Clinical anatomy of the ear. Physiology and rescarch methods of auditory and vestibular analyzers.
Reading File
Finding Sources
Finding Sources
Searching Images
anatomy of the ear clinical diagram
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Searching Images
inner ear cochlea vestibular apparatus anatomy cross section
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from Cummings Otolaryngology to assemble a thorough response. Let me compile the answer.
Clinical Anatomy of the Ear — Physiology & Research Methods of Auditory and Vestibular Analyzers
I. CLINICAL ANATOMY OF THE EAR
A. Temporal Bone
The ear is housed within the temporal bone, which has four embryologically distinct components: squamous, mastoid, petrous, and tympanic parts. The temporal bone articulates with the sphenoid, parietal, occipital, and zygomatic bones, contributing to the cranial, skull base, and facial structures.
- Squamous part — forms the lateral wall of the middle fossa; bears the temporal line, a surface landmark aligned with the zygomatic process.
- Mastoid part — contains the mastoid antrum (deep to the MacEwen triangle); communicates with the middle ear via the aditus ad antrum.
- Petrous part — contains the inner ear and internal auditory canal; the arcuate eminence on its superior surface marks the position of the superior semicircular canal.
- Tympanic part — forms most of the osseous external auditory canal (EAC) and the floor/anterior wall of the middle ear.
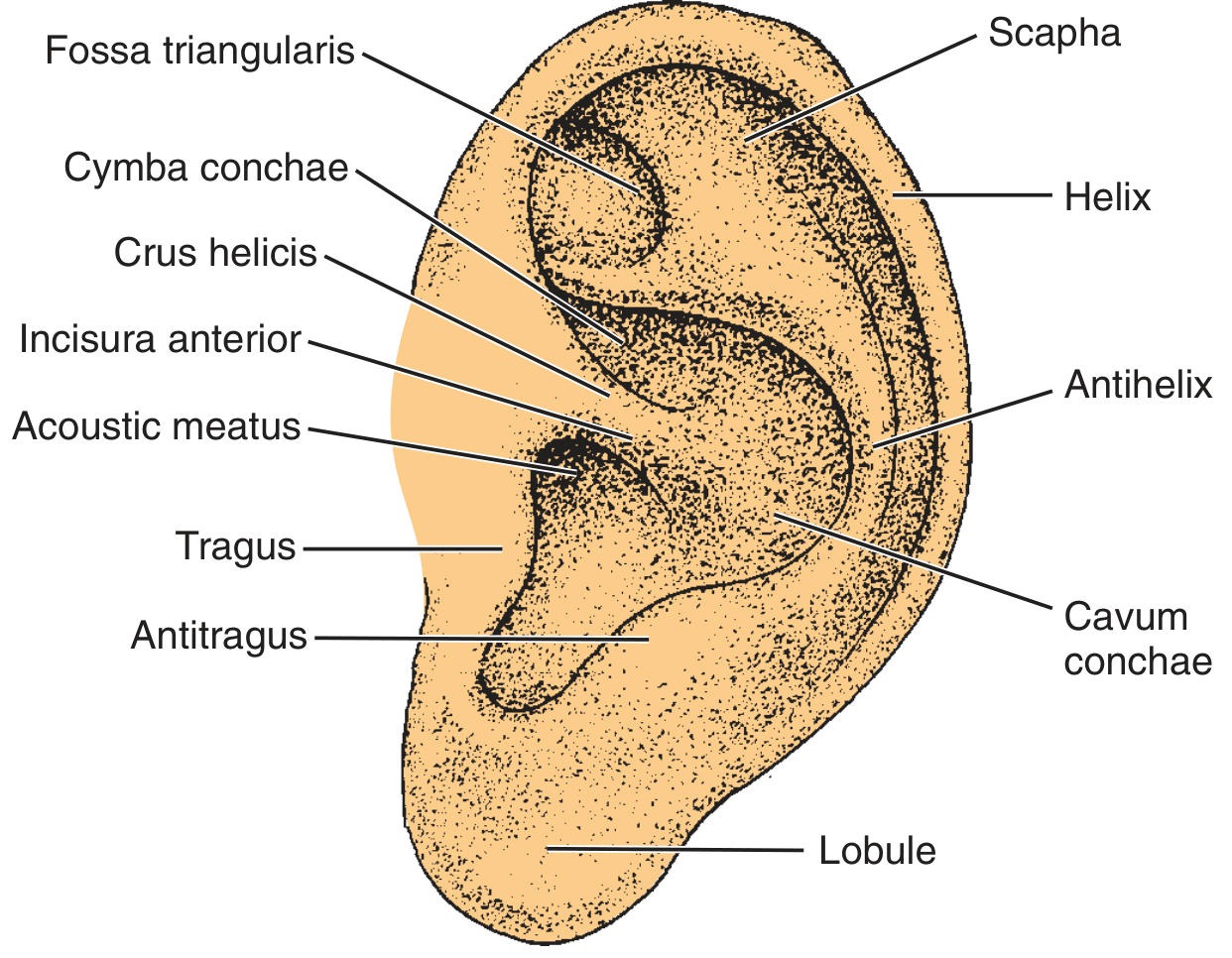
B. External Ear
Auricle (Pinna)
The auricle is a funnel-shaped elastic cartilage framework covered by tightly adherent skin. Key surface landmarks include:
- Helix, antihelix, scapha, triangular fossa
- Concha (resonant frequency ~5300 Hz), tragus, antitragus
- Intertragal notch, lobule (the only cartilage-free part)
The auricle develops from the billocks of His — condensations from the 1st and 2nd branchial arches. Sensory innervation: auriculotemporal branch of V3 (1st arch territory) and a cutaneous branch of the facial nerve (2nd arch territory).
External Auditory Canal (EAC)
- ~2.5 cm in adults; lateral third is cartilaginous/membranous, medial two-thirds is bony.
- The cartilaginous portion contains hair follicles, sebaceous glands, and apocrine (ceruminous) glands that produce cerumen — a hydrophobic, slightly acidic (pH 6.0–6.5) substance.
- The isthmus (bony-cartilaginous junction) is the narrowest point; a site of osteomyelitis granulation in malignant otitis externa.
- Fissures of Santorini — natural defects in the cartilaginous canal that allow spread of infection or neoplasm to the parotid gland.
- Foramen of Huschke — a defect from incomplete ossification in the anterior bony canal; allows spread to the deep parotid lobe.
- The canal has a unique self-cleansing mechanism: keratinous epithelium migrates centrifugally from the TM toward the meatus.
Normal EAC flora is overwhelmingly Gram-positive: S. auricularis, S. epidermidis; Pseudomonas aeruginosa is rare in healthy subjects but is the principal pathogen in malignant otitis externa.
C. Tympanic Membrane (TM)
The TM is a four-layered, concave membrane connecting the EAC to the middle ear:
| Layer | Description |
|---|---|
| Lateral epithelial | Continuous with EAC skin |
| Outer fibrous (radiate) | Inserts radially on the malleus manubrium |
| Inner fibrous (circular) | Circumferential arrangement at periphery |
| Medial mucosal | Middle ear mucosa |
- Peripherally, both fibrous layers merge into the annular ligament, anchoring the TM in the bony tympanic sulcus.
- Pars tensa (thicker, inferior) — has all four layers; the majority of the TM.
- Pars flaccida / Shrapnell membrane (thinner, superior) — lacks the fibrous layer; bounded by the notch of Rivinus; vulnerable to retraction cholesteatoma.
- Otoscopic landmarks: manubrium/mallear stria, umbo (tip of malleus), lateral process, light reflex (anterior-inferior quadrant), pars flaccida, annulus.
D. Middle Ear
The middle ear is an air-filled space derived from the first pharyngeal pouch (endoderm). It is subdivided into:
- Hypotympanum — below the TM annulus
- Mesotympanum — medial to the TM; contains the oval window (occupied by the stapes footplate) and round window
- Epitympanum (attic) — superior compartment; contains the head of malleus and body of incus; the Prussak space lies lateral to the malleus neck and is the origin of pars flaccida cholesteatomas
Ossicular chain:
| Ossicle | Key features |
|---|---|
| Malleus | Manubrium coupled to TM; head in epitympanum |
| Incus | Long process has single nutrient vessel — most vulnerable to resorption |
| Stapes | Footplate sits in oval window; stapedius tendon inserts on its capitulum |
Eustachian tube (ET): Angled ~45° from the middle ear to the nasopharynx; proximal third bony, distal two-thirds fibrocartilaginous. The tensor veli palatini opens it during swallowing/yawning. The carotid artery lies medial to the tympanic orifice.
Facial nerve in the middle ear: Runs through the fallopian canal — most commonly dehiscent (55% of cases) above the oval window. Landmarks: cochleariform process, pyramidal eminence, second genu.
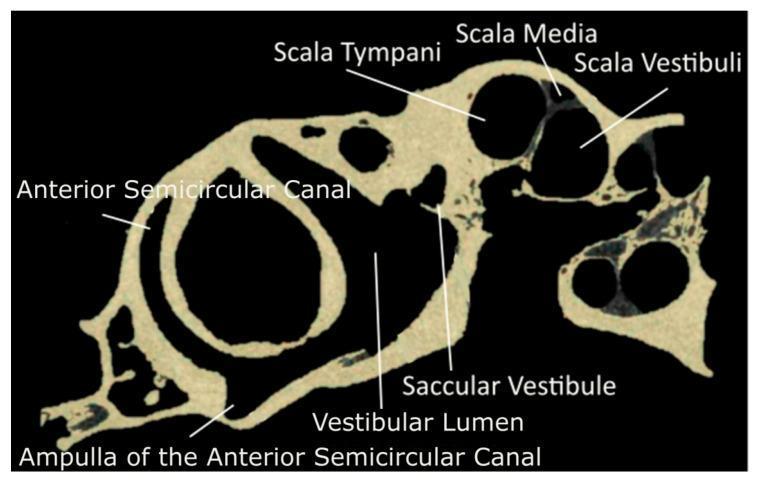
E. Inner Ear (Labyrinth)
Housed within the otic capsule of the petrous temporal bone. Consists of the bony labyrinth (perilymph-filled) and the membranous labyrinth (endolymph-filled).
Scala divisions of the cochlea:
- Scala vestibuli — perilymph; communicates with vestibule
- Scala media (cochlear duct) — endolymph; contains the organ of Corti
- Scala tympani — perilymph; ends at the round window membrane
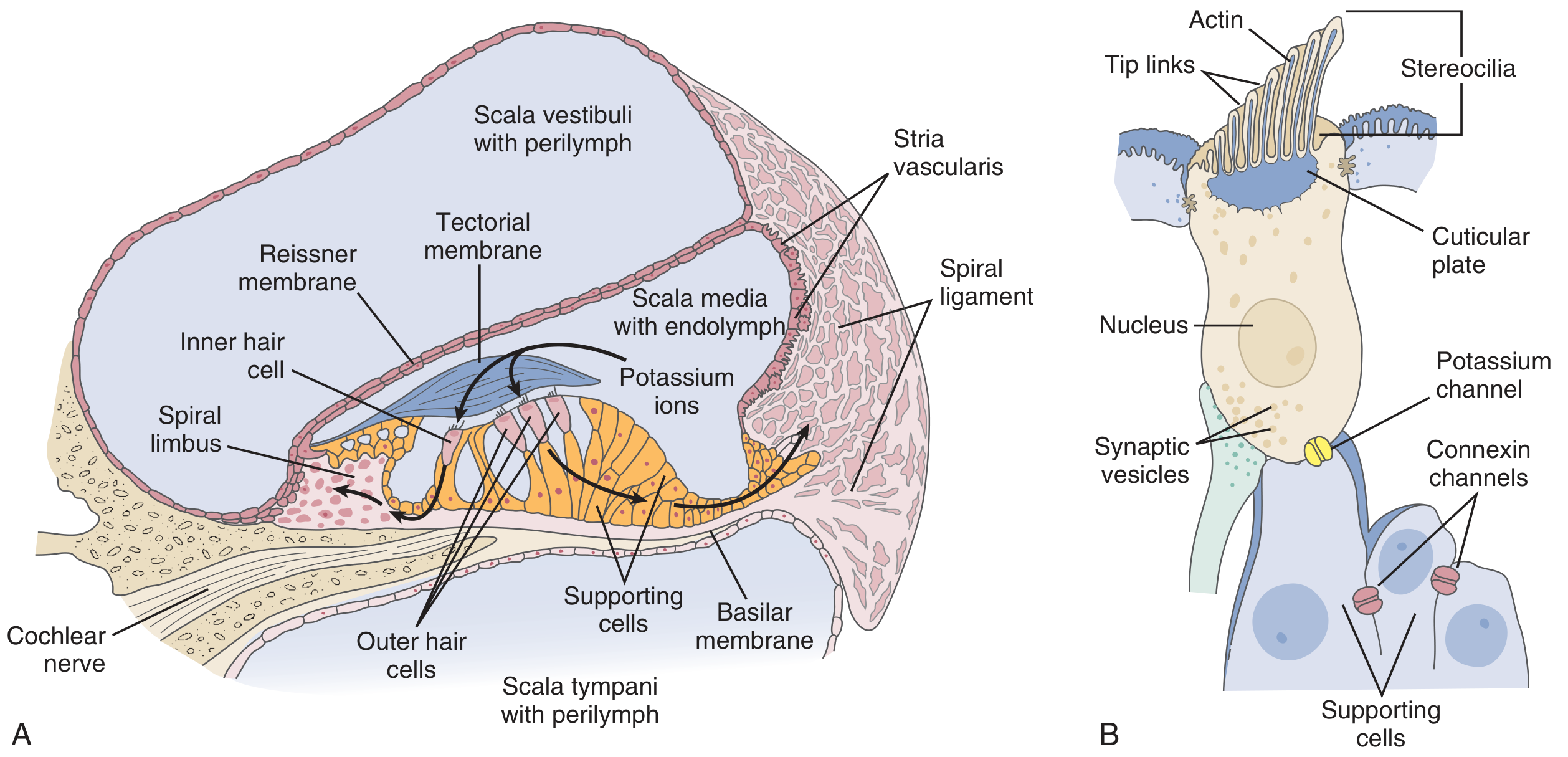
Organ of Corti lies on the basilar membrane and is covered by the tectorial membrane:
- Contains inner hair cells (IHC) — one row; primary afferent transducers (~3500 cells)
- Contains outer hair cells (OHC) — three rows; electromotile amplifiers (~12,000 cells)
- Stereocilia are connected by tip links
Vestibular apparatus:
- 3 semicircular canals (SCC) — superior (anterior), posterior, lateral — detect angular acceleration
- Otolith organs: utricle (horizontal acceleration, head tilt) and saccule (vertical acceleration)
- Each SCC ends in an ampulla containing a crista ampullaris with hair cells embedded in a cupula
II. PHYSIOLOGY OF THE AUDITORY ANALYZER
A. Sound Transmission — Outer and Middle Ear
-
Outer ear: The pinna and EAC funnel sound and amplify specific frequencies. The concha resonates at ~5300 Hz; the EAC at ~3000 Hz. The head shadow effect assists binaural sound localization:
- Interaural time difference — critical for low frequencies
- Interaural amplitude difference — critical for high frequencies
-
Middle ear impedance matching: Air-to-fluid impedance mismatch (~30 dB loss without compensation) is overcome by three mechanisms:
- Area ratio of TM (~55 mm²) to oval window (~3.2 mm²) — ~17:1 pressure amplification
- Lever ratio of the ossicular chain (~1.3:1)
- Conical shape of the TM (buckling effect)
Acoustic impedance has three components: stiffness (dominates low frequencies), mass (dominates high frequencies), and resistance (damping). Resonance occurs when stiffness and mass cancel out. -
Sound conduction pathways:
- Ossicular (air) conduction — dominant pathway: TM → malleus → incus → stapes footplate → oval window → perilymph
- Bone conduction — vibration of temporal bone directly stimulates cochlear fluids
B. Cochlear Transduction
Traveling wave: Sound entering the cochlea creates a traveling wave on the basilar membrane (von Békésy). The basilar membrane is tonotopically organized:
- High frequencies → base (narrow, stiff)
- Low frequencies → apex (wide, compliant)
Mechanoelectrical transduction:
- Basilar membrane displacement deflects hair cell stereocilia via the tectorial membrane
- Tip links open mechanically gated K⁺ channels (TMC1, TMC2 proteins)
- K⁺ influx from endolymph (high [K⁺], +80 mV endocochlear potential maintained by the stria vascularis) depolarizes the hair cell
- Depolarization opens voltage-gated Ca²⁺ channels on the basolateral surface
- Ca²⁺ triggers exocytosis of neurotransmitter (glutamate) at the ribbon synapse → activates primary afferent auditory neurons (CN VIII)
- K⁺ is recycled back to the stria vascularis via connexin gap junctions in supporting cells
OHC electromotility (active amplification): OHCs change length in response to voltage (prestin motor protein), amplifying basilar membrane motion by ~40–50 dB.
C. Auditory Neural Pathway
| Level | Structure | Key Features |
|---|---|---|
| 1st order | Spiral ganglion → CN VIII | Tonotopically tuned; high-SR neurons detect low levels, low-SR neurons have wider dynamic range |
| 2nd order | Cochlear nucleus (pontomedullary junction) | First central relay; 3 divisions: dorsal CN, anterior VCN, posterior VCN |
| 3rd order | Superior olivary complex (SOC) | First site of binaural interaction; origin of olivocochlear (OC) efferent fibers |
| 4th order | Lateral lemniscus + Inferior colliculus (IC) | Bilateral projections; sound localization |
| 5th order | Medial geniculate body (thalamus) | Ventral → primary auditory cortex; dorsal → association cortex |
| Cortex | Heschl's gyrus (Brodmann 41) = AI; Brodmann 22/42 = A2 (Wernicke) | Tonotopic; high freq medial, low freq lateral |
D. Efferent Auditory System
Stapedius reflex (acoustic reflex):
- Triggered by loud sounds (~70–90 dB above threshold)
- Sound → cochlea → CN VIII → cochlear nucleus → interneurons → facial nerve nucleus → stapedius muscle contraction
- Increases ossicular impedance → protects cochlea from loud, low-frequency sounds
- Bilateral and consensual (like the pupillary light reflex)
Olivocochlear (OC) efferent system:
- Medial OC (MOC) fibers → synapse directly on OHCs → reduce OHC electromotility → suppress basilar membrane response
- Function: improves speech perception in noise by suppressing background
III. PHYSIOLOGY OF THE VESTIBULAR ANALYZER
Semicircular canals — angular acceleration:
- Endolymph deflects the cupula in each ampulla
- Hair cell stereocilia are displaced → depolarization or hyperpolarization depending on direction
- The lateral SCC pair operates as a push-pull system: head rotation to one side increases firing rate in the ipsilateral canal and decreases it contralaterally
Otolith organs (utricle & saccule) — linear acceleration & gravity:
- Hair cells are embedded in the macula, covered by an otolithic membrane containing calcium carbonate crystals (otoliths/otoconia)
- Inertia of otoconia deflects stereocilia → detects head tilt and linear motion
Vestibular neural pathway:
- 1st order: Scarpa's ganglion → superior and inferior vestibular nerves → CN VIII
- 2nd order: Vestibular nuclei (medulla) → cerebellum, spinal cord (vestibulospinal reflex), extraocular motor nuclei (vestibuloocular reflex, VOR), cortex
Vestibuloocular reflex (VOR): Stabilizes gaze during head movement; operates at latency ~10 ms. Tested by head impulse test and caloric testing.
IV. RESEARCH METHODS / AUDIOLOGICAL AND VESTIBULAR TESTING
A. Auditory Analyzer
| Method | Principle | Clinical Use |
|---|---|---|
| Pure tone audiometry (PTA) | Threshold detection for 0.25–8 kHz via air and bone conduction | Classify hearing loss (conductive, sensorineural, mixed); degree and configuration |
| Speech audiometry | Speech recognition threshold (SRT) and word recognition score (WRS) | Assess suprathreshold hearing function |
| Tympanometry | Measures TM compliance vs. ear canal pressure | Middle ear effusion, TM perforation, ossicular fixation; classifies into Types A, B, C |
| Acoustic reflex testing | Stapedius reflex threshold and decay | Cochlear vs. retrocochlear pathology; facial nerve assessment |
| Otoacoustic emissions (OAEs) | Measures sounds produced by OHC electromotility (DPOAEs, TEOAEs) | Newborn hearing screening; cochlear function; separated from neural function |
| Auditory brainstem response (ABR) | Click-evoked far-field potentials (Waves I–V) | Threshold estimation, retrocochlear pathology (acoustic neuroma), intraoperative monitoring |
| Auditory steady-state response (ASSR) | Frequency-specific threshold estimation | Frequency-specific audiometry in infants |
| Electrocochleography (ECochG) | Summating potential (SP) and action potential (AP); SP/AP ratio | Ménière's disease (hydrops) — elevated SP/AP ratio > 0.4 |
B. Vestibular Analyzer
| Method | Principle | Clinical Use |
|---|---|---|
| Caloric testing | Warm (44°C) and cool (30°C) water/air in EAC creates convection currents → stimulates horizontal SCC | Assesses each labyrinth independently; canal paresis, directional preponderance (Jongkees formula) |
| Video head impulse test (vHIT) | Measures VOR gain during rapid head rotation; detects catch-up saccades | SCC-specific hypofunction; sensitive for lateral SCC |
| Videonystagmography (VNG) / ENG | Records eye movements during positional tests, gaze testing, caloric tests | Peripheral vs. central vestibular disorders |
| Rotary chair testing | Sinusoidal or step rotation; measures VOR gain, phase, and symmetry | Bilateral vestibular hypofunction; cannot lateralize |
| Dix-Hallpike test | Provocative positional test | Diagnoses posterior SCC BPPV (upbeat torsional nystagmus) |
| Cervical/ocular VEMP (cVEMP / oVEMP) | Vestibular evoked myogenic potentials from sternocleidomastoid or extraocular muscles | cVEMP tests saccule + inferior vestibular nerve; oVEMP tests utricle + superior vestibular nerve |
| Posturography (CDP) | Platform sway under 6 sensory conditions (Sensory Organization Test) | Balance rehabilitation; identifies somatosensory, visual, or vestibular deficits |
| MRI of IAC | High-resolution T2/CISS sequences | Acoustic neuroma, labyrinthitis ossificans, superior SCC dehiscence |
Sources: Cummings Otolaryngology Head and Neck Surgery (Chapters 126 & 128); Miller's Anesthesia 10e (Chapter 66).
This is a shared conversation. Sign in to Orris to start your own chat.