Questions asked in thyroid case presentation viva with answers for Ent post graduation exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from Cummings Otolaryngology — the definitive ENT reference. Let me compile the full viva Q&A.
Thyroid Case Presentation Viva — ENT Postgraduate Exam
A comprehensive Q&A covering anatomy, physiology, pathology, investigations, surgical management, and complications.
ANATOMY
Q1. What is the embryological origin of the thyroid gland?
The thyroid gland develops from an endodermal downgrowth from the floor of the primitive pharynx (foramen cecum at the base of the tongue) and descends along the thyroglossal duct to its final position in the neck. It is present in its final position by the 7th week of embryological development. The thyroglossal duct normally involutes, but remnants can give rise to thyroglossal cysts and fistulae.
Q2. Describe the anatomy of the thyroid gland.
- Lies within the anterior leaves of the middle layer of deep cervical fascia (visceral space), anterior and lateral to the thyroid cartilage, cricoid cartilage, and upper tracheal rings
- Consists of two lateral lobes connected by an isthmus at the level of the 2nd–4th tracheal rings
- A pyramidal lobe is often present (remnant of thyroglossal duct), ascending from the isthmus, more often to the left
- Weight: 20–30 g in adults
- — Cummings Otolaryngology Head and Neck Surgery
Q3. What is the blood supply to the thyroid gland?
- Superior thyroid artery (first branch of external carotid artery) — enters the superior pole
- Inferior thyroid artery (from thyrocervical trunk of subclavian artery) — enters posteriorly, closely related to the recurrent laryngeal nerve (RLN)
- Thyroid ima artery (present in ~3%) — from the aortic arch or brachiocephalic artery
- Venous drainage: superior and middle thyroid veins drain to the internal jugular vein; inferior thyroid veins drain to the brachiocephalic veins
Q4. What is Berry's ligament and why is it important?
Berry's ligament (posterior suspensory ligament) is the thickening of the pretracheal fascia that anchors the thyroid to the trachea and cricoid. The RLN often passes deep to or through this ligament — making this the most dangerous zone during thyroidectomy for RLN injury.
Q5. What is Zuckerkandl's tubercle?
Zuckerkandl's tubercle is a posterior extension of the thyroid lobe (the "posterior horn"). It is an important surgical landmark because the RLN lies in its groove, medial to the tubercle. Identifying it during thyroidectomy helps locate and protect the RLN.
Q6. What is the nerve supply relevant to thyroid surgery?
- Recurrent laryngeal nerve (RLN): motor to all intrinsic laryngeal muscles except cricothyroid; sensory below vocal cords. Injury causes ipsilateral vocal cord palsy.
- External branch of superior laryngeal nerve (EBSLN): motor to cricothyroid muscle (pitch, voice projection). Injury causes a weak, low-pitched voice — the "Amelita Galli-Curci" nerve.
- On the right, the RLN loops under the subclavian artery; on the left, it loops under the aortic arch — making the left RLN longer and at greater risk.
PHYSIOLOGY
Q7. How is thyroid hormone synthesised?
- Iodide trapping (NIS pump, TSH-stimulated)
- Oxidation of iodide to iodine (thyroid peroxidase)
- Organification — iodination of tyrosine residues on thyroglobulin → monoiodotyrosine (MIT) and diiodotyrosine (DIT)
- Coupling — MIT + DIT → T3; DIT + DIT → T4
- Secretion — proteolysis of thyroglobulin releases T3 and T4 into circulation
Q8. What are the transport proteins for thyroid hormones?
- Thyroxine-binding globulin (TBG): accounts for ~75% of bound hormone, highest affinity for T4
- Transthyretin (prealbumin): ~10%
- Albumin: ~10–20% (low affinity, high abundance)
- Less than 1% circulates as free hormone — only the free fraction is biologically active (free T4: ~0.2%; free T3: ~0.3%)
- — Cummings Otolaryngology
Q9. What is the role of deiodinases?
- T4 must be deiodinated to T3 for most biological actions
- Type I deiodinase: primary source of circulating T3; found in liver, kidney, thyroid; activated by TSH; inhibited by PTU
- Type II: mainly in CNS, pituitary, placenta; produces local T3; negatively regulated by thyroid hormone; not inhibited by PTU
- Type III: inactivates T4 and T3 by inner-ring deiodination → reverse T3 (rT3); high in fetal tissues (protects against excess hormone)
Q10. How is thyroid function controlled?
The hypothalamus–pituitary–thyroid axis: TRH (hypothalamus) → TSH (anterior pituitary) → thyroid hormone synthesis/secretion. TSH binds G protein-coupled receptors on thyroid follicular cells, primarily activating cAMP pathways. T3 and T4 exert negative feedback on both pituitary and hypothalamus.
CLINICAL ASSESSMENT
Q11. What questions would you ask in the history of a thyroid swelling?
- Duration, rate of growth, pain
- Pressure symptoms: dysphagia, dyspnoea, voice change (hoarseness → RLN involvement = red flag for malignancy), stridor
- Symptoms of hyper/hypothyroidism
- Family history (MEN2, familial papillary thyroid cancer, FAP)
- History of radiation exposure (therapeutic or Chernobyl/Fukushima type)
- Occupation, residence in endemic goitre areas
Q12. How do you examine the thyroid gland?
- Inspection: swelling moving with deglutition (thyroid or thyroglossal cyst), visible pulsation, distended neck veins (retrosternal goitre)
- Palpation from behind: size, consistency, nodularity, tenderness, fixity, tracheal deviation
- Kocher's test: compress lateral lobes — stridor indicates tracheal narrowing
- Berry's sign: loss of carotid pulsation on palpation — indicates malignant invasion of the carotid artery
- Pemberton's sign: raise arms above head — facial congestion/stridor = retrosternal goitre causing SVC compression
- Percussion over sternum for retrosternal extension
- Auscultation: bruit over a hypervascular gland (Graves' disease)
- Examine lymph nodes (cervical, supraclavicular) and assess for vocal cord function (voice)
Q13. What are the features suggesting malignancy in a thyroid nodule?
- Age < 14 or > 65 years; male sex
- Rapidly growing, hard, fixed mass
- Vocal cord paralysis (hoarseness)
- Cervical lymphadenopathy
- History of radiation exposure
- Family history of thyroid malignancy or MEN2
- Single "cold" nodule on scintigraphy
- Suspicious USG features: hypoechogenicity, microcalcifications, irregular margins, increased intranodular vascularity, size > 4 cm, subcapsular location, abnormal lymph nodes
- — Cummings Otolaryngology
INVESTIGATIONS
Q14. What is the initial investigation of a thyroid swelling?
TSH is the most important initial test. It determines the functional status of the gland.
- Low TSH → hyperthyroidism → proceed to free T4, T3, uptake scan
- Normal/high TSH → proceed to USS and FNAC
Q15. What is FNAC and what are the Bethesda categories?
Fine-needle aspiration cytology (FNAC) is the gold-standard investigation for evaluating thyroid nodules.
| Bethesda Category | Diagnosis | Malignancy Risk | Management |
|---|---|---|---|
| I | Non-diagnostic | 1–4% | Repeat FNAC |
| II | Benign | 0–3% | Follow-up USS |
| III | AUS/FLUS | 5–15% | Repeat FNAC / molecular testing |
| IV | Follicular neoplasm | 15–30% | Lobectomy |
| V | Suspicious for malignancy | 60–75% | Near-total/total thyroidectomy |
| VI | Malignant | 97–99% | Total thyroidectomy |
Q16. When is thyroid scintigraphy indicated?
Scintigraphy (uptake scan with Tc-99m or I-131) is indicated when:
- TSH is suppressed (to identify autonomously functioning "hot" nodules)
- Concern for ectopic thyroid tissue (lingual thyroid, thyroglossal duct remnant in known malignancy)
- A "hot" nodule is nearly always benign; a "cold" nodule has ~5–15% malignancy risk in adults (higher in children)
- — Cummings Otolaryngology
Q17. What does ultrasound show in thyroid malignancy?
Features suspicious for malignancy:
- Hypoechogenicity
- Microcalcifications (psammoma bodies in papillary carcinoma)
- Irregular or infiltrative margins
- Increased intranodular vascularity (on Doppler)
- Subcapsular location
- Size > 4 cm
- Abnormal lymph nodes (rounded, loss of fatty hilum, microcalcifications)
Q18. When is CT/MRI ordered for thyroid disease?
Not routine, but indicated for:
- Rapidly expanding tumour
- Retrosternal/mediastinal extension
- Bulky adenopathy
- Extrathyroidal disease
- Pre-op airway assessment
- Important: iodinated contrast CT should be avoided in suspected papillary or follicular carcinoma — it loads iodine and can delay radioactive iodine (RAI) therapy by months.
Q19. What are thyroid antibodies and their significance?
- Anti-thyroid peroxidase (anti-TPO): most sensitive for autoimmune thyroiditis (Hashimoto's); associated with hypothyroidism
- Anti-thyroglobulin (anti-Tg): less specific; can interfere with serum thyroglobulin assay used for cancer surveillance
- TSH-receptor antibodies (TRAb/TSHR Ab): in Graves' disease; stimulating antibodies drive hyperthyroidism
- Calcitonin: marker for medullary thyroid carcinoma (C-cell tumour)
- Thyroglobulin: tumour marker post-thyroidectomy for differentiated thyroid cancer; should be undetectable after ablation
THYROID DISORDERS
Q20. What are the causes of hyperthyroidism?
- Graves' disease (most common) — TSH receptor–stimulating antibodies
- Toxic multinodular goitre (Plummer's disease)
- Toxic adenoma (autonomously functioning "hot" nodule)
- Thyroiditis (early phase) — de Quervain's, Hashimoto's
- Iodine-induced (Jod-Basedow)
- TSH-secreting pituitary adenoma
- Exogenous thyroid hormone ingestion
Q21. What is Graves' disease?
An autoimmune condition caused by TSH-receptor stimulating antibodies (TRAb). Classic triad: hyperthyroidism, diffuse goitre, and Graves' ophthalmopathy (GO). Pretibial myxoedema is a rare feature. GO is a separate autoimmune orbital process; its activity is independent of thyroid status though smoking is a major risk factor. The natural history of GO involves an active inflammatory phase (6 months–2 years) followed by chronic fibrosing phase. ~50% improve spontaneously, 34% stabilise, 16% worsen.
Q22. What are the treatment options for hyperthyroidism?
- Antithyroid drugs (ATD): Carbimazole (preferred) or PTU — blocks organification; PTU also blocks peripheral T4→T3 conversion. Treat for 12–18 months, ~50% relapse rate.
- Radioactive iodine (RAI/I-131): Definitive; contraindicated in pregnancy and active moderate-severe GO. Note: RAI can worsen GO.
- Surgery (thyroidectomy): Indicated for large goitre with pressure symptoms, malignancy suspicion, patient preference, failure of ATD. Patient must be rendered euthyroid before surgery.
Q23. What is thyroid storm?
A life-threatening thyrotoxic crisis. Usually precipitated by infection, surgery, trauma, discontinuation of ATDs, or I-131 therapy.
Clinical features: fever > 38.5°C, tachycardia, CNS dysfunction (anxiety, agitation, delirium, psychosis, seizures, coma), atrial fibrillation, congestive cardiac failure.
Treatment (Cummings):
- ATDs in large doses (PTU preferred — also blocks conversion)
- Propranolol IV/oral — controls tachycardia and neuromuscular symptoms (most immediately effective)
- Glucocorticoids — hydrocortisone 50 mg or dexamethasone 2 mg IV every 8 hours
- Inorganic iodine 50–100 mg QID (given after ATDs, to block hormone release — Wolff-Chaikoff effect)
- Supportive: anti-pyretics, IV fluids, treat precipitant
- Plasmapheresis: reserved for refractory cases prior to surgery
Q24. What is myxoedema coma?
A life-threatening emergency representing the extreme of hypothyroidism. Precipitated by infection or other illness.
Features: extreme hypothermia, bradycardia, pleural and pericardial effusions, hyponatraemia, hypoventilation, respiratory acidosis, hypoxia, seizures preceding coma.
Management: IV T4 in large doses + IV hydrocortisone, intubation and ventilation, cautious rewarming, blood pressure support. Mortality ~50%.
THYROID NODULE & GOITRE
Q25. How do you classify goitre?
- By aetiology: endemic (iodine deficiency), sporadic, physiological (puberty, pregnancy), inflammatory, neoplastic, Graves'
- By pathology: diffuse/nodular; toxic/non-toxic
- WHO grading (palpation):
- Grade 0: No goitre
- Grade 1: Palpable but not visible
- Grade 2: Visible and palpable
Q26. What is the management of a thyroid nodule?
- TSH + USS
- If USS suspicious → FNAC (Bethesda classification guides next step)
- Benign (Bethesda II): serial USS every 6–18 months; repeat FNAC if growth
- Bethesda IV (follicular neoplasm): lobectomy — cannot distinguish follicular adenoma from follicular carcinoma on cytology; diagnosis requires histopathological demonstration of capsular or vascular invasion
- Bethesda V/VI: total thyroidectomy ± central neck dissection
THYROID MALIGNANCY
Q27. What are the types of thyroid cancer?
| Type | Frequency | Cell of Origin | Features |
|---|---|---|---|
| Papillary (PTC) | ~85% | Follicular cells | Psammoma bodies, nuclear grooves, Orphan Annie nuclei; lymphatic spread; excellent prognosis |
| Follicular (FTC) | ~10% | Follicular cells | Haematogenous spread (bone, lung); diagnosis requires histology (capsular/vascular invasion) |
| Medullary (MTC) | ~5% | Parafollicular C-cells | Calcitonin marker; amyloid stroma; RET proto-oncogene mutation; MEN2 associated |
| Anaplastic | <2% | Follicular cells | Rapidly fatal; elderly; does not take up RAI; chemoradiation only |
| Lymphoma | Rare | B-lymphocytes | On background of Hashimoto's; responds to chemoradiotherapy |
Q28. What are the genetic mutations associated with thyroid cancer?
- PTC in adults: BRAF V600E mutation (most common ~60%)
- PTC in children: RET/PTC rearrangements (more common than BRAF in paediatric cases)
- MTC: RET proto-oncogene mutation (germline in MEN2A, MEN2B; somatic in sporadic)
- FTC: RAS mutations, PAX8-PPAR-γ translocation
- Anaplastic: TP53 mutations
Q29. What is MEN2 and its relevance to thyroid cancer?
- MEN2A: MTC + phaeochromocytoma + parathyroid hyperplasia (RET codon 634 mutation most common)
- MEN2B: MTC + phaeochromocytoma + mucosal neuromas + marfanoid habitus (RET codon 918 mutation)
- Genetic testing is mandatory in all MTC patients; prophylactic thyroidectomy is recommended in RET mutation carriers
Q30. How would you manage a case of well-differentiated thyroid cancer (PTC/FTC)?
- Total thyroidectomy (as it allows RAI ablation and monitoring via thyroglobulin)
- Central neck dissection (Level VI): if clinical/radiological lymph node involvement; routine bilateral central dissection is debated but performed in paediatric cases
- Lateral neck dissection (modified radical/selective): for proven lateral nodal disease
- Postoperative RAI ablation: indicated for distant metastases, T3/T4 tumours, or extensive nodal involvement
- TSH suppression therapy: levothyroxine to suppress TSH below normal — reduces stimulation of any residual tumour cells
- Surveillance: serum thyroglobulin (± anti-Tg antibodies) + neck USS; whole-body RAI scan if thyroglobulin rises
Q31. What are psammoma bodies and where are they seen?
Psammoma bodies are concentrically laminated calcified structures formed by dystrophic calcification within papillae of papillary thyroid carcinoma. They are pathognomonic of PTC and appear as microcalcifications on ultrasound — a key suspicious feature.
SURGERY
Q32. What are the indications for thyroidectomy?
- Confirmed or suspected thyroid malignancy
- Follicular neoplasm (Bethesda IV)
- Pressure symptoms from goitre (dysphagia, dyspnoea, stridor)
- Retrosternal goitre
- Graves' disease refractory to or unsuitable for medical therapy or RAI
- Cosmetic indication
- Patient preference
Q33. What are the types of thyroid surgery?
- Hemithyroidectomy (lobectomy): removes one lobe + isthmus; for solitary nodule, follicular neoplasm
- Near-total thyroidectomy: leaves < 1 g of tissue at ligament of Berry to protect RLN
- Total thyroidectomy: removes all thyroid tissue; required for malignancy
- Subtotal thyroidectomy: leaves 5–7 g bilaterally; less popular now due to recurrence
- Completion thyroidectomy: removes residual lobe after prior lobectomy when malignancy confirmed on histology
Q34. How would you identify the RLN during thyroidectomy?
The RLN is best identified:
- In the tracheoesophageal groove (most reliable landmark)
- At the level of Zuckerkandl's tubercle — the nerve lies medial to the tubercle
- Near Berry's ligament — the nerve may branch or pass through the ligament here
- Intraoperative nerve monitoring (IONM) is increasingly used — reduces risk but does not replace careful dissection
Q35. What is the blood supply of the parathyroid glands and how do you preserve them?
The superior and inferior parathyroid glands (usually 4 in total) are supplied by the inferior thyroid artery. During thyroidectomy, the parathyroids are preserved by:
- Identifying all 4 parathyroids before ligating vessels
- Ligating branches of the inferior thyroid artery close to the thyroid capsule ("capsular dissection")
- Autotransplantation: if vascularity is compromised, the parathyroid is minced and implanted into the sternocleidomastoid or forearm muscle
COMPLICATIONS
Q36. What are the complications of thyroidectomy?
Immediate:
- Haemorrhage → haematoma (life-threatening — can compress airway; requires immediate wound opening at bedside)
- Laryngospasm, tetany (early hypocalcaemia)
Early:
- Hypocalcaemia (most common complication) — due to hypoparathyroidism; transient or permanent; presents as perioral tingling, Chvostek's sign (facial twitch on tapping facial nerve), Trousseau's sign (carpopedal spasm on inflation of BP cuff)
- RLN palsy — hoarseness (unilateral); respiratory distress, stridor requiring re-intubation (bilateral)
- Wound infection, seroma
- Thyroid storm (if operated on unprepared hyperthyroid patient)
Late:
- Hypothyroidism (requires lifelong T4 replacement after total thyroidectomy)
- Permanent hypoparathyroidism
- Keloid/hypertrophic scar
- Voice change (EBSLN injury — loss of high pitch)
- Tracheomalacia (rare, in long-standing large goitre)
Q37. What is the management of post-thyroidectomy hypocalcaemia?
- Monitor serum calcium 12–24 hours post-op
- Symptomatic hypocalcaemia: IV calcium gluconate (10 mL of 10% solution) over 10 minutes, followed by infusion; oral calcium + calcitriol (active vitamin D) long term
- Intact PTH level at 24 hours predicts risk of permanent hypoparathyroidism — PTH < 10 pg/mL is a reliable predictor
Q38. How do you manage a post-thyroidectomy neck haematoma?
A rapidly expanding haematoma is a surgical emergency:
- Immediately open wound and evacuate clot at the bedside to relieve airway compression
- Call for anaesthesia support
- Return to theatre for formal haemostasis
SPECIAL TOPICS
Q39. What is lingual thyroid?
Failure of the thyroid gland to descend from the foramen caecum results in a lingual thyroid — the most common form of ectopic thyroid. It may be the only functioning thyroid tissue in the body. Before any surgery or RAI treatment, a radionuclide scan must confirm the presence of normal ectopic tissue in the neck to avoid causing hypothyroidism.
Q40. What is the difference between primary and secondary hypothyroidism?
- Primary (thyroid failure): High TSH, low free T4 — most common. Causes: Hashimoto's thyroiditis (iodine-sufficient areas), iodine deficiency (worldwide)
- Secondary (pituitary failure): Low TSH, low free T4 — e.g., pituitary adenoma, Sheehan syndrome
- Tertiary (hypothalamic failure): Low TRH → low TSH → low T4
Q41. What drugs can affect thyroid function tests?
- Amiodarone: can cause hypo or hyperthyroidism (contains large amounts of iodine; inhibits T4→T3 conversion)
- Lithium: inhibits thyroid hormone release → hypothyroidism/goitre
- Phenytoin, carbamazepine, phenobarbital, rifampin: increase T4 catabolism → increased dose requirement
- Oestrogens: increase TBG → increased total T4 (but free T4 unchanged)
- Ferrous sulfate, calcium carbonate, aluminum hydroxide, sucralfate, cholestyramine: impair T4 absorption from gut — separate dose by several hours
Q42. What is the significance of thyroglobulin post-thyroidectomy?
Thyroglobulin is synthesised exclusively by thyroid follicular cells. After total thyroidectomy and RAI ablation, serum thyroglobulin should be undetectable. Rising levels indicate:
- Residual thyroid tissue
- Tumour recurrence It is monitored at regular follow-up intervals, with stimulation by TSH withdrawal or recombinant TSH (rhTSH/Thyrogen) to increase sensitivity. Anti-thyroglobulin antibodies (anti-Tg Ab) can interfere with the assay and must be measured simultaneously.
Sources: Cummings Otolaryngology Head and Neck Surgery (9780323612173) | K.J. Lee's Essential Otolaryngology (9781260122237)
Plummers disease
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a complete viva-ready account of Plummer's disease from multiple authoritative sources.
Plummer's Disease (Toxic Multinodular Goitre)
Definition & Eponym
Plummer's disease = Toxic Multinodular Goitre (TMNG) — an enlarged nodular thyroid containing one or more autonomously functioning nodules that produce excess thyroid hormone, leading to hyperthyroidism. Named after Henry Plummer of the Mayo Clinic, 1913.
Epidemiology
- Second most common cause of hyperthyroidism in the United States after Graves' disease
- Among the elderly and in iodine-deficient regions, it is the most common cause of hyperthyroidism
- Female predominance — approximately 5:1 female-to-male ratio
- Typically affects adults above 50 years of age
- Develops from a pre-existing non-toxic nodular goitre — long history of thyroid enlargement with insidious onset of thyrotoxicosis
- — Sabiston Textbook of Surgery
Pathogenesis
- Develops from long-standing multinodular (non-toxic) goitre
- Progressive nodule formation → evolution of hyperfunctional regions → excess thyroid hormone secretion → TSH suppression
- Autonomously functioning nodules often result from activating somatic mutations in the TSH receptor gene → constitutive cAMP signalling → cell proliferation + hormone secretion (independent of TSH)
- Less commonly: activating mutations in Gα subunit (similar to McCune-Albright syndrome)
- These mutations are NOT the same TSHR/Gα activating mutations seen in solitary toxic adenoma — in many toxic MNG nodules, the molecular basis remains unknown; many nodules are polyclonal (unlike solitary toxic adenoma which is more consistently monoclonal)
- — Harrison's Internal Medicine 22e; Sabiston
Stages of Progression (KJ Lee)
| Stage | TSH | T3/T4 | I-123 Scan | Notes |
|---|---|---|---|---|
| Early | Suppressed | Normal | Hot foci + suppressed background | Subclinical hyperthyroidism |
| Intermediate | Suppressed | Normal | Focal hot areas | Not yet truly autonomous |
| Overt (autonomous) | Suppressed | Elevated | Hot foci with complete absence of adjacent normal gland; uptake persists on suppression scan | Truly autonomous |
Subclinical hyperthyroidism = suppressed TSH but normal T4 and T3 — the prehyperthyroid pattern.
Key Distinction from Graves' Disease
| Feature | Plummer's Disease (TMNG) | Graves' Disease |
|---|---|---|
| Mechanism | Autonomous nodule(s), somatic TSH-R mutation | TSH-R stimulating antibodies (TRAb) |
| Age | > 50 years | Younger adults |
| Goitre | Asymmetric, nodular | Diffuse, smooth |
| Ophthalmopathy | Absent | Present (up to 50%) |
| Pretibial myxoedema | Absent | Rare but present |
| TRAb | Negative | Positive |
| Remission with ATDs | Does NOT occur | ~50% remission |
| Scintigraphy | Heterogeneous; multiple hot & cold areas | Diffuse increased uptake |
| Autoimmune aetiology | No | Yes |
Clinical Features
- Long history of goitre (often years–decades) with insidious onset of hyperthyroidism
- Symptoms of mild/subclinical hyperthyroidism — often subtler than Graves'
- Atrial fibrillation, palpitations, tachycardia — especially in the elderly (cardiac manifestations dominate)
- Tremor, nervousness, weight loss
- No ophthalmopathy, no pretibial myxoedema, no thyroid bruit
- Mass effects of the goitre: dysphagia, dyspnoea, stridor, SVC obstruction (Pemberton's sign if retrosternal)
- Jod-Basedow phenomenon: exposure to exogenous iodine (contrast dye, amiodarone) may precipitate or exacerbate thyrotoxicosis in TMNG patients with subclinical disease
- — Harrison's; KJ Lee's Otolaryngology
Investigations
Biochemistry
- TSH: low/suppressed (most important first test)
- Free T4: normal or mildly elevated
- T3: often elevated disproportionately more than T4 (T3 toxicosis common in early/mild disease)
- TRAb: negative (helps rule out Graves' disease)
- Thyroid antibodies (anti-TPO, anti-Tg): may be positive if concurrent autoimmune thyroiditis
Imaging
-
Radionuclide scintigraphy (I-123 or Tc-99m) — first-line imaging:
- Shows heterogeneous uptake — multiple areas of increased ("hot") and decreased ("cold") uptake
- 24-hour RAI uptake may be in the upper normal range (not as elevated as Graves')
- Identifies the location and distribution of autonomously functioning nodules
- Hot nodules are rarely malignant — do not require FNAC
- Cold nodules within the same gland must be evaluated independently (FNAC per sonographic criteria)
-
Ultrasound — mandatory as correlative study:
- Assesses overall thyroid size
- Characterises non-functioning nodules
- Identifies suspicious features requiring FNAC (hypoechogenicity, microcalcifications, irregular margins, increased vascularity)
-
CT/MRI — for retrosternal extension, tracheal compression, mediastinal disease (avoid iodinated contrast if RAI therapy planned)
Pathology (Gross & Microscopic)
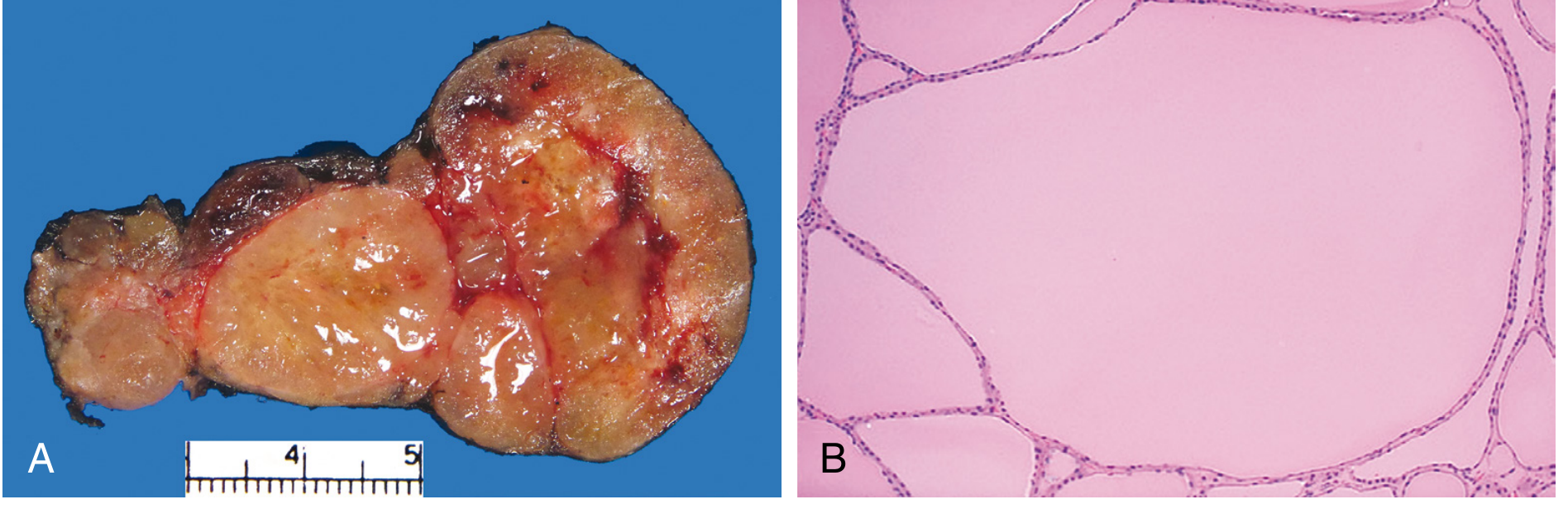
Gross:
- Multilobulated, asymmetrically enlarged gland — can exceed 2000 g
- Cut section: irregular nodules with brown, gelatinous colloid; areas of haemorrhage, fibrosis, calcification, cystic change
- One lobe may enlarge disproportionately; may extend retrosternally
Microscopic (Follicular Nodular Disease):
- Colloid-rich follicles lined by flattened, inactive epithelium (storage phase)
- Areas of follicular hyperplasia (active secretion)
- Degenerative changes: fibrosis, haemosiderin, calcification
- No prominent capsule between nodules and residual thyroid (distinguishes from true adenoma)
- The histological term is "follicular nodular disease"
Malignancy risk: Low (<5%) but not zero — suspicious nodules (particularly cold ones) should be biopsied. — Robbins Pathologic Basis of Disease
Treatment
Three options — same as Graves' but with important differences:
1. Antithyroid Drugs (ATDs)
- Carbimazole/methimazole or PTU — normalise thyroid function
- NOT a definitive long-term strategy — autonomous nodules do not undergo remission with ATDs (disease is not autoimmune)
- Used as preoperative preparation or in elderly/frail/terminally ill patients
2. Radioactive Iodine (RAI / I-131) — most common definitive treatment in the US
- Requires higher doses than Graves' disease (due to lower iodine uptake in TMNG) → higher risk of treatment failure and need for retreatment
- Must render euthyroid first with methimazole ± beta-blockade before RAI
- SSKI and Lugol's solution are CONTRAINDICATED in TMNG (unlike Graves'):
- In TMNG, exogenous iodine does NOT reliably achieve the Wolff-Chaikoff effect
- Instead, iodine can induce hyperthyroidism via the Jod-Basedow phenomenon
- Spontaneous remission does not occur — RAI or surgery is needed for definitive cure
- — Sabiston; Cummings
3. Surgery — most effective for rapid volume reduction
Indications for surgery over RAI:
- Large goitre with pressure symptoms (dysphagia, dyspnoea, stridor)
- Retrosternal extension
- Suspicious cold nodule(s) requiring histopathological diagnosis
- Failed or contraindicated RAI
- Patient preference (faster result, avoids radiation)
- Coexisting malignancy suspected
Procedure:
- Near-total or total thyroidectomy is recommended (eliminates recurrence risk)
- Bilateral subtotal thyroidectomy (leaving 3–6 g remnant) is an alternative but carries recurrence risk
- Patient must be rendered euthyroid preoperatively with methimazole ± beta-blocker
- Surgery more effective than RAI in rapidly reducing thyrotoxicosis and reducing goitre volume
- Risk of long-term hypothyroidism is higher with surgery than RAI
- — Cummings Otolaryngology; Sabiston
Jod-Basedow Phenomenon (Viva favourite)
- Iodine-induced hyperthyroidism in a patient with underlying autonomous thyroid nodules (TMNG or sub-clinical disease)
- Mechanism: autonomous nodules use the exogenous iodine load to synthesise and release excess T3/T4 without TSH stimulation
- Triggered by: iodinated contrast dye (CT scan), amiodarone, povidone-iodine, topical antiseptics
- Clinically important: before any CT with contrast in a patient with known TMNG, weigh the risk of precipitating thyroid storm
Key Viva Points — Summary
| Point | Answer |
|---|---|
| Eponym | Henry Plummer, Mayo Clinic, 1913 |
| Most common cause of hyperthyroidism | Graves' (overall); TMNG (elderly + iodine-deficient regions) |
| Eye signs | Absent |
| Scintigraphy finding | Heterogeneous — multiple hot & cold areas |
| Why hot nodules rarely malignant | Autonomous TSH-R mutations drive function; malignant cells lose differentiated function |
| Cold nodules in TMNG | Must be evaluated with FNAC — higher malignancy risk |
| Spontaneous remission | Does NOT occur (unlike Graves') |
| Why Lugol's/SSKI contraindicated | Jod-Basedow phenomenon — iodine worsens hyperthyroidism |
| Preferred preop preparation | Methimazole + beta-blockade (NOT iodine) |
| Surgical procedure | Near-total or total thyroidectomy |
| Molecular basis | Somatic activating TSH-R gene mutations (constitutive cAMP) |
Sources: Cummings Otolaryngology Head and Neck Surgery | KJ Lee's Essential Otolaryngology | Harrison's Internal Medicine 22e | Sabiston Textbook of Surgery | Robbins Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.