Clinical anatomy of the ear. Physiology and research methods of auditory and vestibular analyzers
Reading File
Finding Sources
Finding Sources
Searching Images
anatomy of the ear cochlea vestibular system diagram
Finding Sources
Searching Images
auditory pathway brainstem cochlear nerve hearing physiology
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compile a thorough, well-structured response.
Clinical Anatomy of the Ear: Physiology and Research Methods of Auditory and Vestibular Analyzers
I. OVERVIEW
The ear is both the organ of hearing and of balance. It is anatomically divided into three parts: the external ear, middle ear, and internal ear. These three divisions serve as a linked mechanical-to-neural transduction chain.
"The ear is the organ of hearing and balance. It has three parts... The internal ear converts the mechanical signals received from the middle ear, which start as sound captured by the external ear, into electrical signals to transfer information to the brain. The internal ear also contains receptors that detect motion and position." — Gray's Anatomy for Students
II. EXTERNAL EAR
Auricle (Pinna)
The auricle projects from the side of the head and collects sound. Its cartilaginous skeleton is organized into:
- Helix — the outer rim, ending inferiorly at the fleshy lobule (the only part without cartilage)
- Antihelix — a curved parallel rim anterior to the helix
- Concha — the hollow center from which the external acoustic meatus opens
- Tragus / Antitragus — elevations flanking the meatus opening
Intrinsic muscles (small, between cartilages) and extrinsic muscles (anterior, superior, posterior auricular) — both groups innervated by the facial nerve [VII].
Innervation of auricle (from multiple sources):
| Surface | Nerve |
|---|---|
| Anterosuperior | Auriculotemporal nerve (V3) |
| Anterior/posterior inferior | Great auricular nerve (cervical plexus) |
| Posterosuperior | Lesser occipital nerve |
| Deeper surfaces | Auricular branch of vagus [X] and facial nerve [VII] |
Vasculature: External carotid → posterior auricular artery (posterior); superficial temporal artery (anterior). Lymphatics drain anteriorly into parotid nodes, posteriorly into mastoid nodes.
External Acoustic Meatus
Extends ~2.5 cm from the concha to the tympanic membrane. The lateral one-third is cartilaginous; the medial two-thirds is a bony canal in the temporal bone. The canal follows an S-shaped course: upward-anteriorly → slightly posteriorly → anteriorly-downward. To examine the tympanic membrane, pull the auricle superiorly, posteriorly, and slightly laterally. Skin lining contains hair follicles and ceruminous glands (modified sweat glands producing earwax).
Innervation: Auriculotemporal nerve [V3] (anterior and superior walls); auricular branch of vagus [X] (posterior and inferior walls).
Tympanic Membrane (Eardrum)
Separates the external meatus from the middle ear. Tilted medially — its lateral surface faces inferiorly and anteriorly. Divided into:
- Pars tensa — the main functional part, taut
- Pars flaccida (Shrapnell's membrane) — the smaller superior region, loosely attached
The handle of the malleus is embedded in the tympanic membrane. The chorda tympani nerve runs in the upper one-third; therefore surgical incisions on the membrane are always made below this level, in the posteroinferior quadrant (which also has richer blood supply).
Clinical note: Perforation may result from trauma or otitis media. While many ruptures heal spontaneously, large ones require myringoplasty. Chronic otitis media can damage the ossicular chain and cause deafness.
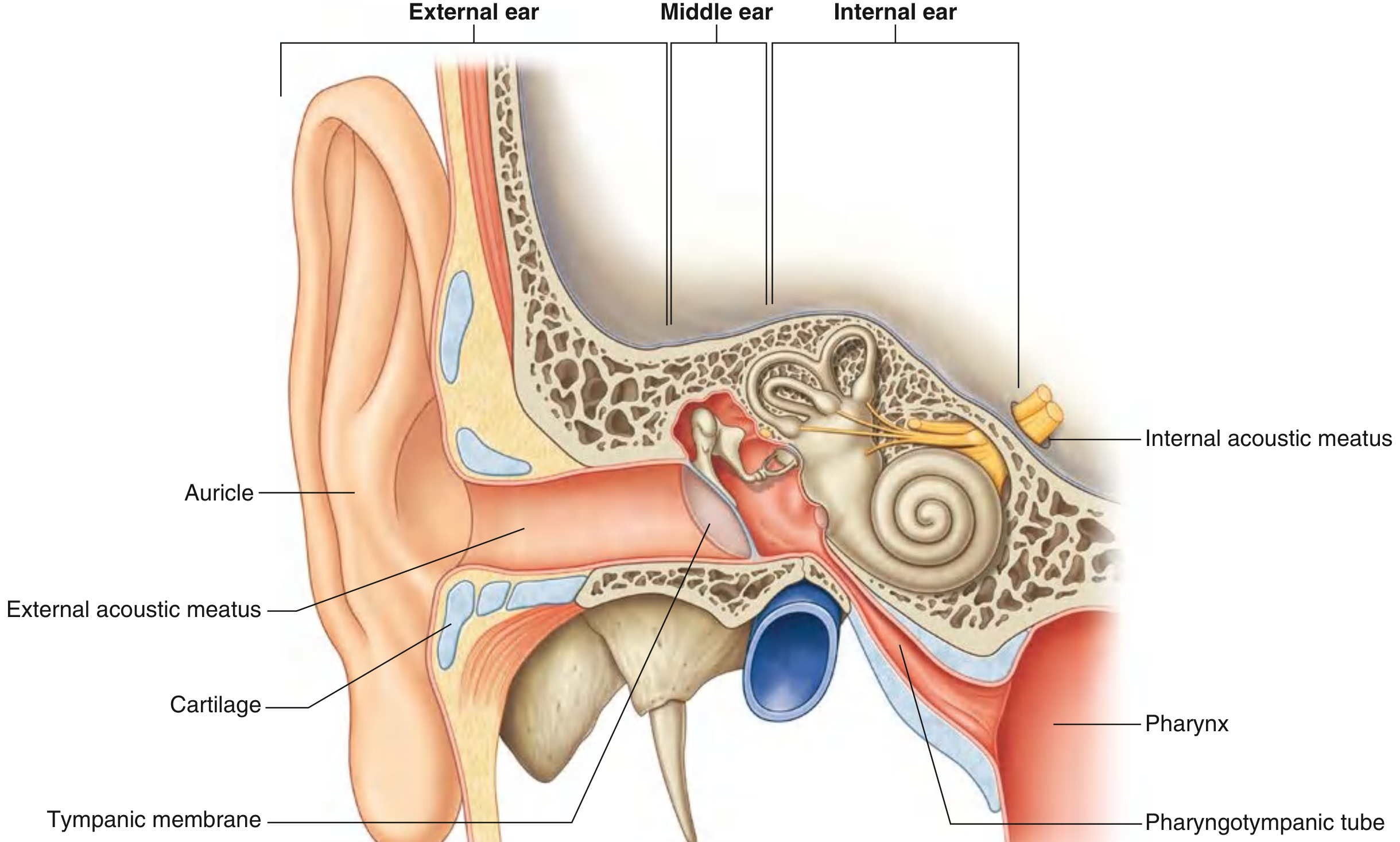
III. MIDDLE EAR
The middle ear is an air-filled, mucous-membrane-lined space in the petrous temporal bone between the tympanic membrane laterally and the internal ear medially. It consists of:
- Tympanic cavity proper — adjacent to the tympanic membrane
- Epitympanic recess — the superior extension housing the malleus head and incus body
It communicates anteriorly with the nasopharynx via the pharyngotympanic (Eustachian) tube, and posteriorly with the mastoid air cells via the aditus to the mastoid antrum.
Walls of the Middle Ear
| Wall | Key Structure |
|---|---|
| Tegmental (roof) | Tegmen tympani — thin bone separating the middle ear from the middle cranial fossa |
| Jugular (floor) | Thin bone over the jugular bulb |
| Labyrinthine (medial) | Promontory (basal cochlear coil bulge); oval window (stapes footplate); round window; prominence of facial canal; prominence of lateral semicircular canal |
| Mastoid (posterior) | Pyramidal eminence (stapedius tendon); chorda tympani entry point |
| Anterior | Pharyngotympanic tube opening; tensor tympani canal; internal carotid artery |
Tympanic plexus (on the promontory): formed by the tympanic branch of CN IX and sympathetic branches from the internal carotid plexus. Supplies mucosa of middle ear, mastoid, and pharyngotympanic tube. Gives rise to the lesser petrosal nerve → otic ganglion → parotid gland (parasympathetic secretomotor).
Auditory Ossicles
Three tiny bones transmit vibrations from the tympanic membrane to the oval window:
- Malleus ("hammer") — largest; handle embedded in tympanic membrane; head articulates with incus in epitympanic recess; anterior process anchored to anterior wall by ligament.
- Incus ("anvil") — body articulates with malleus head; long limb descends and articulates with stapes; short limb attaches posteriorly by ligament.
- Stapes ("stirrup") — smallest bone in the body; head articulates with incus long process; footplate fits into the oval window.
Muscles of the Ossicles
| Muscle | Attachment | Innervation | Action |
|---|---|---|---|
| Tensor tympani | Handle of malleus | Mandibular nerve [V3] via medial pterygoid nerve | Pulls malleus medially, tenses tympanic membrane, dampens vibrations from loud sounds |
| Stapedius | Neck of stapes | Facial nerve [VII] | Pulls stapes posteriorly, reduces oscillation amplitude (acoustic reflex) |
The acoustic reflex (stapedius contraction in response to loud noise, >80 dB) protects the inner ear. It is tested clinically by tympanometry.
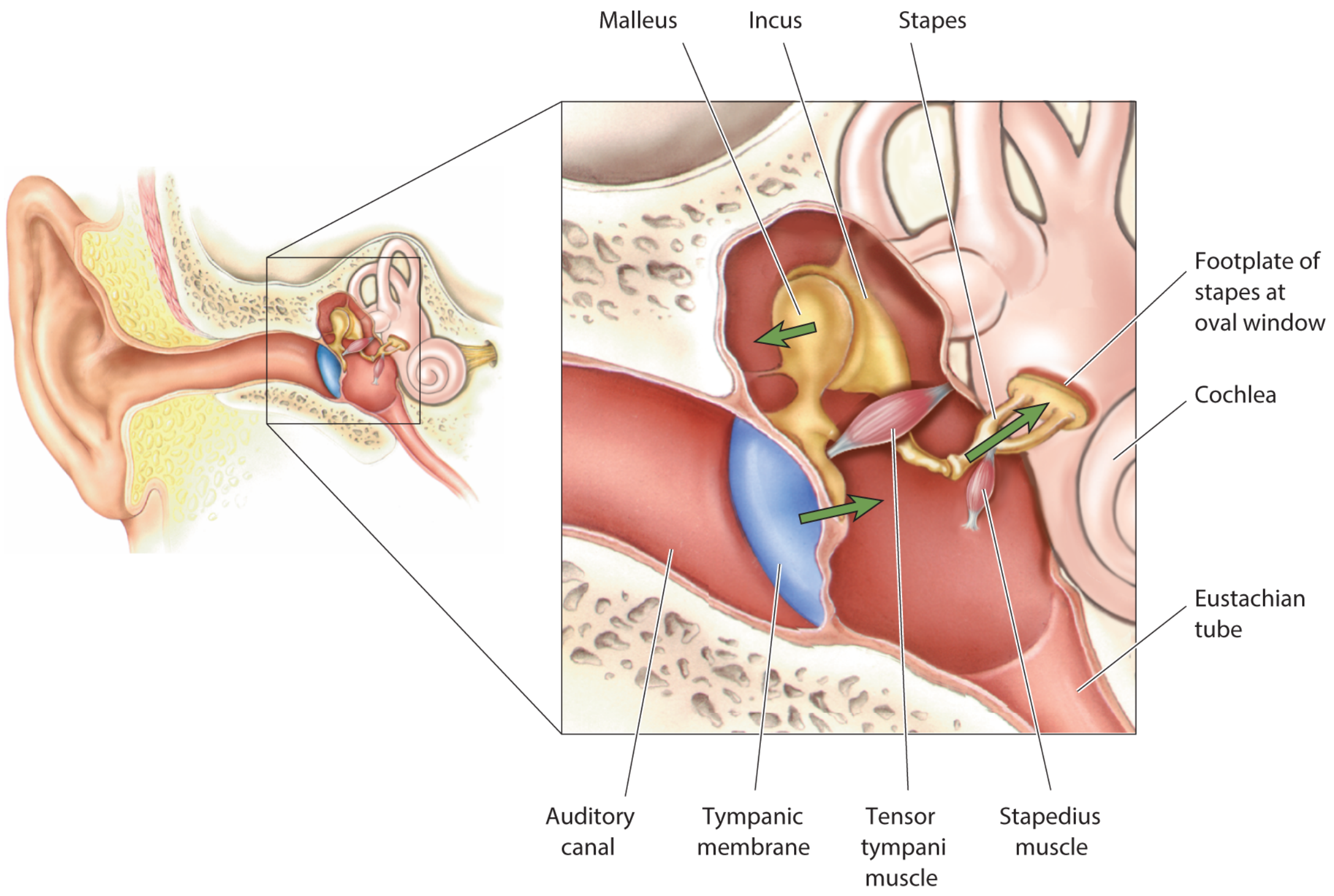
Sound Force Amplification
The middle ear overcomes the impedance mismatch between air and fluid. It does this by:
- Area advantage: The tympanic membrane (~55 mm²) is ~17× larger than the oval window (~3.2 mm²), concentrating pressure.
- Lever action: The ossicular lever ratio provides ~1.3× mechanical advantage.
- Combined: ~22-fold pressure amplification, equivalent to ~25 dB.
IV. INTERNAL (INNER) EAR
Located in the petrous temporal bone, between the middle ear laterally and the internal acoustic meatus medially. Contains two labyrinths:
A. Bony Labyrinth
Three communicating cavities filled with perilymph (similar to CSF, high Na⁺):
- Vestibule — central region; oval window on lateral wall; communicates with cochlea anteriorly, semicircular canals posterosuperiorly
- Three semicircular canals — anterior, posterior, lateral; each dilates at one end into an ampulla
- Cochlea — spiral structure of 2.5–2.75 turns around a central bony core (modiolus); divided by the cochlear duct into scala vestibuli (above) and scala tympani (below); these communicate at the apex through the helicotrema
B. Membranous Labyrinth
Suspended within the perilymph, filled with endolymph (high K⁺, ~150 mM; strongly positive potential of +80 mV — the endocochlear potential):
- Cochlear duct (scala media) — organ of hearing
- Utricle and saccule — linear acceleration sensors
- Three semicircular ducts — rotational acceleration sensors
The utriculosaccular duct connects the sacs. The endolymphatic duct passes through the vestibular aqueduct to expand into the endolymphatic sac on the posterior surface of the petrous temporal bone, where it reabsorbs endolymph.
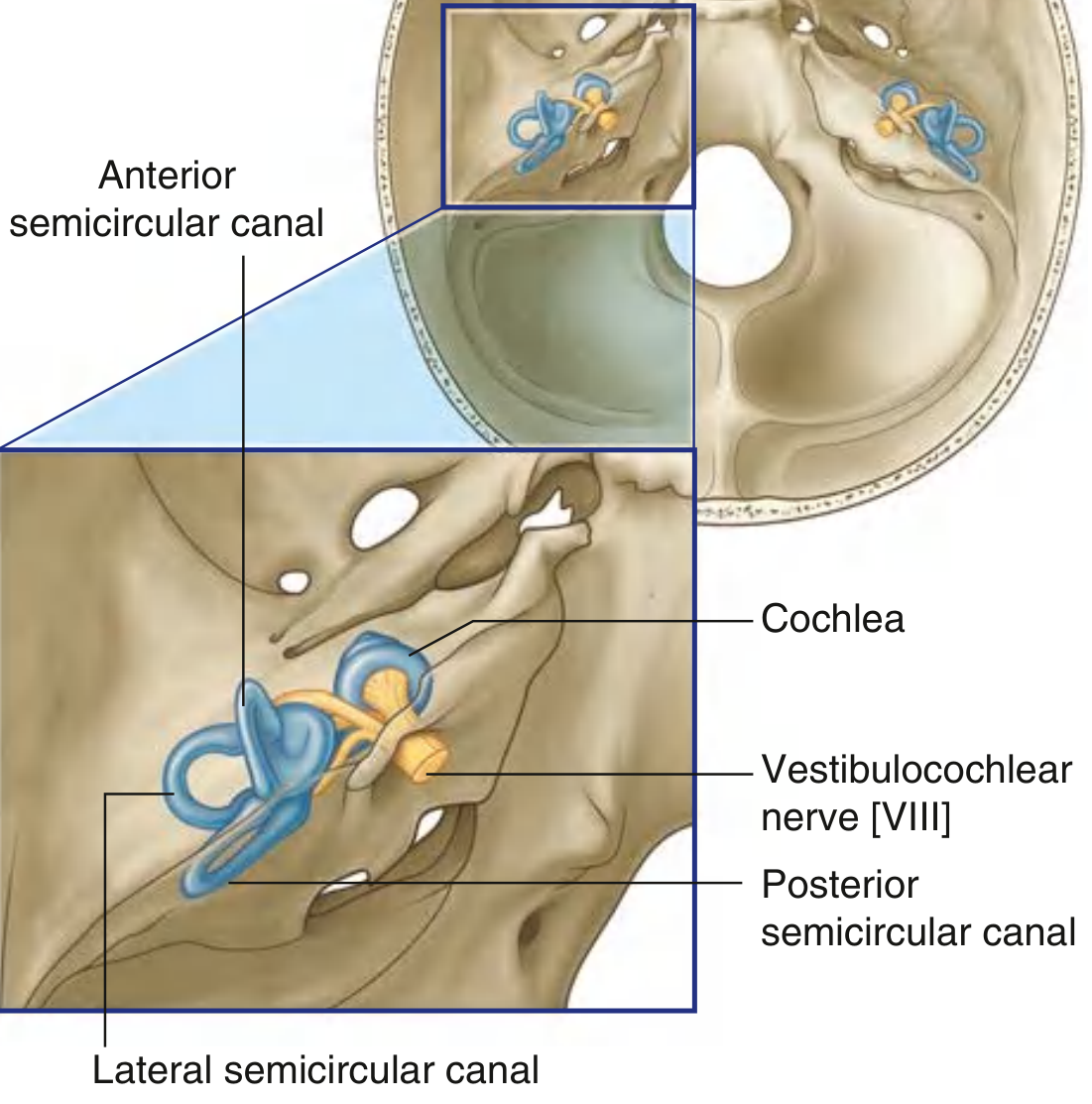

Vestibulocochlear Nerve [CN VIII]
Enters the internal acoustic meatus and divides into:
- Cochlear nerve — from spiral ganglion (hearing)
- Vestibular nerve — from vestibular ganglion (balance); carries superior and inferior divisions
V. PHYSIOLOGY OF THE AUDITORY ANALYZER
Nature of Sound
Sounds are periodic variations in air pressure traveling at ~343 m/s. Characterized by:
- Frequency (Hz) — perceived as pitch; human range 20–20,000 Hz
- Amplitude — perceived as loudness, measured in decibels (dB SPL)
Cochlear Mechanics — Basilar Membrane & Tonotopy
The basilar membrane is narrow and stiff at the base (responds to high frequencies), and wide and flaccid at the apex (responds to low frequencies). Sound entering through the oval window sets up a traveling wave that peaks at a frequency-specific location:
- High frequencies → peak near the base
- Low frequencies → wave travels to the apex
This tonotopic (place) coding is the fundamental mechanism of pitch discrimination, preserved all the way to the auditory cortex.
Organ of Corti — Transduction
Sitting on the basilar membrane, the organ of Corti contains:
- Inner hair cells (IHC) — 1 row (~3,500 cells); primary sensory receptors; receive ~95% of spiral ganglion afferents
- Outer hair cells (OHC) — 3 rows (~12,000 cells); amplify basilar membrane movement via electromotility (somatic motor driven by prestin protein)
- Tectorial membrane — gelatinous membrane above the hair cells; stereocilia of OHCs are embedded in it
Each hair cell has 50–150 stereocilia arranged in a staircase pattern. Tip links connect adjacent stereocilia. When the basilar membrane flexes, stereocilia bend toward the tallest row → tip links pull open TMC mechanotransduction channels → K⁺ (and Ca²⁺) enters from endolymph → hair cell depolarizes.
The mechanism is unusual: opening K⁺ channels depolarizes rather than hyperpolarizes, because endolymph has extremely high K⁺ (~150 mM) and the endocochlear potential (+80 mV) creates a ~120 mV driving force across the stereociliary membrane. When transduction channels open, K⁺ rushes in along the voltage gradient.
Depolarization → voltage-gated Ca²⁺ channels open at the basolateral membrane → glutamate released onto spiral ganglion dendrites → action potentials generated.
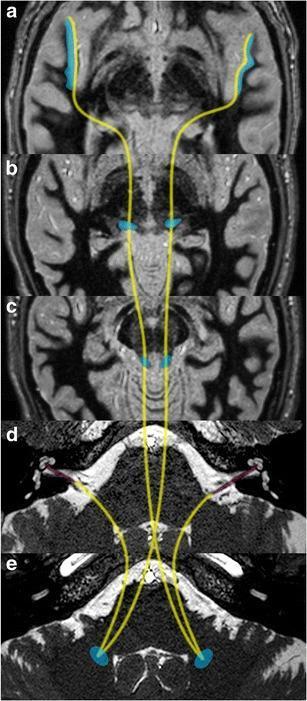
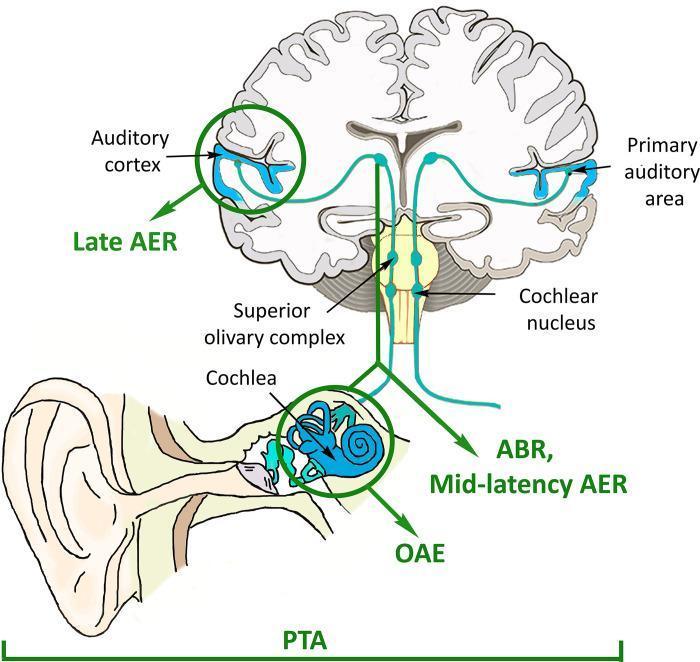
Central Auditory Pathway
The auditory pathway from cochlea to cortex:
Cochlea (spiral ganglion)
↓ CN VIII (cochlear nerve)
Cochlear nuclei (dorsal & ventral — brainstem)
↓ decussates via trapezoid body
Superior olivary complex (first binaural integration; sound localization)
↓
Lateral lemniscus
↓
Inferior colliculus (midbrain; reflex coordination)
↓
Medial geniculate nucleus (MGN, thalamus)
↓
Primary auditory cortex — A1 (Heschl's gyrus, superior temporal gyrus)
Each auditory neuron has a characteristic frequency — it responds maximally to one frequency and decreasingly to others. This tuning property is maintained at all levels of the pathway.
Encoding Sound Intensity and Frequency
- Intensity: encoded by firing rate of spiral ganglion neurons and the number of neurons recruited
- Frequency: encoded by (1) place code (tonotopy on basilar membrane) and (2) phase-locking (neurons fire at specific phases of the sound wave, useful below ~4,000 Hz)
Sound Localization
| Mechanism | Frequency Range | Cue |
|---|---|---|
| Interaural time difference (ITD) | <1,500 Hz | Sound phase/arrival time difference between ears; processed in medial superior olive |
| Interaural intensity difference (IID) | >2,000 Hz | Head acts as a sound shadow; processed in lateral superior olive |
VI. PHYSIOLOGY OF THE VESTIBULAR ANALYZER
Sensory Organs
A. Otolith organs — static and linear acceleration
- Macula of utricle: detects linear acceleration in the horizontal plane and sideways head tilts; hair cells embedded in a gelatinous membrane loaded with calcium carbonate crystals (otoliths/otoconia)
- Macula of saccule: detects linear acceleration in the vertical plane (forward-backward, up-down)
When the head tilts or accelerates, inertia causes the otolith membrane to lag behind, deflecting the hair cell cilia. The striola (a curvilinear dividing line) reverses hair cell polarity across each macula, enabling bidirectional sensitivity.
B. Semicircular canals — angular/rotational acceleration
- Three canals oriented in nearly orthogonal planes: lateral (horizontal), anterior (superior), and posterior
- At each ampulla, the crista ampullaris houses hair cells capped by the gelatinous cupula, which spans the full width of the ampulla
- Angular acceleration of the head causes endolymph to lag due to inertia → pushes or pulls the cupula → deflects hair cell cilia
- The lateral canal of one side works in push-pull with the opposite lateral canal: rightward head rotation excites the right horizontal canal hair cells and inhibits the left
Vestibulo-Ocular Reflex (VOR)
The VOR stabilizes images on the retina during head movement. Head rotation → vestibular nuclei → eye muscles move in the opposite direction to head movement at the same velocity. This reflex is so fast (~10 ms latency) that it outpaces visual feedback.
During sustained rotation, alternating slow compensatory eye movements and fast resets produce nystagmus, named by the direction of the fast phase.
Vestibulospinal Reflexes
Vestibular nuclei project to spinal cord via medial and lateral vestibulospinal tracts, adjusting postural muscle tone in response to head position.
Vestibular Cortex
Vestibular signals ultimately reach the parieto-insular cortex (primary vestibular cortex), hippocampus (spatial navigation), and prefrontal cortex. Unlike hearing, vestibular sensation rarely reaches consciousness under normal circumstances.
VII. RESEARCH METHODS
A. Audiological Methods
| Test | Principle | What It Assesses |
|---|---|---|
| Pure-tone audiometry (PTA) | Patient responds to tones at standardized frequencies (250–8000 Hz) presented via headphones or bone conductor | Air-conduction and bone-conduction thresholds; identifies conductive vs. sensorineural hearing loss |
| Speech audiometry | Speech recognition threshold and word discrimination score | Central auditory processing and cochlear function |
| Tympanometry | Measures compliance of tympanic membrane as air pressure is varied in sealed ear canal | Middle ear pressure, effusion, ossicular chain integrity, acoustic reflex (stapedius) |
| Otoacoustic emissions (OAEs) | Microphone in ear canal detects sounds generated by OHC electromotility | OHC function; used in neonatal screening; present with normal cochlear function up to ~30 dB HL |
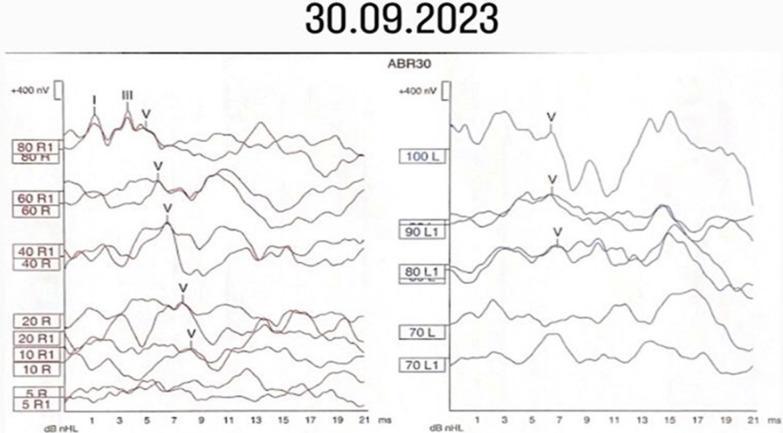
| Auditory brainstem response (ABR/BAEP) | Click stimulus → surface electrodes record waves I–V corresponding to CN VIII, cochlear nuclei, superior olive, lateral lemniscus, inferior colliculus | Threshold estimation, neural conduction timing, retrocochlear pathology (acoustic neuroma); identifies wave V at threshold |
| Electrocochleography (ECoG) | Near-field recording from cochlear promontory or TM electrode | Summating potential (SP) and action potential (AP); elevated SP/AP ratio in Menière's disease |
B. Vestibular Methods
| Test | Principle | What It Assesses |
|---|---|---|
| Caloric test | Warm (40°C) or cold (30°C) water or air introduced into the external ear canal; convective endolymph currents mimic head rotation | Lateral semicircular canal function; compares each ear separately; absent response = ipsilateral vestibular hypofunction |
| Rotatory chair test | Patient rotated in sinusoidal or velocity steps while eye movements (VOR) are recorded | Bilateral vestibular function; gain, phase, and symmetry of VOR |
| Video head impulse test (vHIT) | High-velocity brief head rotations; high-speed camera records eye movements | VOR gain for all six semicircular canals; detects "corrective saccades" with canal paresis |
| Vestibular evoked myogenic potentials (VEMPs) | Loud clicks or tone bursts stimulate the ear; EMG recorded from SCM muscle (cVEMP) or periocular muscles (oVEMP) | cVEMP tests saccule and inferior vestibular nerve; oVEMP tests utricle and superior vestibular nerve |
| Posturography | Patient stands on a force platform; sensory conditions systematically manipulated | Sensory integration for balance (vision, proprioception, vestibular) |
| Electronystagmography / Videonystagmography (ENG/VNG) | Electrodes or infrared cameras record eye movements during caloric, positional, and gaze tests | Full oculomotor and vestibular battery |
| Dix-Hallpike test | Rapid positional head maneuver | Diagnosis of BPPV (posterior canal); positional geotropic nystagmus confirms otolith displacement |
C. Imaging
| Modality | Application |
|---|---|
| High-resolution CT of temporal bone | Bony anatomy; fractures; ossicular chain; cholesteatoma; cochlear implant planning |
| MRI with gadolinium | Soft tissue — acoustic neuroma (enhances on T1+contrast), endolymphatic hydrops (3D FIESTA/CISS sequences show membranous labyrinth), labyrinthitis |
| 3D FIESTA/CISS MRI | Delineates cochlea, semicircular canals, cochlear and vestibular nerves within the internal acoustic canal |
VIII. CLINICAL CORRELATES
| Condition | Anatomy/Mechanism | Key Feature |
|---|---|---|
| Otitis externa ("Swimmer's ear") | Infection of external acoustic meatus | Pain on tragus palpation |
| Otitis media | Middle ear infection; pharyngotympanic tube dysfunction | TM perforation, conductive hearing loss |
| Otosclerosis | Abnormal bone fixation of stapes footplate | Progressive conductive loss; Carhart notch on audiogram |
| Ménière's disease | Endolymphatic hydrops (excess endolymph) | Episodic vertigo, low-frequency SNHL, tinnitus, aural fullness; elevated SP/AP on ECoG |
| BPPV | Displaced otoconia in semicircular canal (usually posterior) | Brief positional vertigo; treated with Epley maneuver |
| Acoustic neuroma (vestibular schwannoma) | Tumor of Schwann cells on CN VIII (usually superior vestibular nerve) | Unilateral SNHL, tinnitus, abnormal ABR (prolonged I–V interval) |
| Nystagmus | Imbalance of vestibular nuclear activity | Evaluated by ENG/VNG; caloric test asymmetry |
Sources
- Gray's Anatomy for Students — External ear, middle ear, internal ear (pp. 1093–1106)
- Neuroscience: Exploring the Brain, 5th ed. — Auditory and vestibular system (pp. 1019–1090)
- Medical Physiology (Boron & Boulpaep) — Vestibular and auditory transduction; hair cells (pp. 551–552)
Clinical anatomy of the ear. Physiology and research methods of auditory and vestibular analyzers
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.