
PXL_20260520_023808801~2.jpg
I am an ENT resident posted in OT. This is the diagnosis and procedure planned for today. Walk me through the diagnosis including findings, what it is and whatever a consultant might ask me. Then the procedure, begin with anatomy, physiology instruments investigation and step by step brief on the procedure
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Here is your complete OT briefing for today.
SCC Right Lateral Border of Tongue + Wide Local Excision + Neck Dissection
PART 1 — THE DIAGNOSIS
What Is It?
Squamous cell carcinoma (SCC) of the oral tongue — the most common malignancy of the oral cavity. The oral tongue (anterior 2/3, anterior to the circumvallate papillae) is the second most common site of oral cancer (~30%), and the lateral border is the most frequent subsite within the tongue. This patient has a right-sided lesion.
Clinical Findings — What You Will See / Have Seen
| Feature | Detail |
|---|---|
| Appearance | Indurated, ulcerated, exophytic mass on the lateral border — often with raised, everted edges and central necrosis |
| Palpation | Hard, fixed base — induration extending beyond visible margins is pathognomonic |
| Early lesion | Erythroplakia (red velvety patch) — most common early SCC presentation; leukoplakia is a precursor |
| Late features | Tongue fixation (invasion of intrinsic/extrinsic muscles), trismus, referred otalgia (via CN V3/lingual n.), dysphagia, altered speech, cervical lymphadenopathy |
| Neck | Palpate ipsilateral levels I–III; tongue SCC can also skip to level IV |
Depth of invasion (DOI) >2–4 mm = higher rate of regional metastasis and mortality. DOI is the single most critical prognostic pathological parameter.
Aetiology & Risk Factors
- Tobacco (smoking + smokeless) + alcohol (synergistic)
- Poor oral hygiene, chronic dental trauma/irritation
- Immunosuppression
- Increasing incidence in young patients with no identifiable risk factors — postulated genetic susceptibility
- HPV-negative oral tongue SCC — TP53 (83%) and CDKN2A (57%) mutations dominate (unlike HPV+ oropharyngeal SCC which is TP53 wild-type)
Investigations
Tissue diagnosis first:
- Incisional biopsy of the lesion (most tongue lesions are biopsy-able in the office/OPD)
Staging workup:
| Investigation | Purpose |
|---|---|
| CT neck with contrast | Node assessment, bone involvement, primary extent |
| MRI tongue/floor of mouth | Best for DOI assessment, perineural spread, soft tissue extent |
| CT chest | Exclude pulmonary metastases and synchronous primary |
| PET-CT | Used in locally advanced disease or nodal uncertainty |
| EUA (Examination Under Anaesthesia) | When full extent cannot be assessed in clinic; combined with biopsy |
| Orthopantomogram (OPG) | Mandibular involvement assessment |
| Panendoscopy | Rule out synchronous primaries (incidence 2.4–4.5%) |
AJCC 8th Edition TNM Staging (Oral Cavity — Know This Cold)
The 8th edition introduced DOI into T staging — a major change from prior editions.
| T Stage | Criteria |
|---|---|
| T1 | Tumour ≤2 cm, DOI ≤5 mm |
| T2 | Tumour ≤2 cm with DOI >5–10 mm OR tumour >2–4 cm with DOI ≤10 mm |
| T3 | Tumour >4 cm OR any tumour with DOI >10 mm |
| T4a | Moderately advanced — cortical bone, deep tongue muscles, skin of face |
| T4b | Very advanced — masticator space, pterygoid plates, skull base, ICA |
N staging now includes extranodal extension (ENE):
- N1: Single ipsilateral node ≤3 cm, no ENE
- N2a: Single ipsilateral node 3–6 cm, no ENE
- N2b: Multiple ipsilateral nodes ≤6 cm, no ENE
- N2c: Bilateral/contralateral nodes ≤6 cm, no ENE
- N3b: Any node with clinical ENE
Histopathological Prognostic Factors (What the Path Report Will Say)
- DOI — most important for staging and nodal risk
- Tumour grade — well (G1), moderate (G2), poorly differentiated (G3); poorly differentiated = more aggressive
- Pattern of invasion — cohesive vs. non-cohesive advancing front; non-cohesive = worse
- Perineural invasion (PNI) — independent risk factor for cervical metastasis, local recurrence
- Lymphovascular invasion (LVI)
- Bone invasion — cortical erosion alone ≠ T4; medullary invasion = T4a
- Resection margins — clear (>5 mm), close (1–5 mm), involved (<1 mm). Close/involved margins → adjuvant RT
Consultant's Questions — Be Ready For These
- What is the most common site for SCC within the tongue? → Lateral border
- Why does lateral border tongue SCC carry a poor prognosis? → Rich lymphatic drainage, early occult nodal spread, proximity to deep muscles and floor of mouth
- What is DOI and why does it matter? → Depth of invasion from basement membrane of adjacent normal mucosa to deepest tumour point; >4 mm → risk of nodal mets doubles; determines T stage in 8th AJCC
- What is the incidence of occult nodal metastasis in clinically N0 oral tongue SCC? → 20–25%; justifies elective neck dissection
- What is a skip metastasis? → Direct spread to level III or IV bypassing levels I and II — more common with oral tongue
- Which neck levels drain the oral tongue? → Levels I, II, III (level IV also at risk for tongue SCC — skip metastasis)
- What is the significance of ENE? → Extranodal extension — breach of lymph node capsule; independent predictor of disease-specific survival; now upstages N disease in AJCC 8th
- What are indications for postoperative radiotherapy? → Involved/close margins, PNI, LVI, bone invasion, ENE, ≥2 positive nodes, N2–N3 disease
- What is erythroplakia? → Red velvety mucosal lesion with highest malignant transformation rate (~50%) — more dangerous than leukoplakia
- What is the management of mandibular involvement? → Periosteal invasion → marginal mandibulectomy; medullary invasion → segmental resection
PART 2 — THE PROCEDURES
PROCEDURE A: Wide Local Excision of the Right Lateral Border of Tongue (Partial Glossectomy)
Anatomy of the Tongue
Boundaries of the oral tongue (mobile tongue):
- Anterior 2/3, separated from base (posterior 1/3) by the circumvallate papillae
- Lateral border = where most SCCs arise
Muscles — Intrinsic (change shape, no bony attachment):
- Superior longitudinal, inferior longitudinal, transverse, vertical
Muscles — Extrinsic (change position, all insert into tongue):
| Muscle | Origin | Action | Nerve |
|---|---|---|---|
| Genioglossus | Mental spine of mandible | Protrudes tongue | CN XII |
| Hyoglossus | Hyoid | Depresses tongue | CN XII |
| Styloglossus | Styloid process | Retracts, elevates | CN XII |
| Palatoglossus | Palatine aponeurosis | Elevates posterior tongue | CN X |
Nerve Supply:
- Sensation, anterior 2/3: Lingual nerve (branch of V3)
- Taste, anterior 2/3: Chorda tympani (CN VII) via lingual nerve
- Sensation + taste, posterior 1/3: CN IX (glossopharyngeal)
- Motor (all muscles except palatoglossus): CN XII (hypoglossal)
Arterial supply: Lingual artery (branch of external carotid), runs deep to hyoglossus
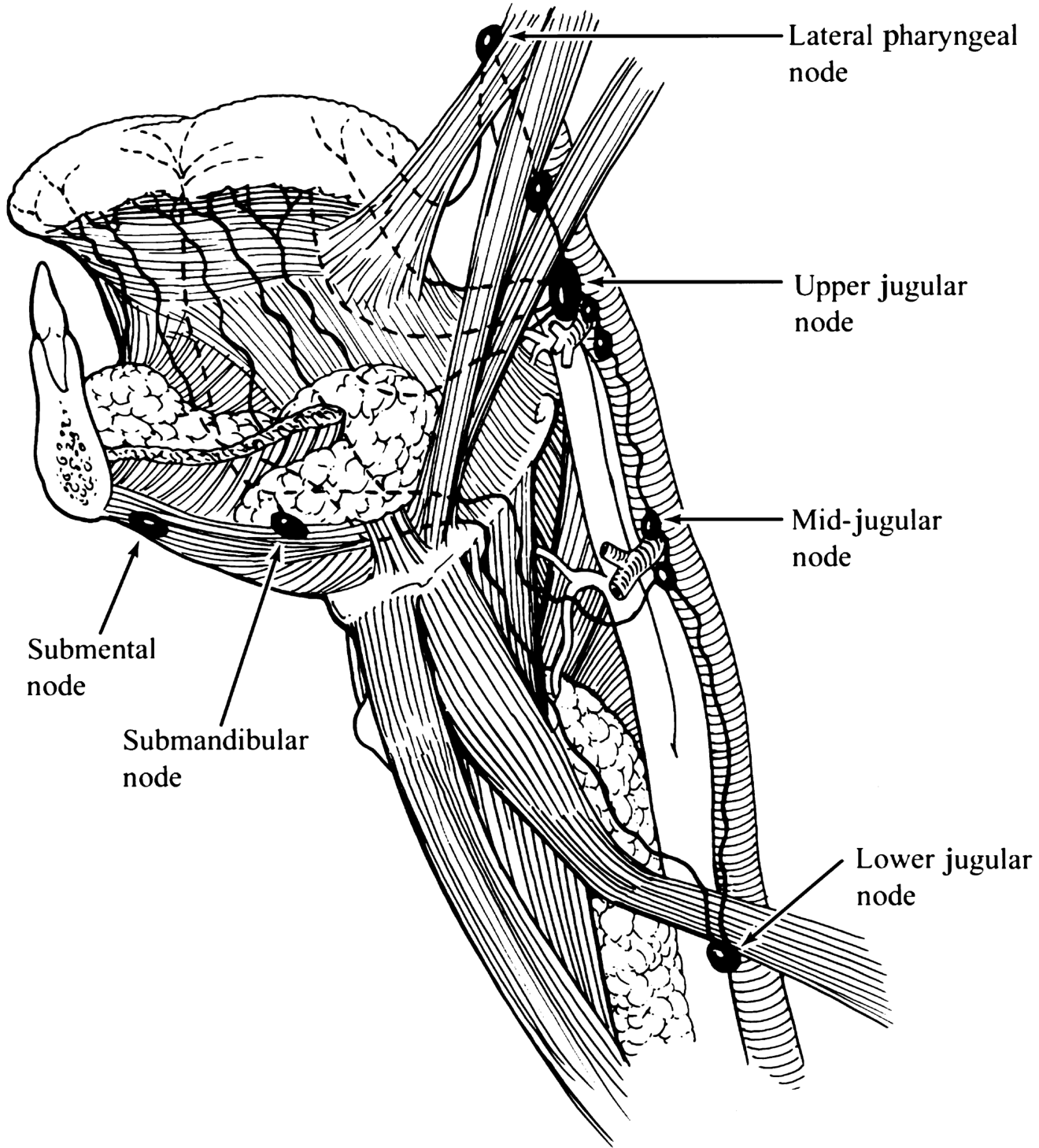
Lymphatics: Rich submucosal plexus → submental → submandibular → upper/mid jugular chain (levels I–III, and skip to IV)
Instruments for Wide Local Excision
- Blade 15 / 10 scalpel
- Mouth gag (Dingman or Boyle Davis) for exposure
- Self-retaining tongue sutures (2-0 silk stay sutures in tongue tip)
- Needle holders, tissue forceps, scissors
- Bipolar or monopolar cautery
- Diathermy loop / CO₂ laser (in some centres)
- Vessel loops / Lahey swabs
- Measuring rule (for margin marking)
- Specimen orientation suture/marking inks
Wide Local Excision — Step by Step
Pre-op setup:
- General anaesthesia — nasoendotracheal intubation (keeps mouth free)
- Patient supine, head ring, shoulder roll for neck extension
- Mouth gag inserted for exposure
Steps:
-
Mark the tumour margins — minimum 1 cm clear margin marked around the visible/palpable tumour edges with a marking pen. Frozen section margin control is performed intraoperatively.
-
Stay sutures — 2-0 silk sutures placed through the tongue tip and lateral tongue to provide traction and improve visualisation.
-
Incision — Full-thickness elliptical incision through mucosa, submucosa, and underlying muscle using blade 15 or electrocautery. The cut is made in continuity, not piecemeal.
-
Deep margin — Resection extends down through intrinsic and, if needed, extrinsic tongue muscle (hyoglossus). The lingual artery lies deep — careful haemostasis required. Suture ligation of the lingual vessels if they are encountered.
-
Orientation of specimen — Suture/ink specimen immediately (e.g., long stitch = superior, short = anterior). Send for frozen section (margins) and formal histopathology (DOI, grade, PNI, LVI).
-
Hemostasis — Bipolar cautery / suture ligation. The tongue is highly vascular.
-
Reconstruction / closure:
- Small defects (<1/3 tongue): Primary closure with absorbable sutures (3-0 Vicryl) — best functional outcome
- Moderate defects: Secondary intention (floor of mouth) or split-thickness skin graft
- Large defects (>1/2 tongue): Radial forearm free flap (RFFF) or anterolateral thigh (ALT) flap
PROCEDURE B: Neck Dissection
Anatomy of the Neck Levels (AHNS Classification)
| Level | Contents | Anatomical Boundaries |
|---|---|---|
| IA | Submental nodes | Between anterior bellies of digastric |
| IB | Submandibular nodes | Submandibular triangle |
| IIA | Upper jugular (above SAN) | Skull base to hyoid; anterior to SAN |
| IIB | Upper jugular (below/posterior to SAN) | Posterior to SAN |
| III | Mid-jugular | Hyoid to lower border of cricoid |
| IV | Lower jugular | Cricoid to clavicle |
| V | Posterior triangle | Posterior to SCM, anterior to trapezius |
| VI | Central compartment | Hyoid to sternal notch, carotid to carotid |
For oral tongue SCC → Supraomohyoid ND = Levels I–III (elective, N0). Add Level IV for tongue SCC (skip risk). Node-positive → Modified Radical ND (I–V preserving CN XI, IJV, SCM).
Key Structures to Protect
| Structure | Level / Location | Risk |
|---|---|---|
| CN XI (Spinal accessory n.) | Enters SCM, traverses posterior triangle | Shoulder drop if injured |
| CN XII (Hypoglossal n.) | Loops below digastric | Tongue deviation, dysarthria |
| Marginal mandibular branch (CN VII) | In superficial layer of deep cervical fascia | Lip droop |
| Internal jugular vein (IJV) | In carotid sheath | Haemorrhage |
| Common / internal carotid artery | Carotid sheath | Catastrophic haemorrhage |
| Phrenic nerve | On anterior scalene muscle | Hemidiaphragm paralysis |
| Vagus nerve (CN X) | In carotid sheath (posterior) | Vocal cord palsy |
| Thoracic duct | Left neck, level IV–V junction | Chylous fistula |
| Lingual nerve | Near submandibular gland | Tongue sensation loss |
Neck Dissection Types — Know the Classification
- Radical ND (RND): Removes levels I–V + SCM + IJV + CN XI → rarely done now
- Modified Radical ND (MRND): Levels I–V, preserves one or more of (SCM, IJV, CN XI) — Type I: preserves CN XI; Type II: preserves CN XI + IJV; Type III: all three preserved
- Selective ND (SND): Only at-risk levels. For oral tongue: Supraomohyoid ND = Levels I–III (add IV for tongue)
- Extended ND: Standard + additional structures (e.g. parotid, retropharyngeal nodes)
Neck Dissection — Step by Step (Supraomohyoid / Selective I–IV for Tongue SCC)
Position & Prep:
- Supine, head ring, shoulder roll
- Head turned contralateral to dissection side
- Prep and drape neck
Incision:
- Modified apron incision (MacFee/hockey-stick) — 2 cm below mandible, extending posteriorly toward mastoid tip
- Skin flaps raised in subplatysmal plane — preserve greater auricular nerve and external jugular vein posteriorly
Steps:
-
Raise subplatysmal flaps — superiorly to mandible, inferiorly to clavicle (if extended). Identify and protect the marginal mandibular nerve in the superficial layer of deep cervical fascia over the submandibular gland.
-
Open investing fascia at anterior border of SCM. Dissect fibrofatty contents away from SCM medially.
-
Identify CN XI (SAN) — enters SCM posteriorly; dissect free from skull base to SCM entry. This delineates the superior border of Level IIB.
-
Level II dissection — Triangular packet bounded by posterior belly of digastric (superior), SAN (posterior), and SCM (lateral). Pass tissue packet under the SAN to protect it.
-
Levels III and IV — Sweep fibrofatty tissue inferiorly. The phrenic nerve lies on the anterior scalene (deep to prevertebral fascia — do not breach). The sensory branches of cervical plexus can be preserved in SND (not Level V dissection).
-
Level I dissection (submandibular triangle):
- Skeletonise the inferior border of the mandible
- Identify and ligate the facial artery and vein (retromandibular)
- Identify lingual nerve and CN XII entering submandibular region
- Excise submandibular gland if indicated (or separate it from the nodal specimen)
- Protect the marginal mandibular branch throughout
-
Medial sweep — All fibrofatty tissue swept medially over the carotid sheath. IJV is exposed and preserved. The omohyoid muscle is skeletonised at the hyoid and used as the inferior boundary marker.
-
Specimen removed en bloc — Oriented and sent to histopathology. All levels should be separately marked.
-
Haemostasis + closure:
- Suction drains (Redivac/Blake) × 1–2 placed
- Platysma closed (2-0 Vicryl)
- Skin closed (3-0 Prolene or staples)
Postoperative Considerations
| Issue | Action |
|---|---|
| Shoulder dysfunction | Physiotherapy; due to SAN traction |
| Chylous fistula | Left-side dissection; milky discharge in drain; TPN/fat-free diet / surgical ligation |
| Haemorrhage | Drain output monitoring; carotid "blowout" is the most feared complication |
| Wound infection | Antibiotics; oral flora contamination risk |
| Facial/cerebral edema | Bilateral IJV ligation avoided — serial surgeries or staged |
| Pathological margin | Frozen section control intraoperative; if positive → re-excise |
Post-op Oncological Decision Points
- pN0 (no nodes) + clear margins → Surveillance
- pN+ single node, no ENE → consider post-op RT
- Multiple nodes or ENE → Post-op chemoradiation (platinum-based)
- Positive/close margins → Post-op RT ± chemotherapy
- DOI >4 mm in clinically N0 tongue → Elective neck dissection (levels I–IV) justified
Sources: K.J. Lee's Essential Otolaryngology; Cummings Otolaryngology Head & Neck Surgery (6e); Bailey & Love's Short Practice of Surgery (28e)
Good luck in the OT today. If the consultant pushes you on margins, the answer they want to hear is: "1 cm clinical margin, confirmed by intraoperative frozen section, with DOI driving the decision for elective neck dissection."
Incision for modifiedneck dissection
Finding Sources
Searching Images
neck dissection incision types apron MacFee utility
Reading File
Loading Image
Loading Image
Here are all the neck dissection incisions you need to know, with the clinical context for each.
Incisions for Modified Neck Dissection
The Guiding Principle
A good neck dissection incision must:
- Give adequate exposure of all levels being dissected
- Avoid trifurcate points (three-way junctions = poor blood supply = necrosis risk)
- Keep the carotid artery covered by a broad skin flap at all times
- Lie in a skin crease where possible (cosmesis)
- Avoid prior radiation ports when possible
1. MacFee Incision (Two Parallel Transverse Incisions) — MOST COMMONLY USED
Two horizontal parallel incisions:
- Upper limb: 2 fingerbreadths below mandible, from mastoid tip to midline/submental region
- Lower limb: Just above the clavicle (supraclavicular), extending laterally

Why it's preferred:
- Best blood supply to the intervening skin bridge — the central skin flap between the two incisions receives perforators from both sides
- Best choice in irradiated necks — lowest wound dehiscence rate (0% in one study vs. 11% for triradiate)
- Cosmetically excellent — lies in skin creases (Langer's lines)
- No trifurcate point
Limitation: Slightly less direct access to the submandibular triangle (Level I) compared to apron incision
2. Modified Apron (Schobinger) Incision — Most Common for Levels I–III
Single curvilinear incision, starting 2 cm below the mastoid tip, curving forward below the mandible toward the submental region, then back down to the clavicle along the anterior SCM border.
Variants:
- Can be extended into a lip-split for oral cavity access (pull-through technique)
- Bilateral apron: Extends across the midline to the other side — for bilateral SND
- Boomerang incision: For bilateral ND when lip-splitting is also required
Why it's used here (oral tongue + neck):
- Ideal for combined wide local excision + neck dissection — the upper limb can be extended to access the oral cavity via pull-through or lip split
- Excellent Level I and II exposure
- Single incision = simpler and cosmetically reasonable
3. Hockey Stick Incision
A low transverse incision (~1–2 cm above clavicle) that curves upward along the posterior border of SCM toward the mastoid tip — making an "L" shape.

Used for: Levels II–IV or IV–VI (thyroid cancer). Less commonly used for full MRND as upper Level I exposure is limited.
4. Triradiate (Y / T-shaped) Incision — Now Largely Abandoned
Three limbs meeting at a single point on the neck — this trifurcate junction is ischaemic and prone to breakdown, especially post-RT. Wound dehiscence rate 11% vs 0% for apron. Historically used for radical ND; rarely used now.
Summary Table
| Incision | Shape | Best For | Key Advantage | Avoid When |
|---|---|---|---|---|
| MacFee | Two parallel horizontals | MRND, post-RT neck | Best vascularity, lowest dehiscence | Need concurrent oral cavity access |
| Apron (Schobinger) | Single curvilinear | SND I–III + oral cavity combined | Level I exposure, extendable | Heavily irradiated neck |
| Hockey stick | L-shape | Levels II–IV, thyroid ND | Lower neck access | Need upper level I |
| Triradiate | Y/T | Historically radical ND | — | Irradiated neck, modern surgery |
For Today's Case (Tongue SCC + Right MRND)
The modified apron incision is most appropriate — it allows:
- Access to Levels I–V on the right
- Can be connected to the oral cavity via pull-through or lip-split for the tongue wide local excision
- The incision is placed in a skin crease, 2 cm below the mandible
If the neck has been previously irradiated (e.g., salvage case), switch to MacFee to reduce flap necrosis risk.
Source: Cummings Otolaryngology Head & Neck Surgery, 6e
This is a shared conversation. Sign in to Orris to start your own chat.