Refractive error (myopia, hyperopia, astigmatism) | Reduces VA; correctable by lenses |
| Media opacity (corneal scar, cataract, vitreous hemorrhage) | Reduces VA |
| Macular disease (AMD, diabetic maculopathy) | Reduces central VA |
| Optic nerve disease | Reduces VA ± color vision |
| Amblyopia | Unilateral or bilateral reduced VA from abnormal visual development |
| Pupil size | Very small or very large pupils reduce VA |
| Illumination | Low light reduces VA (shifts from cone to rod-dominated vision) |
Sources:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., pp. 17-18
- Guyton and Hall Textbook of Medical Physiology, p. 627
- Ganong's Review of Medical Physiology, 26th ed., p. 206
How does refractive error affect visual acuity?
Finding Sources
Searching the Web
refractive error mechanism visual acuity myopia hyperopia astigmatism
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Excellent - I now have all the content I need for a thorough, well-illustrated answer.
How Refractive Error Affects Visual Acuity
The Normal (Emmetropic) Eye
In emmetropia, the refractive power of the cornea and lens system is perfectly matched to the axial length of the eye. Parallel light rays from distant objects converge to a sharp point focus exactly on the retina, producing maximum VA. The foveal cones receive a crisp, well-defined image.
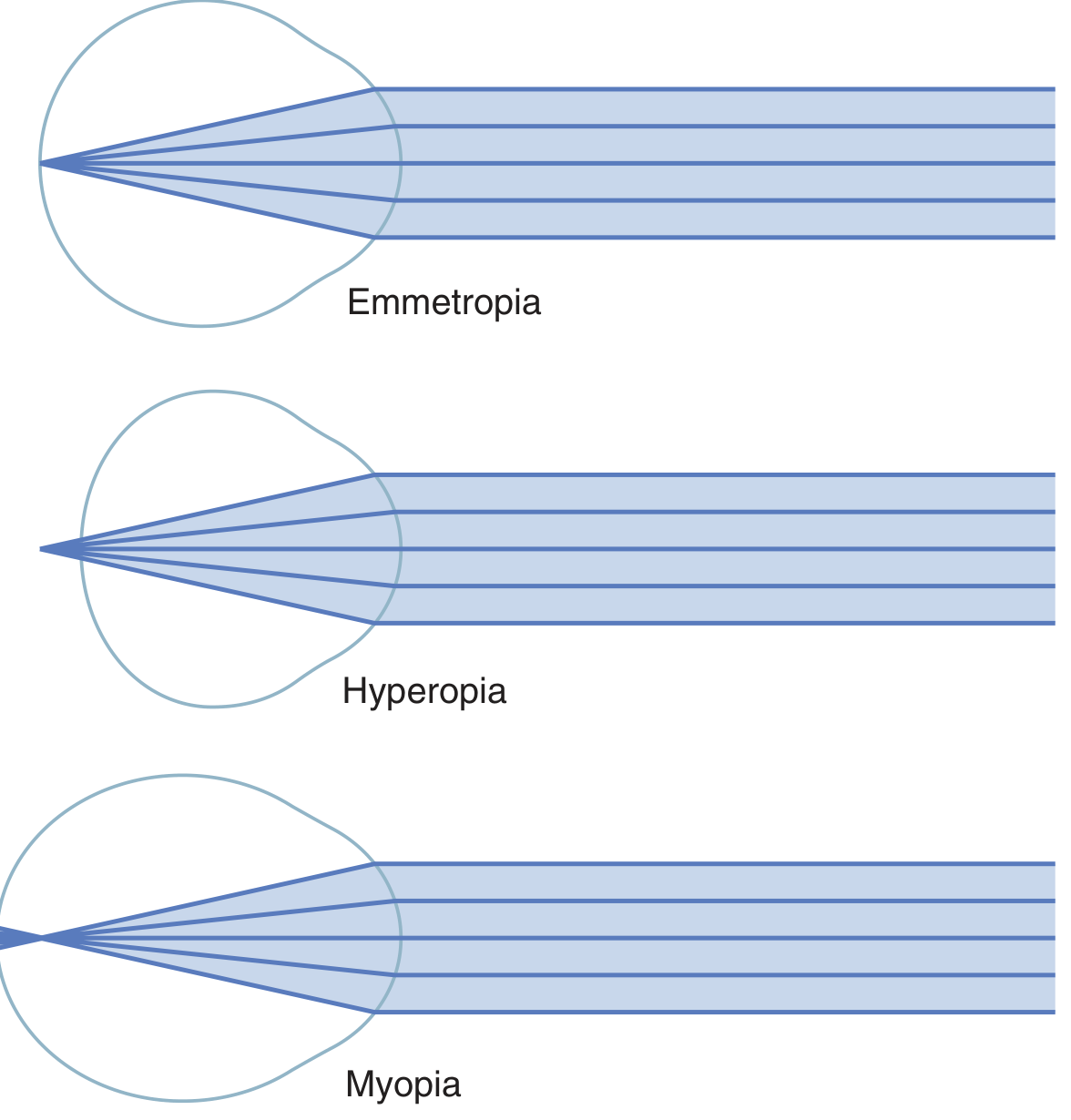
Figure: Parallel light rays focus on the retina in emmetropia, behind the retina in hyperopia, and in front of the retina in myopia. - Guyton & Hall Textbook of Medical Physiology
The Mechanism of VA Reduction
When focus falls off the retina, instead of a sharp point of light hitting a photoreceptor, a blur circle (or blur ellipse in astigmatism) is projected. The larger the blur circle, the more photoreceptors it covers simultaneously, reducing the eye's ability to distinguish fine detail. This directly degrades VA in a dose-dependent manner - the greater the refractive error (measured in dioptres, D), the worse the VA.
Types of Refractive Error and Their Effects
1. Myopia (Nearsightedness)
- Cause: The eyeball is too long anteroposteriorly, or the lens/cornea has excessive refractive power
- Effect on VA: Parallel light from distant objects converges to a focal point in front of the retina. By the time the rays reach the retina they have diverged again, producing a blur circle
- Distance VA: Reduced (blurred for distant objects)
- Near VA: Preserved - as an object moves closer, its diverging rays require greater convergence, and at some point the focus falls on the retina. The myope has a definite far point for clear vision
- Compensation: The ciliary muscle cannot weaken the lens further (it is already maximally relaxed), so no accommodation can compensate
- Correction: Concave (minus power, diverging) lens - diverges incoming rays before they enter the eye, shifting the focal point back onto the retina
2. Hyperopia (Farsightedness / Hypermetropia)
- Cause: The eyeball is too short, or the refractive power of the lens system is too weak
- Effect on VA: Parallel light from distant objects has not yet converged when it reaches the retina - the focal point lies behind the retina
- Partial compensation by accommodation: The ciliary muscle can contract to increase lens curvature (accommodation), adding refractive power. Mild hyperopia may thus be fully corrected by accommodation, with no VA loss - but this requires sustained ciliary effort, causing eyestrain (asthenopia), headaches, and fatigue
- In high or uncorrected hyperopia: Once accommodation is exhausted, both distance and near VA are impaired. In old age (presbyopia), when the lens loses elasticity, even mild hyperopia can no longer be compensated
- Prolonged convergence associated with constant accommodation can eventually produce strabismus
- Correction: Convex (plus power, converging) lens
3. Astigmatism
- Cause: Non-uniform curvature of the cornea (or occasionally the lens) - different meridians have different radii of curvature
- Effect on VA: Light rays in different planes focus at different distances from the retina. One meridian may be in focus while the perpendicular meridian is not - producing a blurred, distorted retinal image at all distances
- Critically: Accommodation cannot compensate for astigmatism, because the lens changes curvature approximately equally in all meridians. Therefore, without correction, the astigmatic eye never produces a fully sharp image at any distance
- Correction: A cylindrical lens equalises refraction across all meridians. Often combined with a spherical component (spherocylindrical lens prescription)
4. Presbyopia
- Cause: Age-related loss of lens elasticity, reducing accommodative amplitude
- Effect on VA: Progressive loss of near VA (usually apparent from ~40-45 years). Distance VA is unaffected in emmetropes, but near objects can no longer be brought into focus
- Correction: Convex (plus) reading lenses, bifocals, or multifocals
5. Anisometropia
- A significant difference in refractive error between the two eyes
- The blurred image from the more ametropic eye can suppress cortical processing of that eye's input
- In children, this is a leading cause of amblyopia (permanent VA reduction due to abnormal visual development), because the brain preferentially develops connections from the better-seeing eye
Summary Table
| Type | Structural Defect | Focal Point | VA Impaired | Correcting Lens |
|---|---|---|---|---|
| Myopia | Axial length too long / excess power | In front of retina | Distance | Concave (minus) |
| Hyperopia | Axial length too short / insufficient power | Behind retina | Distance + near (when accommodation fails) | Convex (plus) |
| Astigmatism | Non-uniform corneal curvature | Multiple planes | All distances | Cylindrical |
| Presbyopia | Reduced lens elasticity | Behind retina for near | Near only | Convex reading lens |
Correction Options Beyond Spectacles
- Contact lenses - sit closer to the nodal point, correcting the same refractive error with a different (usually lower) power
- LASIK / surface ablation (PRK) - laser reshaping of the corneal curvature to achieve emmetropia; corrects myopia, hyperopia, and astigmatism
- SMILE - small-incision lenticule extraction, for myopia and myopic astigmatism
- Phakic intraocular lens (ICL) - implanted behind the iris; used for high refractive errors beyond laser range
- Clear lens extraction - removal and replacement of the natural lens with an IOL; eliminates both refractive error and future cataract risk but removes all accommodation
Sources:
- Guyton and Hall Textbook of Medical Physiology, pp. 625-626
- Ganong's Review of Medical Physiology, 26th ed., pp. 200-202
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., pp. 299-302
How does the pinhole test help diagnose refractive vs pathological VA loss?
Finding Sources
Finding Sources
Searching the Web
pinhole test visual acuity refractive vs pathological blur mechanism ophthalmology
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Now I have everything needed for a thorough answer.
The Pinhole Test: Diagnosing Refractive vs. Pathological VA Loss
The Optical Principle
In any eye with refractive error, incoming light rays from all parts of the pupil converge at the wrong distance - forming a blur circle on the retina instead of a sharp point. The wider the pupil, the more peripheral (oblique) rays enter, and the larger the blur circle becomes.
A pinhole aperture (~1 mm diameter) acts as a spatial filter: it blocks all peripheral, off-axis rays and admits only the narrow central bundle of light. These central rays are nearly parallel regardless of whether the eye's refractive power is correct, so they produce a much smaller retinal spot - effectively bypassing the need for perfect optical focus. The result is an increased depth of focus, which compensates for moderate refractive error.
In simple terms: the pinhole removes the blur circle that refractive error creates. If the blur circle was the cause of poor VA, VA improves. If the retina, optic nerve, or visual pathways are damaged, there is no blur circle to remove - the information is simply lost at source, and the pinhole cannot help.
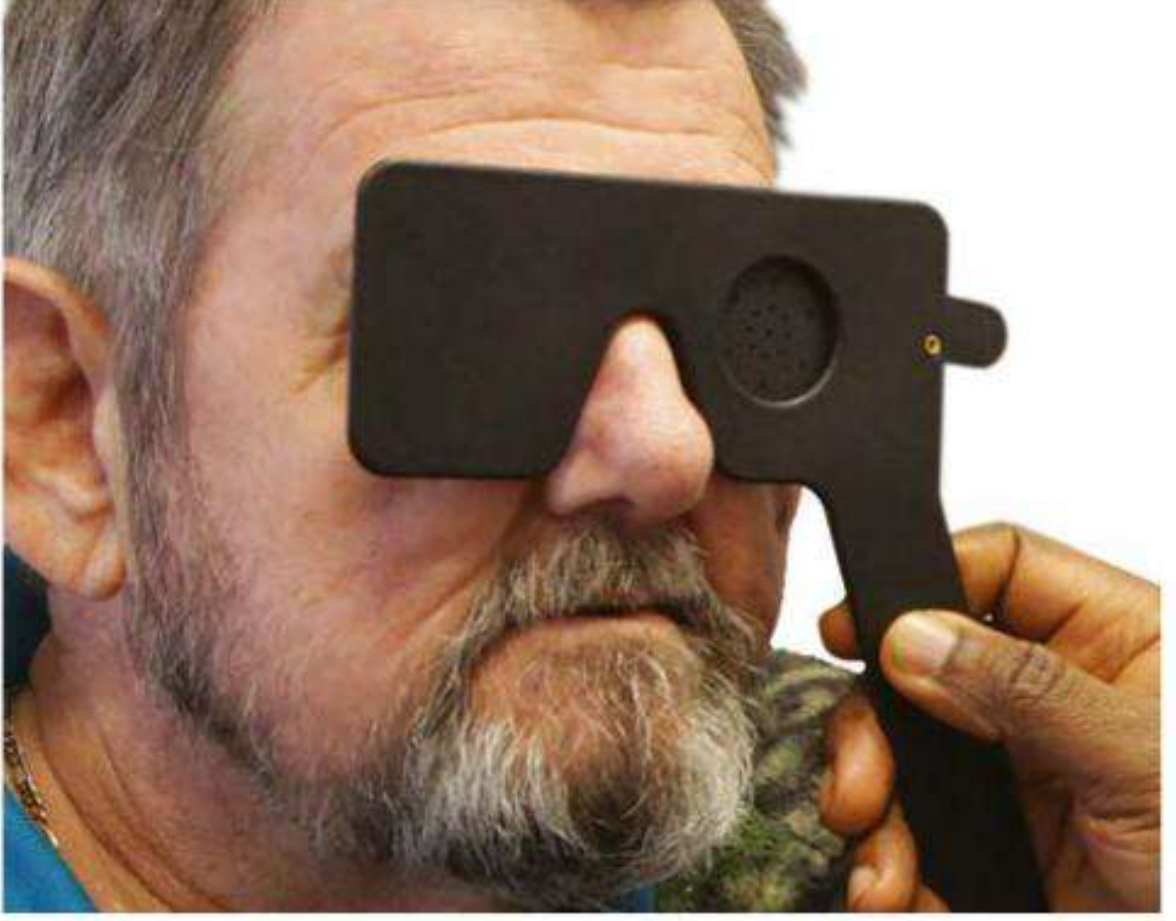
Fig. 1.2 Pinhole occluder. - Kanski's Clinical Ophthalmology
Interpreting the Result
| Pinhole Result | Interpretation | Next Step |
|---|---|---|
| VA improves (by 1+ Snellen lines) | Reduced VA is primarily from an uncorrected or under-corrected refractive error | Refer for formal refraction and spectacle/contact lens prescription |
| VA unchanged | VA loss is not from refractive error | Investigate for retinal, optic nerve, or neurological pathology |
| VA worsens | Suggests macular disease, posterior lens opacity, or significant media opacity | Urgent ophthalmic review |
"The pinhole permits a narrow shaft of light to fall on the fovea, eliminating the need for light to be correctly focused by the anterior segments of the eye. If the acuity improves to near normal with a pinhole, one can conclude that the reduced vision relates to a refractive error caused by a defect in the optical media rather than a neurological cause."
- Adams and Victor's Principles of Neurology, 12th ed.
"If there is nonrefractive pathology, such as retinal edema or aqueous hemorrhage, causing the acuity deficit, pinhole testing will show no improvement in the (poor) visual acuity."
- Rosen's Emergency Medicine
What the Pinhole Can and Cannot Rule Out
Optical media that the pinhole bypasses (refractive causes)
The pinhole compensates for any condition that produces an unfocused retinal image:
- Uncorrected myopia, hyperopia, astigmatism
- Presbyopia
- Early/mild cataract (where the lens is still partially transparent but has irregular refraction)
- Minor corneal irregularity (early keratoconus, dry eye surface change)
Pathological causes that the pinhole does NOT improve
These involve destruction of the neural apparatus - no amount of optical sharpening can recover lost neural signal:
- Macular disease (age-related macular degeneration, diabetic maculopathy, macular hole) - the photoreceptors themselves are damaged
- Optic nerve disease (optic neuritis, ischaemic optic neuropathy, glaucoma) - axons transmitting the signal are lost
- Retinal vascular disease (central/branch retinal artery or vein occlusion, retinal ischaemia)
- Vitreous haemorrhage / dense media opacity - too much light is blocked entirely, not just defocused
- Cortical/neurological visual loss (occipital stroke, posterior cortical atrophy)
Important exceptions and caveats
-
Macular disease and posterior lens opacities may actually make VA worse through a pinhole - reducing retinal illumination in an already compromised macula, or diffracting light at a dense posterior capsule opacity, can actively degrade the limited vision that remains. This is the reverse of the expected response and is a clinically useful sign of pathology.
-
Dense media opacities (severe cataract, dense vitreous haemorrhage, significant corneal scar) also fail to improve - not because the neural pathway is damaged, but because too little light reaches the retina at all through a 1 mm aperture. This is a limitation: a negative pinhole result in such cases does not necessarily mean neural disease.
-
Diffraction limit: Making the aperture too small introduces diffraction artifacts that can slightly reduce resolution even in a normal eye. The standard ~1 mm pinhole is calibrated to minimise this.
-
The pinhole is not a substitute for formal refraction. A patient whose VA improves with pinhole still needs a proper refraction to quantify and correct their refractive error. The pinhole only establishes that correction is possible, not what that correction is.
Clinical Protocol
- Measure unaided (uncorrected) VA first
- Measure VA with the patient's own glasses/contacts (best corrected VA)
- If best corrected VA is less than 6/6 (or if no correction is available), test with a pinhole:
- Commercial multi-hole occluder, or an 18-gauge needle hole punched through a card/index card is acceptable in the ED
- Test one eye at a time with the other fully occluded
- Record both values: e.g., "VA 6/18 unaided, 6/6 with pinhole" (refractive cause) vs. "VA 6/18 unaided, 6/18 with pinhole" (pathological cause)
Summary
The pinhole is a bedside tool that separates optical blur from neural damage. Its logic is simple: if sharpening the retinal image (by eliminating peripheral rays) restores VA, the problem is in the eye's optics. If VA remains unchanged, the problem lies at or beyond the retina - in the photoreceptors, optic nerve, or visual cortex - and requires further investigation with fundoscopy, visual field testing, imaging, or electrophysiology.
Sources:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., p. 17
- Adams and Victor's Principles of Neurology, 12th ed., p. 252
- Harrison's Principles of Internal Medicine, 22nd ed., p. 264
- Tintinalli's Emergency Medicine: A Comprehensive Study, p. 1470 (chapter)
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 1470
- Rosen's Emergency Medicine, p. 215
This is a shared conversation. Sign in to Orris to start your own chat.