Digestive System: Anatomy - Mouth, Pharynx, Esophagus, Deglutition, Stomach, Pancreas, Liver and Gallbladder, Small Intestine, Large Intestine, Phases of Digestion - Mechanical and chemical processes. Absorption of nutrients. Disorders - GERD, ulcers, celiac disease
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Searching Images
gastric secretion parietal cell acid mechanism diagram
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Digestive System: Comprehensive Guide
1. MOUTH (Oral Cavity)
The mouth is where both mechanical and chemical digestion begin.
Anatomy
- Teeth: Incisors (cutting force ~55 lbs), molars (grinding force ~200 lbs)
- Tongue: Manipulates food, initiates the voluntary phase of swallowing
- Salivary glands (parotid, submandibular, sublingual): secrete saliva (~1.5 L/day)
Mechanical Digestion: Mastication (Chewing)
Chewing is controlled by the motor branch of CN V (trigeminal). A chewing reflex operates: the bolus causes reflex inhibition of jaw muscles → jaw drops → stretch reflex → rebound contraction → closes teeth. Chewing is especially important for fruits and vegetables that have indigestible cellulose membranes; it also dramatically increases surface area for enzymatic action. — Guyton & Hall Textbook of Medical Physiology
Chemical Digestion
- Salivary amylase (ptyalin): begins starch hydrolysis (cleaves α-1,4 glycosidic bonds)
- Lingual lipase: minor initial fat digestion
- Saliva maintains oral pH (~6.8–7.0) and lubricates the bolus with mucin
2. PHARYNX
The pharynx serves dual functions — respiration and swallowing — and is converted into a food passage for only a few seconds at a time.
Anatomy
- Nasopharynx (above soft palate)
- Oropharynx (behind mouth)
- Laryngopharynx (connects to larynx and esophagus)
- Key structures: soft palate, epiglottis, palatopharyngeal folds, tonsillar pillars, upper esophageal sphincter (UES)
3. DEGLUTITION (Swallowing)
Swallowing has three stages (Guyton & Hall; Ganong's Review of Medical Physiology):
Stage 1 — Voluntary
The tongue squeezes the bolus posteriorly against the hard palate into the pharynx. Once initiated, the reflex becomes involuntary.
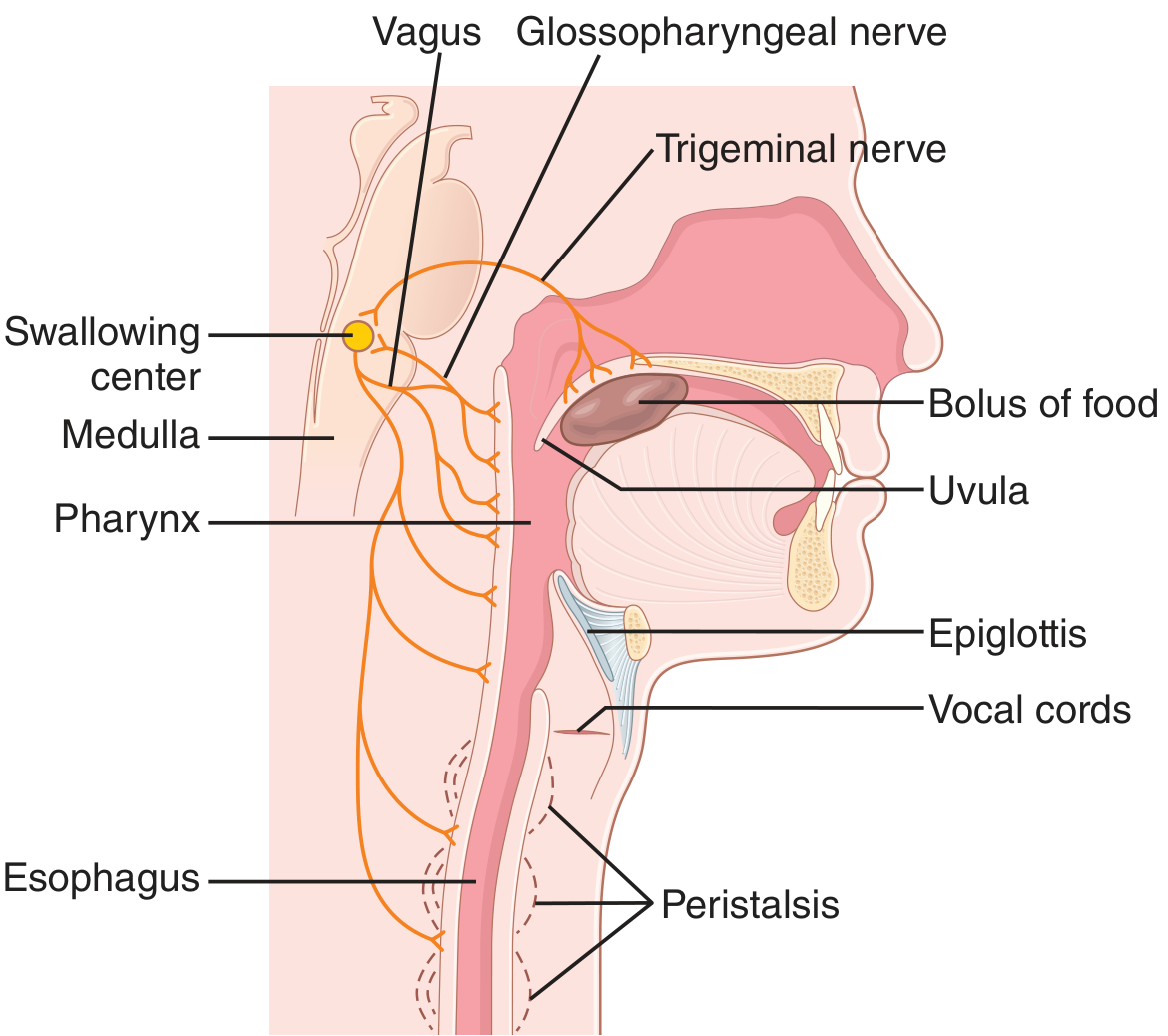
Stage 2 — Pharyngeal (Involuntary)
Triggered by afferent impulses in CN V, IX, and X, integrated in the nucleus of the tractus solitarius and nucleus ambiguus in the medulla. The sequence:
- Soft palate elevates → closes posterior nares (prevents nasal reflux)
- Palatopharyngeal folds approximate → form a slit (food filter)
- Vocal cords approximate; larynx pulled upward and anteriorly; epiglottis tips backward over the glottis (prevents aspiration)
- UES relaxes → food enters esophagus
- Respiration is inhibited throughout this stage
Stage 3 — Esophageal (Involuntary)
A peristaltic wave sweeps at ~4 cm/s from UES to LES. Liquids reach the stomach before the wave arrives (gravity-assisted in upright position); if residual food remains, a secondary peristaltic wave is triggered.
Sphincters
| Sphincter | Location | Resting Pressure | Key Function |
|---|---|---|---|
| UES (pharyngoesophageal) | Pharynx–esophagus junction | Highest of all GI sphincters | Prevents air entry during respiration; opens during swallowing |
| LES (lower esophageal) | Esophagus–stomach junction | Maintained by intrinsic myogenic tone + cholinergic input | Permits food into stomach; prevents gastric reflux |
The LES is relaxed by VIP and NO (via vagal interneurons) and contracted by acetylcholine from vagal endings. — Medical Physiology, Boron & Boulpaep
4. ESOPHAGUS
- A muscular tube ~25 cm long
- Upper third: striated muscle; lower two-thirds: smooth muscle; middle third: mixed
- Lined by non-keratinized stratified squamous epithelium
- Produces no digestive enzymes — purely transport
- Peristalsis (primary and secondary) drives bolus to stomach
5. STOMACH
Anatomy
Four regions: cardia, fundus, body (corpus), antrum/pylorus
Gastric glands differ by region:
- Corpus/fundus: Parietal cells + chief cells + ECL cells + mucus neck cells
- Antrum: G cells (gastrin) + D cells (somatostatin) — no parietal cells
Cell Types and Secretions
| Cell | Location | Product | Function |
|---|---|---|---|
| Parietal (oxyntic) | Corpus | HCl + Intrinsic factor | Acid digestion; B₁₂ absorption |
| Chief (peptic) | Corpus | Pepsinogen | Activated to pepsin at pH <3; protein digestion |
| G cells | Antrum | Gastrin | Stimulates parietal cells and ECL cells |
| D cells | Antrum + corpus | Somatostatin | Inhibits gastrin release and acid secretion |
| ECL cells | Corpus | Histamine | Potent stimulator of parietal cells (H₂ receptor) |
| Mucus cells | Neck of glands | HCO₃⁻ + Mucus | Protects gastric wall |
Gastric Acid Secretion
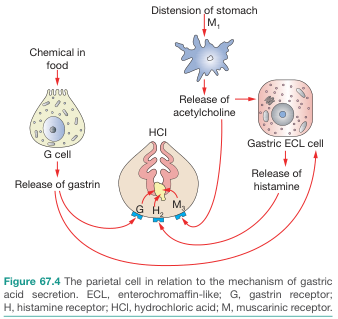
Three convergent stimuli activate the parietal cell's H⁺/K⁺-ATPase (proton pump):
- Gastrin → G receptor on parietal cell + ECL cell → ↑Ca²⁺ signaling
- Histamine → H₂ receptor on parietal cell → ↑cAMP → activates proton pump
- Acetylcholine (vagal) → M₃ receptor → ↑Ca²⁺ signaling
Pepsins are endopeptidases activated from pepsinogens at pH <3 and initiate protein digestion by hydrolyzing interior peptide bonds. A low gastric pH also limits bacterial colonization of the small intestine. — Medical Physiology
Gastric Motor Functions
- Receiving food (receptive relaxation of fundus — VIP-mediated)
- Mixing (antral contractions grind food into chyme)
- Grinding (retrograde peristalsis)
- Emptying through pylorus into duodenum (regulated by duodenal feedback — CCK, secretin slow emptying)
6. PANCREAS
Exocrine Pancreas
The pancreas secretes ~1.5 L/day of alkaline juice (pH 8.0–8.3) via the duct of Wirsung into the duodenum. Key enzymes:
| Enzyme | Substrate | Activation |
|---|---|---|
| Trypsinogen → Trypsin | Proteins (endopeptidase) | Activated by enterokinase (duodenal brush border) |
| Chymotrypsinogen → Chymotrypsin | Proteins | Activated by trypsin |
| Proelastase → Elastase | Elastin/proteins | Activated by trypsin |
| Pancreatic amylase | Starch → maltose | Secreted in active form |
| Pancreatic lipase | Triglycerides → fatty acids + 2-monoglyceride | Requires colipase + bile salts |
| Phospholipase A₂ | Phospholipids | Activated by trypsin |
| Cholesterol esterase | Cholesterol esters | Active form |
Bicarbonate (from ductal cells) neutralizes gastric acid entering the duodenum, creating the optimal pH for enzyme activity.
Hormonal regulation:
- Secretin (from S cells of duodenum, triggered by acid): stimulates bicarbonate-rich pancreatic secretion
- CCK (from I cells, triggered by fats and proteins): stimulates enzyme-rich secretion
Endocrine Pancreas (Islets of Langerhans)
- α cells → Glucagon
- β cells → Insulin
- δ cells → Somatostatin
7. LIVER AND GALLBLADDER
Liver
The liver is the largest gland (~1.5 kg), with dual blood supply: hepatic artery (25%) + portal vein (75%).
Digestive function — Bile production:
- Hepatocytes produce ~600–1000 mL bile/day
- Primary bile acids: cholic acid and chenodeoxycholic acid (conjugated with glycine or taurine → bile salts)
- Bile salts emulsify dietary fats → form micelles → dramatically increase surface area for lipase action
- Bile also contains: bilirubin, cholesterol, phospholipids, water, ions
Other liver functions (non-digestive): glucose metabolism (glycogenesis/gluconeogenesis), protein synthesis (albumin, clotting factors), drug metabolism (CYP450), immune function (Kupffer cells).
Gallbladder
- Stores and concentrates bile (10× concentration by absorbing water and electrolytes)
- Contraction triggered by CCK (released when fat/protein enters the duodenum)
- Bile is released via common bile duct → ampulla of Vater → duodenum
- Sphincter of Oddi regulates flow into the duodenum
8. SMALL INTESTINE
Longest segment (~6–7 m). Three regions: duodenum → jejunum → ileum
Anatomical Adaptations for Absorption
Surface area is amplified ~600-fold by three structural features:
- Plicae circulares (circular folds) — permanent mucosal folds
- Villi — finger-like projections of mucosa (~1 mm tall)
- Microvilli (brush border) — on each enterocyte, expressing digestive enzymes
Brush border enzymes: lactase, sucrase-isomaltase, maltase, peptidases, alkaline phosphatase
Duodenum
- Receives chyme + pancreatic juice + bile
- Brunner's glands secrete alkaline mucus (protects from acid)
- Site of iron absorption and calcium absorption
Jejunum
- Principal site for absorption of most nutrients (carbohydrates, proteins, fats, fat-soluble vitamins)
- High density of villi
Ileum
- Absorbs vitamin B₁₂–intrinsic factor complex (specific receptor: cubam)
- Bile salt reabsorption (enterohepatic circulation — ~95% recycled)
- Contains Peyer's patches (lymphoid tissue, immune surveillance)
Intestinal Motility
- Segmentation contractions: mixing
- Peristalsis: propulsion
- Migrating motor complex (MMC): housekeeping between meals
9. LARGE INTESTINE
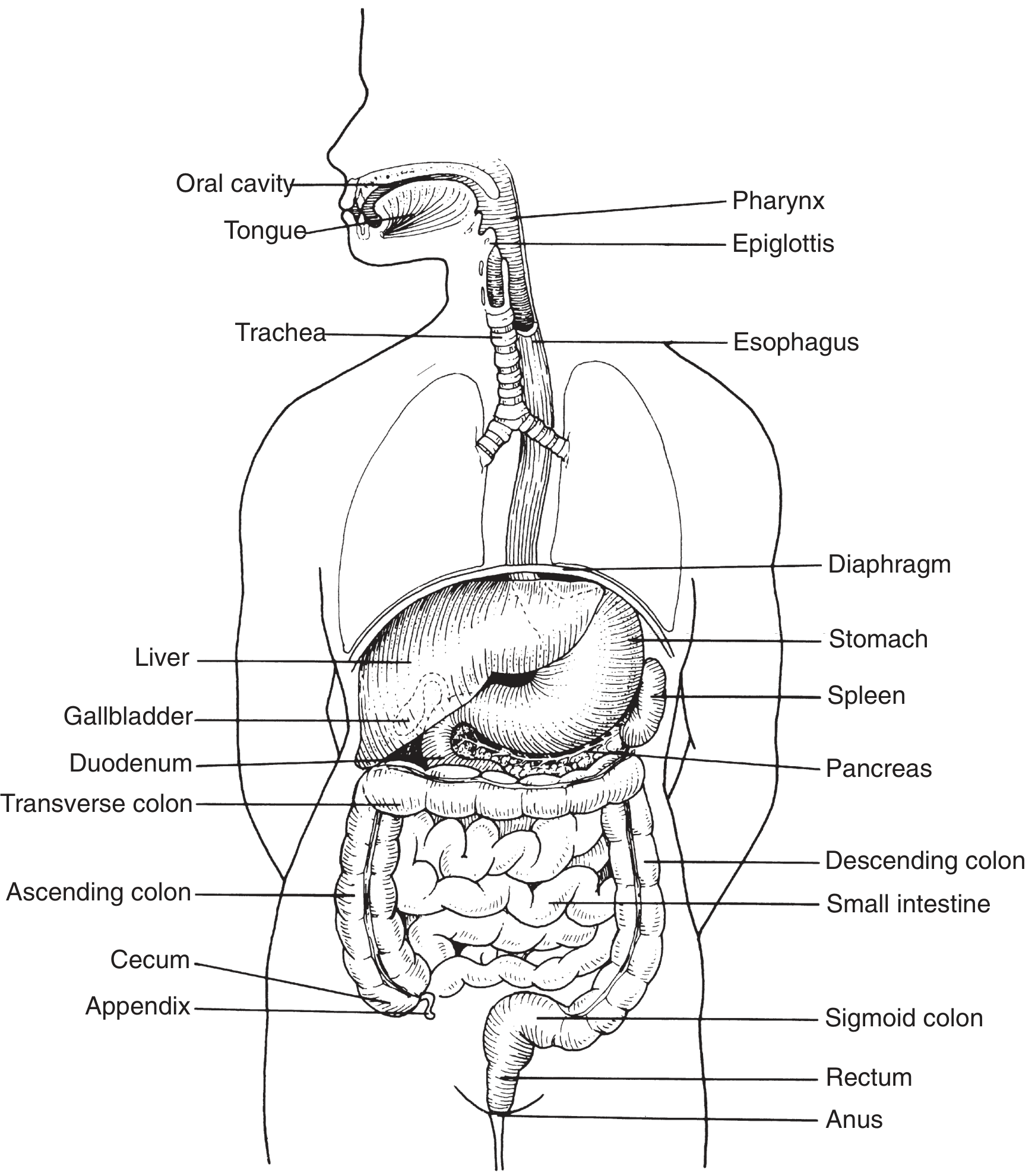
Length ~1.5 m. Regions: cecum → ascending colon → transverse colon → descending colon → sigmoid colon → rectum → anal canal
Functions
- Water and electrolyte absorption (~1.5 L/day absorbed; only ~100–200 mL excreted in feces)
- Na⁺ absorption mechanisms (Medical Physiology):
- Nutrient-coupled (jejunum/ileum)
- Electroneutral NaCl absorption via parallel Na-H/Cl-HCO₃ exchangers (ileum + proximal colon)
- Electrogenic Na⁺ absorption via ENaC (distal colon — aldosterone-regulated; key in Na⁺ conservation)
- Fermentation of undigested carbohydrates by colonic bacteria → short-chain fatty acids (SCFAs), gases (CO₂, H₂, CH₄)
- Feces formation: bacteria, sloughed epithelial cells, undigested material, water
The Appendix
A lymphoid organ attached to the cecum; functionless in digestion but contains immune tissue.
10. PHASES OF DIGESTION
| Phase | Trigger | Effects |
|---|---|---|
| Cephalic phase | Sight, smell, thought of food → hypothalamus/cortex → vagus nerve | ↑saliva, ↑gastric acid & pepsinogen, ↑gastric motility (~30% of total acid response) |
| Gastric phase | Food in stomach → distension + peptides/amino acids → G cells | ↑gastrin → ↑HCl, ↑pepsin, ↑gastric motility (~60% of acid response) |
| Intestinal phase | Chyme enters duodenum → CCK, secretin, GIP released | ↑pancreatic enzymes & bile (CCK); ↑bicarbonate (secretin); ↓gastric emptying (CCK + secretin = enterogastric reflex) |
Gastric Inhibition: When acidic chyme enters the duodenum → secretin inhibits gastrin + stimulates bicarbonate. Fat in duodenum → CCK slows gastric emptying. GIP (gastric inhibitory peptide) stimulates insulin release.
11. MECHANICAL DIGESTION
| Location | Process | Mechanism |
|---|---|---|
| Mouth | Mastication | Jaw muscles (CN V); grinding + cutting; ↑surface area |
| Esophagus | Peristalsis | Coordinated smooth/striated muscle contraction |
| Stomach | Mixing waves + retropulsion | Antral grinding → chyme formation |
| Small intestine | Segmentation + peristalsis | Haustral movements mix with enzymes |
| Large intestine | Haustrations + mass movements | Mass peristalsis (1–3×/day, often postprandial) |
12. CHEMICAL DIGESTION
Carbohydrates
- Mouth: salivary amylase → maltose + dextrins
- Small intestine: pancreatic amylase → disaccharides; brush border enzymes (maltase, sucrase, lactase) → monosaccharides (glucose, fructose, galactose)
Proteins
- Stomach: pepsin (endopeptidase) begins denaturation and cleavage
- Small intestine: trypsin, chymotrypsin, elastase (endopeptidases) + carboxypeptidase A/B (exopeptidases) → dipeptides/tripeptides + amino acids; brush border peptidases → free amino acids
Fats
- Mouth/stomach: lingual + gastric lipase (minor)
- Small intestine: bile salts emulsify → pancreatic lipase + colipase → fatty acids + 2-monoglycerides → incorporate into micelles → absorbed by enterocytes → re-esterified into triglycerides → packaged into chylomicrons → secreted into lymph (lacteals)
Nucleic Acids
- Pancreatic DNase and RNase → nucleotides
- Brush border nucleotidases + nucleosidases → bases + sugars + phosphate
13. ABSORPTION OF NUTRIENTS
| Nutrient | Primary Site | Mechanism |
|---|---|---|
| Glucose, galactose | Jejunum | SGLT1 (secondary active, Na⁺-coupled) apical; GLUT2 basolateral |
| Fructose | Jejunum | GLUT5 apical; GLUT2 basolateral |
| Amino acids | Jejunum | Na⁺-coupled transporters (multiple families) |
| Fats (LCFAs) | Jejunum | Micelle → passive diffusion into enterocyte → chylomicron → lacteals |
| Medium-chain fatty acids | Small intestine | Direct portal absorption (no chylomicron needed) |
| Fat-soluble vitamins (A, D, E, K) | Small intestine | Bile salt-dependent micelle absorption |
| Vitamin B₁₂ | Terminal ileum | Intrinsic factor–cubam receptor complex |
| Folate | Jejunum | Carrier-mediated |
| Iron (Fe²⁺) | Duodenum | DMT-1 (divalent metal transporter); ferroportin basolateral |
| Calcium | Duodenum | Vitamin D–dependent (calbindin-D); passive in ileum/colon |
| Water | Small + large intestine | Osmotic gradient following solute absorption |
| Bile salts | Terminal ileum | Active transport (ASBT) → enterohepatic circulation |
14. DISORDERS
14.1 Gastroesophageal Reflux Disease (GERD)
Pathophysiology: Inappropriate relaxation or reduced resting tone of the LES allows reflux of gastric acid into the esophagus. Predisposing factors: hiatal hernia, obesity, smoking, pregnancy, medications (calcium channel blockers, nitrates). — Ganong's Review; Medical Physiology
Symptoms: Heartburn, regurgitation, dysphagia, hoarseness (atypical), chronic cough
Complications: Erosive esophagitis → Barrett's esophagus (columnar metaplasia → ↑risk of adenocarcinoma)
Treatment (Rosen's Emergency Medicine):
| Agent | Mechanism | Example |
|---|---|---|
| PPIs (first-line) | Irreversibly block H⁺/K⁺-ATPase | Omeprazole 20 mg qd, Pantoprazole 40 mg qd |
| H₂ receptor antagonists | Block H₂ receptors on parietal cells | Famotidine 20–40 mg bid |
| Sucralfate | Mucosal protectant | 1 g q6h (adjunct) |
| Antacids | Neutralize HCl | PRN symptom relief |
Lifestyle: weight loss and head-of-bed elevation have the best evidence; also avoid caffeine, alcohol, chocolate, fatty foods, late meals.
14.2 Peptic Ulcer Disease (PUD)
Definition: Mucosal defect penetrating through the muscularis mucosae, most commonly in duodenum (D1) and stomach (lesser curvature).
Etiology:
- H. pylori infection (~70–90% of duodenal ulcers; ~60–70% of gastric ulcers) — urease → ammonia → mucosal damage; disrupts protective mucus layer; upregulates gastrin
- NSAIDs — inhibit COX-1 → ↓prostaglandin synthesis → ↓mucus/bicarbonate secretion + ↓mucosal blood flow
- Zollinger-Ellison syndrome — gastrin-secreting tumor → massive acid hypersecretion
Pathophysiology: Imbalance between aggressive factors (acid, pepsin, H. pylori, NSAIDs) and defensive factors (mucus, bicarbonate, prostaglandins, mucosal blood flow).
Symptoms: Epigastric pain — classically burning, worse 2–3 hours after meals (duodenal) or worse immediately after eating (gastric); nausea, bloating. May be asymptomatic until complication (bleeding, perforation).
Diagnosis: Endoscopy (gold standard); H. pylori: ¹³C-urea breath test, stool antigen, rapid urease test, serology.
Treatment:
- H. pylori eradication: Triple therapy — PPI + clarithromycin + amoxicillin (×14 days); or bismuth quadruple therapy
- NSAID ulcers: stop NSAID + PPI (4–8 weeks); misoprostol for prevention
- Complications: surgical intervention for perforation, uncontrolled bleeding
14.3 Celiac Disease
Definition: Immune-mediated enteropathy triggered by dietary gluten (gliadin fraction of wheat, rye, barley) in genetically predisposed individuals. — Henry's Clinical Diagnosis; Robbins Pathology
Genetics: Nearly all patients carry HLA-DQ2 or HLA-DQ8 haplotypes (necessary but not sufficient).
Pathophysiology:
- Tissue transglutaminase (tTG) deamidates gliadin peptides
- Deamidated gliadin is presented by HLA-DQ2/DQ8 on antigen-presenting cells to CD4⁺ T cells
- Cytokine release → CD8⁺ T-cell activation → epithelial damage
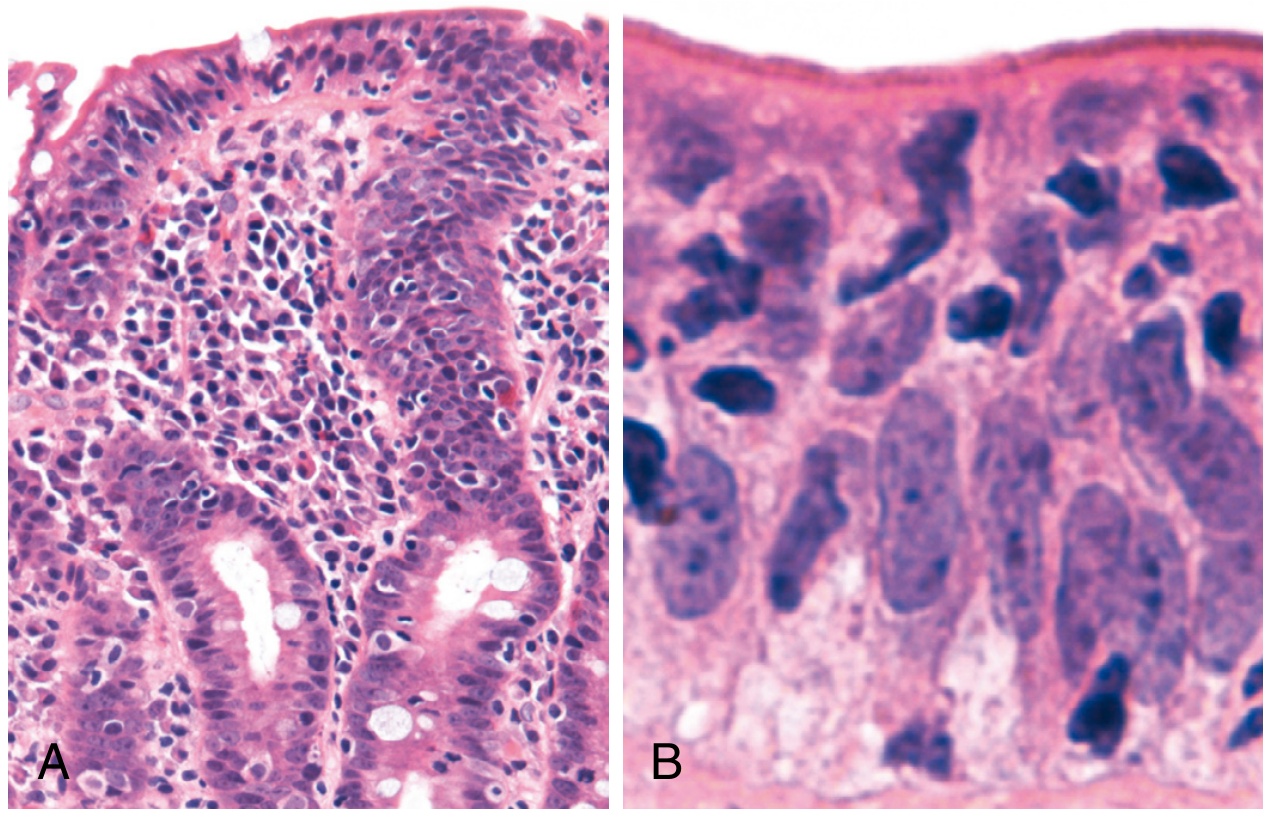
- Result: villous atrophy + crypt hyperplasia + increased intraepithelial lymphocytes (IELs)
- Loss of villous surface area → malabsorption
Clinical Features:
- Classic: chronic diarrhea, steatorrhea, weight loss, abdominal bloating, failure to thrive (children)
- Atypical: iron deficiency anemia, osteoporosis, infertility, dermatitis herpetiformis (10%), neurological symptoms
- Silent: positive serology + villous atrophy, no symptoms
- Associations: type 1 DM, Down syndrome, Turner syndrome, IgA deficiency, autoimmune thyroid disease
- Worldwide prevalence ~1%; women 2–3× more affected than men
Diagnosis:
- Serology: anti-tTG IgA (most sensitive/specific); anti-endomysial (EMA-IgA); anti-deamidated gliadin (DGP) IgG if IgA-deficient
- Duodenal biopsy: gold standard — villous atrophy, crypt hyperplasia, ↑IELs (Marsh classification)
- HLA typing: DQ2/DQ8 (high negative predictive value — rules out disease if absent)
Treatment: Lifelong strict gluten-free diet — resolution of symptoms and histological recovery (months to years). Monitoring: repeat anti-tTG titres to assess dietary compliance.
Deficiencies to supplement: iron, folate, vitamin D, calcium, vitamin B₁₂, zinc.
Summary: The Digestive Tract at a Glance
Mouth → Pharynx → Esophagus → Stomach → Duodenum → Jejunum → Ileum → Colon → Rectum → Anus
↓ ↓ ↓ ↓ ↓ ↓ ↓ ↓
Amylase Swallowing Peristalsis HCl Bile + Main B₁₂/ Water/
Lipase reflex LES Pepsin Pancreatic nutrient Bile salt electrolyte
(mech) (medulla) Gastrin enzymes absorption absorption absorption
Sources: Guyton & Hall Textbook of Medical Physiology | Medical Physiology (Boron & Boulpaep) | Ganong's Review of Medical Physiology, 26th Ed. | Robbins & Cotran Pathologic Basis of Disease | Henry's Clinical Diagnosis & Management | Rosen's Emergency Medicine | Goodman & Gilman's Pharmacological Basis of Therapeutics | Bailey & Love's Short Practice of Surgery, 28th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.