Clinical anatomy of the ear. Physiology and research methods of auditory and vestibular analyzers. Explain in detail
Reading File
Finding Sources
Finding Sources
Searching Images
anatomy of the ear clinical diagram
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching Images
cochlea inner ear anatomy cross section diagram
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Searching Images
vestibular system semicircular canals utricle saccule
Reading File
Loading Image
Loading Image
Reading File
Searching Images
audiometry hearing test tympanometry research methods
I now have comprehensive material from the textbooks and images to compile a thorough answer. Let me synthesize everything.
Clinical Anatomy of the Ear — Physiology and Research Methods of Auditory and Vestibular Analyzers
I. OVERVIEW AND EMBRYOLOGY
The ear is housed within the temporal bone, which articulates with the sphenoid, parietal, occipital, and zygomatic bones. The temporal bone has four embryologically distinct components: squamous, mastoid, petrous, and tympanic parts.
Embryological development:
- The outer and middle ears derive from the first and second branchial arches and the first branchial groove/pouch
- The inner ear arises from the otic placode (~3 weeks gestation), which invaginates to form the otocyst (otic vesicle) — the precursor of the entire membranous labyrinth
- The otocyst has two parts:
- Pars superior → semicircular canals and ampullae (develop in order: superior, posterior, lateral)
- Pars inferior → saccule and cochlea
- The cochlear duct reaches 2.5 turns by 10 weeks, adult size by 20 weeks, and the organ of Corti becomes functional at ~21 weeks
- The endolymphatic sac and duct continue growing until age 3–4 years
II. EXTERNAL EAR (Auricle + External Auditory Canal)
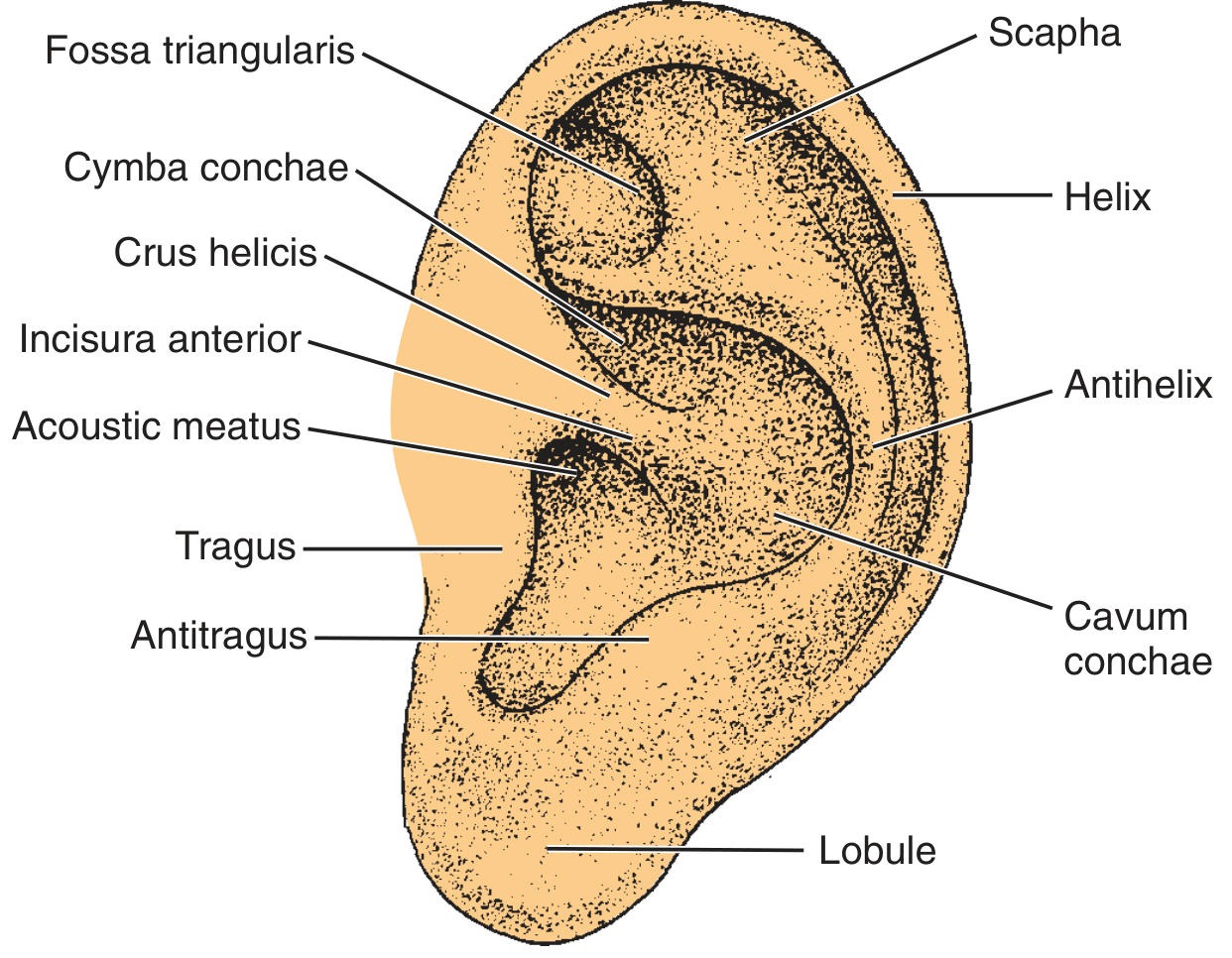
Auricle (Pinna)
The auricle is a funnel-shaped cartilaginous structure of elastic cartilage covered by keratinizing squamous epithelium. Its surface landmarks include:
| Structure | Description |
|---|---|
| Helix | Outer curved rim |
| Antihelix | Inner Y-shaped ridge; encloses the triangular fossa |
| Scapha | Groove between helix and antihelix |
| Tragus | Anterior cartilaginous projection |
| Antitragus | Opposite the tragus; separated from it by the intertragal notch |
| Concha | Deep central bowl (cymba conchae superiorly, cavum conchae inferiorly) |
| Lobule | Cartilage-free fatty inferior portion |
Blood supply: Posterior auricular artery and superficial temporal artery (both from the external carotid artery).
Sensory innervation: Auriculotemporal branch of V3 (trigeminal), cutaneous branch of CN VII, and branches from C2–C3.
Clinical notes:
- The lateral perichondrium is tightly adherent; the medial is loose — relevant to hematoma and infection spread
- Sebaceous glands and hair follicles are in the subcutaneous layer; adipose tissue is restricted to the lobule
External Auditory Canal (EAC)
- Length: ~2.5 cm in adults
- Lateral 1/3: cartilaginous — contains sebaceous glands, apocrine (ceruminous) glands, and hair follicles beneath squamous epithelium
- Medial 2/3: bony — lined by thin immobile skin with no glands; continuous with the tympanic membrane epithelium
- Isthmus: the bony-cartilaginous junction; the narrowest point of the canal
- Cerumen (earwax): produced from glandular secretions and sloughed epithelium; hydrophobic, slightly acidic (pH 6.0–6.5), protective
- Self-cleansing mechanism: Keratinous layers of the TM migrate centrifugally toward the cartilaginous canal where cerumen is extruded
- Fissures of Santorini: natural defects in the cartilaginous EAC — provide pathways for infection/tumor spread to the parotid gland
- Foramen of Huschke: incomplete ossification of the anterior bony canal — allows spread to the deep parotid lobe
III. TYMPANIC MEMBRANE
The tympanic membrane (TM) forms the medial wall of the EAC and the lateral wall of the middle ear.
Structure:
- Four layers: lateral squamous epithelium (EAC skin), outer radiate fibrous layer, inner circular fibrous layer, medial mucosal layer
- Attached centrally to the manubrium of the malleus at the umbo; peripherally anchored by the annular ligament in the tympanic sulcus
Two regions:
- Pars tensa (inferior, thicker): supported by both fibrous layers; most of the TM
- Pars flaccida / Shrapnell membrane (superior, thinner): lacks the fibrous layer; attached superiorly to the notch of Rivinus; clinical importance in cholesteatoma formation
Otoscopic landmarks: Manubrium/mallear stria (7 o'clock or 5 o'clock position), umbo, lateral process, anterior and posterior mallear folds, light reflex (cone of light), long process of incus, promontory, and round window visible through the translucent TM.
IV. MIDDLE EAR (Tympanic Cavity)
The middle ear is an air-filled space formed by expansion of the first pharyngeal pouch. It communicates anteriorly with the nasopharynx via the Eustachian tube and posteriorly with the mastoid antrum and air cells.
Compartments
- Epitympanum (attic): above the mallear folds; contains the head of the malleus and body/short process of the incus
- Mesotympanum: the main chamber; contains most of the ossicular chain
- Hypotympanum: floor of the middle ear; lies near the jugular bulb
Ossicular Chain
The three ossicles transmit vibrations from the TM to the oval window, providing a mechanical impedance-matching system between air (EAC) and fluid (perilymph of the inner ear):
| Ossicle | Features |
|---|---|
| Malleus | Handle (manubrium) embedded in TM; head articulates with the incus |
| Incus | Body and long process; articulates with the stapes via the lenticular process |
| Stapes | Footplate sits in the oval window; smallest bone in the body |
Clinical note: The long process of the incus is the most vulnerable ossicle — it has a single nutrient vessel without collateral circulation and is commonly destroyed in chronic otitis media.
Impedance matching mechanics:
- The lever effect of the ossicular chain provides a ~1.3× mechanical advantage
- The area ratio of TM to stapes footplate (~17:1) provides the primary pressure amplification
- Combined effect: ~25–30 dB amplification of sound pressure at the oval window
Key Structures
- Eustachian tube: equalizes middle ear pressure; opens with swallowing/yawning; normally closed in adults; shorter, more horizontal in children (predisposing to otitis media)
- Round window: covered by the secondary tympanic membrane; allows fluid displacement within the cochlea
- Stapedius muscle: attached to the stapes, innervated by CN VII; the acoustic reflex (contraction in response to loud sounds) reduces transmission of low-frequency sound and protects the inner ear
- Tensor tympani: attached to the malleus, innervated by V3; tenses the TM
- Chorda tympani: branch of CN VII passing through the middle ear; carries taste from the anterior 2/3 of the tongue and secretomotor fibers to the submandibular gland
Facial Nerve in the Middle Ear
The facial nerve traverses the temporal bone in the fallopian canal with four segments and two genu:
- Labyrinthine segment (most narrow; watershed vascular supply — most vulnerable to Bell's palsy/herpes zoster)
- Geniculate ganglion (gives off greater superficial petrosal nerve → lacrimal gland)
- Tympanic (horizontal) segment: courses over the cochleariform process → superior to oval window
- Mastoid (vertical) segment: descends to the stylomastoid foramen
V. INNER EAR
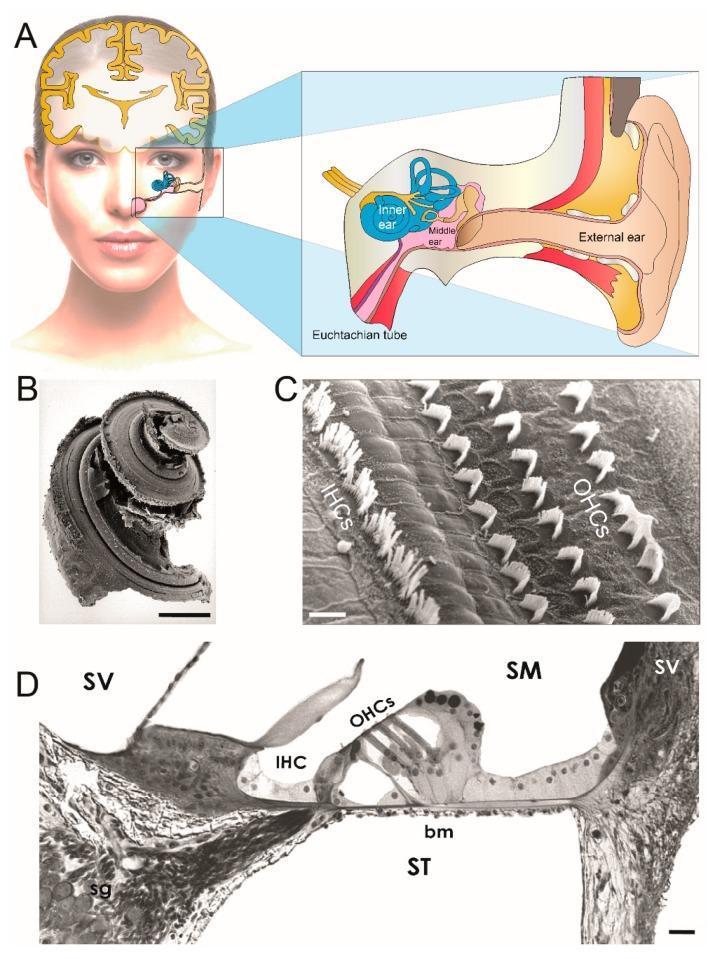
The inner ear is housed within the otic capsule (petrous temporal bone) and consists of:
- Bony labyrinth: spaces within the petrous bone, filled with perilymph (Na⁺-rich, similar to extracellular fluid)
- Membranous labyrinth: enclosed within the bony labyrinth, filled with endolymph (K⁺-rich, ~150 mEq/L K⁺, maintained by the stria vascularis — analogous to intracellular fluid)
Cochlea (Auditory Organ)
The cochlea makes 2.5 turns around the central bony modiolus and contains three fluid-filled chambers:
| Compartment | Contents | Communication |
|---|---|---|
| Scala vestibuli | Perilymph | Continuous with scala tympani at the helicotrema (apex) |
| Scala media (cochlear duct) | Endolymph | Separated from vestibuli by Reissner's membrane; from tympani by basilar membrane |
| Scala tympani | Perilymph | Ends at the round window membrane |
Organ of Corti (on the basilar membrane):
- Inner hair cells (IHCs): ~3,500; arranged in a single row; the primary auditory transducers (responsible for >95% of afferent nerve input)
- Outer hair cells (OHCs): ~12,000; arranged in 3–4 rows; electromotile — amplify and tune basilar membrane motion (electromotility powered by prestin protein)
- Stereocilia project from hair cell apices into the tectorial membrane
- Tip links connect stereocilia; deflection opens mechanosensitive K⁺/Ca²⁺ channels
- Spiral ganglion: bipolar neurons whose peripheral processes contact hair cells and central axons form the cochlear nerve (CN VIII)
VI. PHYSIOLOGY OF THE AUDITORY ANALYZER
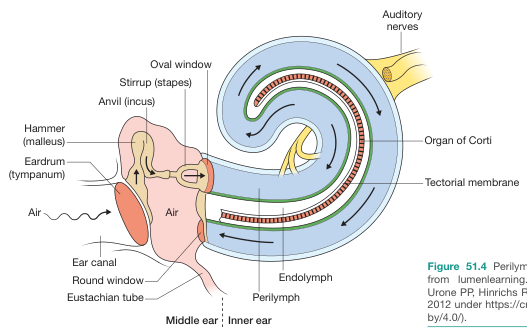
Mechanoelectrical Transduction
- Sound waves enter the EAC → vibrate the TM → mechanical vibration transmitted via ossicular chain → stapes footplate compresses oval window
- Fluid wave travels through scala vestibuli → displaces the basilar membrane → returns through scala tympani → dissipates at the round window
- The basilar membrane exhibits tonotopic organization:
- Base (narrow, stiff): responds to high frequencies (up to ~20,000 Hz)
- Apex (wide, flexible): responds to low frequencies (~20 Hz)
- Basilar membrane displacement causes shearing of stereocilia against the tectorial membrane → deflection opens mechano-gated ion channels → K⁺ influx (from endolymph) → receptor potential
- IHC depolarization → glutamate release → activation of spiral ganglion afferents → action potentials along the cochlear nerve
Endocochlear Potential
- The stria vascularis generates a +80 mV endocochlear potential (endolymph positive relative to perilymph)
- This provides the electrochemical driving force for K⁺ influx into hair cells
- Disruption (e.g., by connexin-26/GJB2 mutations that impair K⁺ recycling) causes sensorineural hearing loss
Auditory Central Pathway
Cochlear nerve → cochlear nuclei (medulla) → superior olivary complex (where binaural inputs converge for sound localization) → lateral lemniscus → inferior colliculus (midbrain) → medial geniculate nucleus (thalamus) → primary auditory cortex (Heschl's gyri, superior temporal plane, Brodmann areas 41–42)
VII. VESTIBULAR SYSTEM

Anatomy
Five end organs of the vestibular system:
- Three semicircular canals (SCCs): detect angular acceleration
- Utricle: detects linear acceleration (horizontal plane) and head tilt
- Saccule: detects linear acceleration (vertical/sagittal plane)
Semicircular canals are oriented roughly orthogonally in three planes:
- Superior (anterior) SCC: detects head pitch (sagittal plane)
- Posterior SCC: detects head roll
- Lateral (horizontal) SCC: detects head yaw
Each SCC dilates at one end into an ampulla, which contains the crista ampullaris — a sensory ridge covered by hair cells embedded in a gelatinous cupula that spans the full ampullary cross-section.
Otolith Organs (Utricle and Saccule)
- Both contain a macula: a flat sensory epithelium with hair cells covered by the otolithic membrane (gelatinous layer embedded with calcium carbonate crystals — otoconia/otoliths)
- Gravity and linear acceleration displace the otolithic membrane relative to the hair cells, deflecting stereocilia
Transduction Mechanism
- Hair cells have a tall kinocilium and stepwise stereocilia bundle
- Deflection toward the kinocilium → depolarization (increased firing)
- Deflection away → hyperpolarization (decreased firing)
- Hair cells release glutamate onto afferent fibers of the superior and inferior vestibular nerves (branches of CN VIII), which synapse in the vestibular nuclei (medulla/pons) and the cerebellum
Central Vestibular Pathway
Vestibular nerve → vestibular nuclei (4 nuclei: superior, inferior, medial, lateral/Deiters) →
- Vestibulospinal tracts (medial and lateral) → postural reflexes
- Medial longitudinal fasciculus (MLF) → eye movement coordination (vestibulo-ocular reflex, VOR)
- Cerebellum (flocculus, nodulus) → calibration and adaptation
- Thalamus → PIVC (parieto-insular vestibular cortex) → conscious spatial orientation
VIII. RESEARCH METHODS OF THE AUDITORY ANALYZER
A. Subjective (Behavioral) Tests
| Test | Principle | Use |
|---|---|---|
| Pure-tone audiometry (PTA) | Patient responds to tones at different frequencies (250–8000 Hz) and intensities via air conduction (AC) and bone conduction (BC) | Gold standard for threshold determination; differentiates conductive vs. sensorineural hearing loss (air-bone gap) |
| Speech audiometry | Speech recognition threshold (SRT) and word recognition score (WRS) | Assesses functional hearing; detects retrocochlear pathology |
| Weber test | Tuning fork on vertex; lateralization to the affected ear = conductive loss; to the better ear = sensorineural loss | Bedside screening |
| Rinne test | AC vs. BC comparison at the ear; negative (BC > AC) = conductive loss | Bedside screening |
B. Objective (Physiological) Tests
| Test | Principle | Clinical Use |
|---|---|---|
| Tympanometry | Measures TM compliance as ear canal pressure is varied; generates a tympanogram | Middle ear effusion (type B), Eustachian tube dysfunction, ossicular fixation or discontinuity |
| Acoustic reflex testing | Stapedius muscle contraction to loud sound (~70–90 dB above threshold); detected by tympanometer | CN VII integrity, retrocochlear lesions |
| Otoacoustic emissions (OAEs) | Low-intensity sounds generated by OHC electromotility; detected in the EAC — TEOAEs (transient evoked) and DPOAEs (distortion product) | Universal neonatal hearing screening; cochlear function; cannot detect auditory neuropathy alone |
| Auditory Brainstem Response (ABR/BERA) | Electroencephalographic recording of neural responses (Waves I–V) to click stimuli — generated from cochlear nerve (I), cochlear nuclei (II), superior olive (III), lateral lemniscus (IV), inferior colliculus (V) | Threshold estimation in infants; retrocochlear (VIII nerve/brainstem) pathology; intraoperative monitoring |
| Auditory Steady-State Response (ASSR) | Frequency-specific continuous stimuli; automated threshold detection | Frequency-specific thresholds in infants who cannot cooperate with ABR |
| Electrocochleography (ECochG) | Measures cochlear potentials (summating potential, action potential) close to the cochlea | Menière's disease (elevated SP:AP ratio); cochlear hydrops |
C. Imaging
- CT temporal bone (high-resolution): bony anatomy of EAC, ossicles, mastoid; cholesteatoma assessment; canal atresia
- MRI with gadolinium: soft tissue detail — internal auditory canal (IAC) nerve anatomy, endolymphatic sac, acoustic neuroma, cochlear duct patency, endolymphatic hydrops
IX. RESEARCH METHODS OF THE VESTIBULAR ANALYZER
| Test | Principle | Clinical Use |
|---|---|---|
| Caloric testing (Hallpike-FitzGerald) | Warm (44°C) and cold (30°C) water/air irrigation of the EAC induces convection currents in the lateral SCC endolymph → nystagmus; COWS rule: Cold Opposite, Warm Same | Unilateral vestibular hypofunction; canal paresis quantification |
| Video Head Impulse Test (vHIT) | High-velocity, small-amplitude head impulses in the plane of each SCC; video capture of eye movements; pathological = corrective saccades (covert or overt) after the impulse | Individual SCC function; superior to caloric for detecting high-frequency canal paresis |
| Videonystagmography / Electronystagmography (VNG/ENG) | Records eye movements during gaze, positional, and caloric tests using infrared goggles or electrodes | Comprehensive peripheral and central vestibular testing |
| Dix-Hallpike maneuver | Rapid supine positioning with head rotated 45° to one side; positive = delayed geotropic rotatory nystagmus | Diagnosis of posterior SCC BPPV |
| Vestibular Evoked Myogenic Potentials (VEMPs) | Cervical VEMP (cVEMP): saccule → inferior vestibular nerve → sternocleidomastoid; Ocular VEMP (oVEMP): utricle → superior vestibular nerve → contralateral inferior oblique | Saccular and utricular function; superior canal dehiscence; vestibular neuritis |
| Rotational chair testing | Patient rotated sinusoidally in darkness; VOR gain, phase, and symmetry measured | Bilateral vestibular hypofunction; cannot be assessed by caloric alone |
| Posturography (Computerized Dynamic Posturography) | Measures postural sway on a moving platform under various visual/proprioceptive conditions | Balance rehabilitation; sensory organization |
| MRI (gadolinium-enhanced) | 3D-FLAIR and T2-SPAIR sequences 4 hours after IV gadolinium injection; endolymph (bright) vs. perilymph (dark) | Endolymphatic hydrops grading in Menière's disease |
Summary
The ear is a tripartite organ with highly specialized functions:
- The outer ear collects and directs sound; the EAC's anatomy — including cerumen, narrow isthmus, and epithelial migration — provides both acoustic function and a self-protecting microenvironment
- The middle ear transforms low-impedance airborne vibrations into high-impedance fluid waves, amplifying pressure ~25–30 dB through the TM:footplate area ratio and ossicular lever mechanism
- The cochlea performs frequency analysis (tonotopy) and mechanoelectrical transduction through the organ of Corti; the stria vascularis-maintained endocochlear potential (+80 mV) drives K⁺ influx and is essential for hair cell function
- The vestibular apparatus encodes rotational motion (SCCs via crista ampullaris/cupula) and linear acceleration/gravity (utricle and saccule via otolith organs), forming the sensory basis for the VOR, postural reflexes, and spatial orientation
- Clinical investigation uses a layered approach: bedside tuning fork tests → audiometry → tympanometry/OAEs/ABR for the auditory system; caloric, vHIT, VEMPs, and rotational testing for the vestibular system; advanced imaging (CT + MRI) for structural pathology
Sources:
- Cummings Otolaryngology Head and Neck Surgery, Chapter 126 (Anatomy of the Temporal Bone, External Ear, and Middle Ear)
- K.J. Lee's Essential Otolaryngology, Inner Ear (Cochlea, Vestibule, IAC)
- Miller's Anesthesia 10e, Synopsis of Ear, Nose, and Throat Anatomy
- Bailey and Love's Short Practice of Surgery 28e
This is a shared conversation. Sign in to Orris to start your own chat.