Endometriosis
Reading File
Finding Sources
Searching Images
endometriosis pelvis laparoscopy lesions
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of endometriosis based on authoritative medical textbooks.
Endometriosis
Definition
Endometriosis is defined by the presence of endometrial glands and stroma in locations outside the uterus. It affects approximately 10% of women in their reproductive years and nearly 50% of women with infertility.
Types
There are three recognized forms:
- Superficial peritoneal endometriosis — implants on the peritoneal surface
- Ovarian endometriosis — forms endometriomas ("chocolate cysts")
- Deep infiltrating endometriosis (DIE) — the form with the highest risk of malignant transformation
Pathogenesis
The exact mechanism remains elusive, but four leading theories exist:
| Theory | Mechanism |
|---|---|
| Regurgitation (Sampson's) | Retrograde menstrual flow implants endometrial tissue at ectopic pelvic sites via the fallopian tubes |
| Benign metastasis | Endometrial tissue spreads to distant sites (bone, lung, brain) via blood/lymphatics |
| Metaplastic | Coelomic epithelium (mesothelium) undergoes metaplasia into endometrial tissue — explains cases in men or pre-menarchal girls |
| Stem/progenitor cell | Bone marrow stem cells differentiate into endometrial tissue at ectopic sites |
Why implants persist — molecular mechanisms
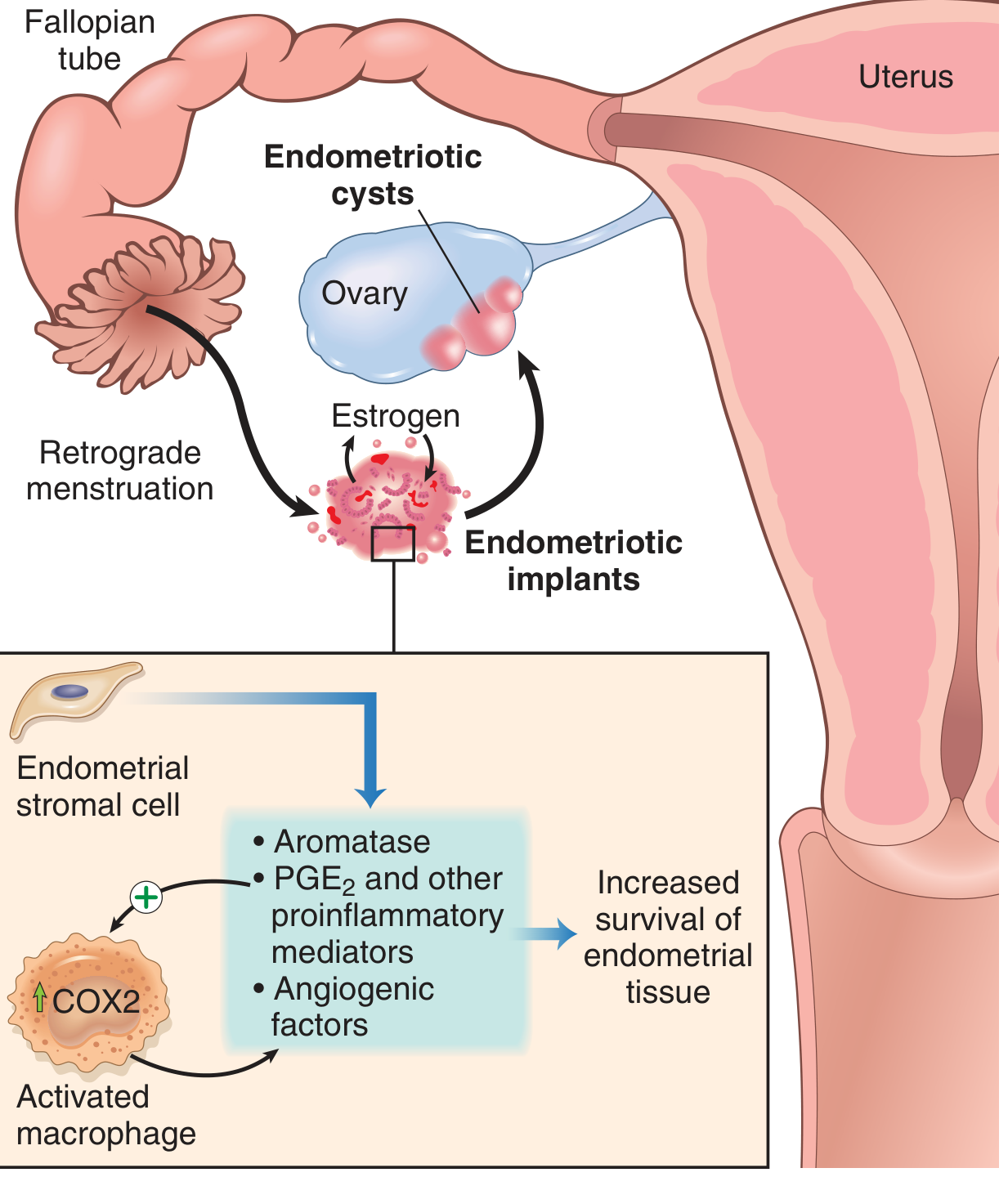
Endometriotic implants are not simply "misplaced" endometrium — they are metabolically distinct:
- Aromatase overexpression → local estrogen production from androgens
- Elevated PGE₂, VEGF, and MMPs (partly from recruited macrophages) → promotes inflammation and angiogenesis
- This creates a self-sustaining estrogen-rich microenvironment that favors implant survival
Morphology
- Grossly: red-brown nodules on serosal surfaces (1 mm to 1–2 cm), representing sites of cyclic bleeding
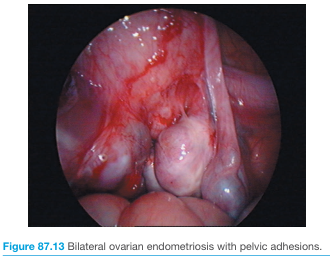
- Extensive disease → fibrous adhesions between tubes, ovaries, and surrounding structures; obliteration of the pouch of Douglas
- Endometriomas ("chocolate cysts"): cystic ovarian masses (3–5 cm) filled with old brown blood
- Microscopically: diagnosis requires both endometrial glands AND stroma at ectopic sites
Laparoscopic appearance
Common Sites of Involvement
- Pelvic (most frequent): ovaries, pouch of Douglas, uterosacral ligaments, fallopian tubes
- Gastrointestinal: 12–37% of cases; sigmoid colon and small bowel most common; caecum also affected
- Serosal implants invade the muscularis propria → fibrosis, wall contraction, mass effect
- Mucosal surface remains intact but rectal bleeding may occur
- Extra-pelvic (rare): periumbilical tissue, laparotomy scars, lung, pleura, bone, brain
Clinical Features
| Feature | Details |
|---|---|
| Dysmenorrhea | Severe; hallmark symptom due to intrapelvic bleeding |
| Dyspareunia | Deep pain during intercourse |
| Chronic pelvic pain | Persistent; from adhesions and peritoneal inflammation |
| Menstrual irregularities | Common |
| Infertility | Presenting complaint in 30–40% of patients |
Diagnosis
- Clinical suspicion based on symptoms (especially the triad of dysmenorrhea, dyspareunia, pelvic pain)
- Laparoscopy — gold standard; allows direct visualization and biopsy of implants
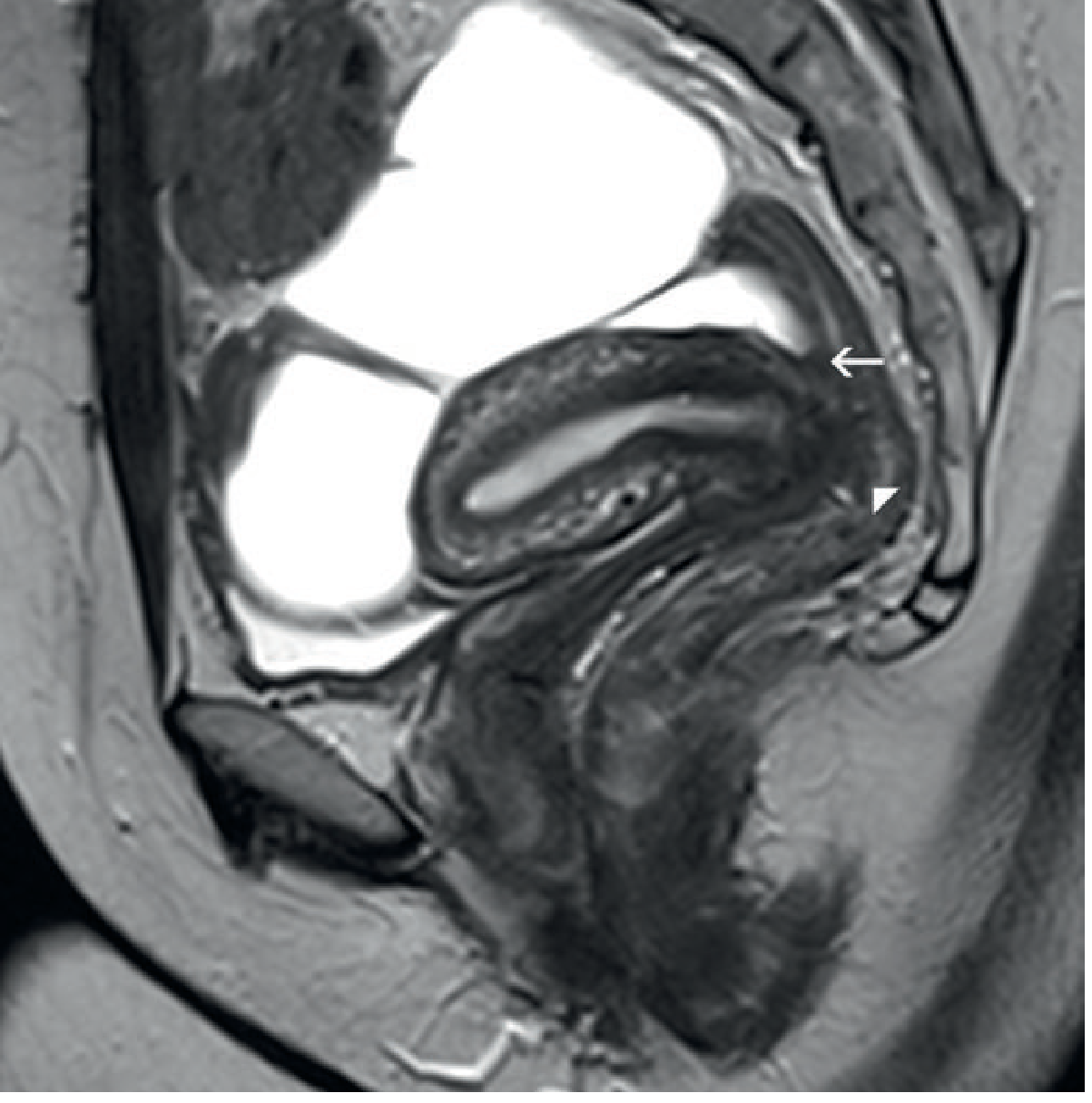
- MRI — preferred cross-sectional imaging; demonstrates low-signal fibrotic plaques, rectovaginal nodules, and pouch of Douglas obliteration on T2-weighted sequences
- Transvaginal ultrasound — can identify endometriomas and, with expertise, superficial implants ("honeycomb" appearance with pocket/hat signs on peritoneal surfaces)
MRI of deep infiltrating endometriosis
Treatment
| Category | Options |
|---|---|
| Medical | NSAIDs/COX-2 inhibitors (pain), aromatase inhibitors (reduce local estrogen), GnRH agonists/antagonists, combined oral contraceptives, progestins |
| Surgical | Laparoscopic excision or ablation of implants; adhesiolysis; cystectomy for endometriomas; nerve-sparing deep excision for DIE |
Malignant Transformation
Although uncommon, malignancy can develop within endometriotic tissue. Risk is mainly confined to deep infiltrating endometriosis. Endometriosis-associated ovarian cancers are primarily clear cell and endometrioid histotypes.
Sources: Robbins & Kumar Basic Pathology; Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.