Clinical anatomy of the ear. Physiology and research methods of auditory and vestibular analyzers.
Reading File
Finding Sources
Finding Sources
Searching Images
anatomy of the ear cochlea vestibular system diagram
Finding Sources
Searching Images
middle ear ossicles tympanic membrane anatomy
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Searching Images
inner ear cochlea hair cells organ of Corti physiology transduction
Reading File
Searching Images
audiometry hearing test tuning fork Rinne Weber vestibular caloric testing
Reading File
I now have comprehensive information from Gray's Anatomy for Students and supplementary images. Let me compile the full answer.
Clinical Anatomy of the Ear — Physiology and Research Methods of the Auditory and Vestibular Analyzers
I. OVERVIEW
The ear is the paired organ of hearing and balance, housed within the temporal bone. It has three anatomical divisions: external ear, middle ear, and internal ear (labyrinth).
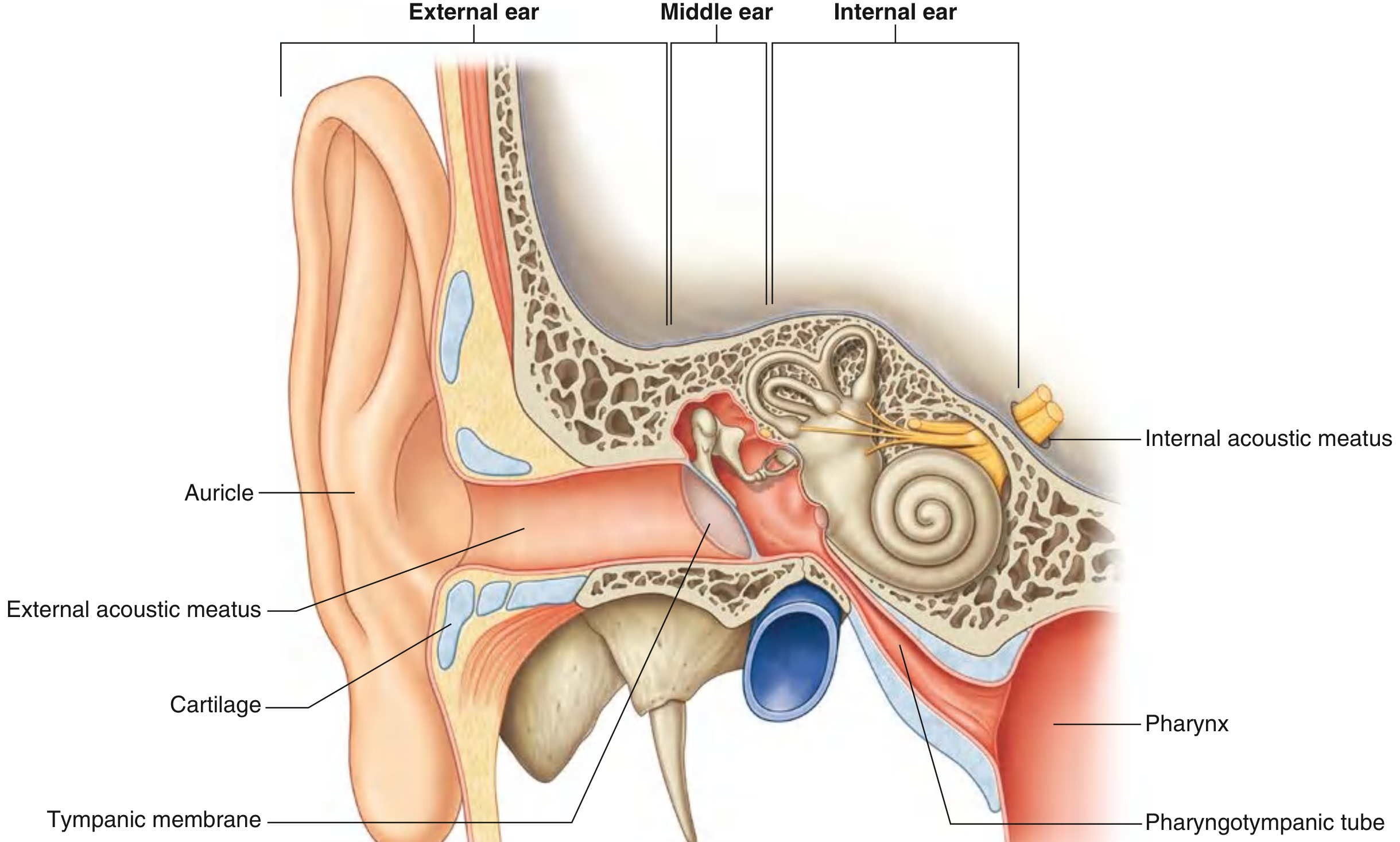
Fig. Right ear showing all three divisions — Gray's Anatomy for Students
II. EXTERNAL EAR
Auricle (Pinna)
The auricle is a cartilaginous framework covered with skin, designed to capture and funnel sound. Key surface landmarks:
- Helix — large outer rim, ending inferiorly at the fleshy lobule (only part without cartilage)
- Antihelix — curved ridge parallel and anterior to the helix
- Concha — deep hollow from which the external acoustic meatus opens
- Tragus — elevation anterior to the meatal opening
- Antitragus — elevation above the lobule, opposite the tragus
Muscles: Intrinsic muscles alter auricle shape; extrinsic muscles (anterior, superior, posterior auricular) reposition it. All are innervated by the facial nerve [VII].
Innervation of auricle:
- Great auricular nerve (C2–C3) — outer and posterior surfaces
- Auriculotemporal nerve (V3) — anterior and superior surfaces
- Lesser occipital nerve (C2) — superior part of the posterior surface
- Auricular branch of vagus [X] — small contribution
External Acoustic Meatus
A canal about 2.5 cm long, running from the concha to the tympanic membrane. The outer one-third is cartilaginous; the inner two-thirds are bony (temporal bone). The canal curves slightly (anterior and inferior), requiring the auricle to be pulled posterosuperiorly for otoscopic examination.
Innervation: Primarily by the auriculotemporal nerve [V3] (anterior/superior walls) and the auricular branch of the vagus [X] (posterior/inferior walls) — stimulation of the posterior wall can elicit the Arnold reflex (coughing).
III. TYMPANIC MEMBRANE
The tympanic membrane (eardrum) separates the external meatus from the middle ear. It is positioned obliquely — sloping medially from superior to inferior and posteriorly to anteriorly. It consists of a connective tissue core lined with skin externally and mucous membrane internally.
- Umbo — the central concavity produced by attachment of the handle (manubrium) of the malleus
- Cone of light — anteroinferior bright light reflex visible on otoscopy
- Pars flaccida (Shrapnell's membrane) — thin, superior part above the malleolar folds, clinically significant in cholesteatoma
- Pars tensa — thick, taut remainder of the membrane
- Fibrocartilaginous ring — attaches the membrane peripherally to the tympanic sulcus
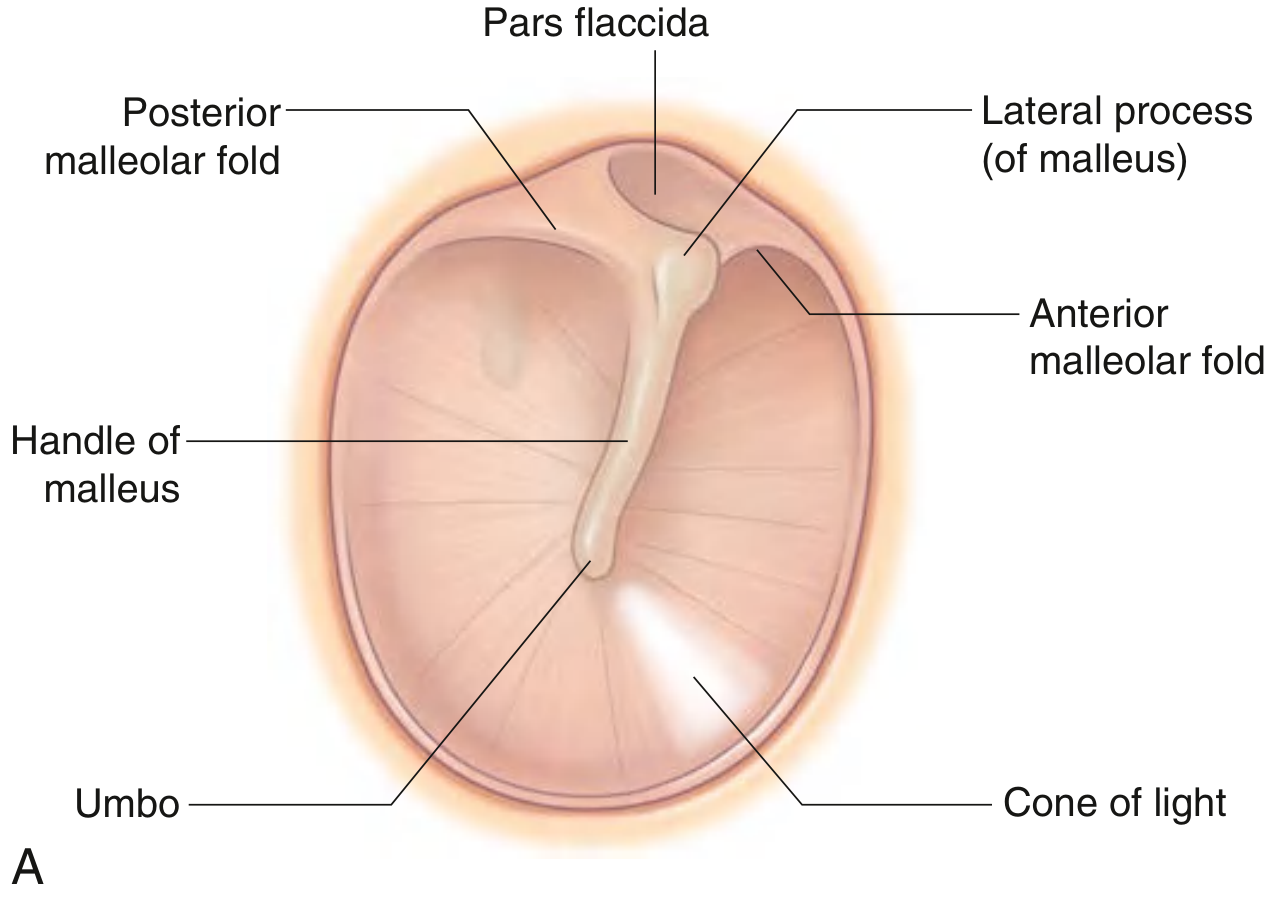
Fig. Tympanic Membrane (Right Ear) — Gray's Anatomy for Students
Innervation: Outer surface: auriculotemporal nerve [V3] + auricular branch of vagus [X]; inner surface: tympanic branch of glossopharyngeal [IX].
IV. MIDDLE EAR (TYMPANIC CAVITY)
A mucosa-lined cavity in the petrous part of the temporal bone, containing the ossicular chain and two small muscles.
Walls
| Wall | Feature |
|---|---|
| Lateral | Tympanic membrane |
| Medial | Promontory (basal turn of cochlea), oval window (fenestra vestibuli), round window (fenestra cochleae), prominence of facial canal |
| Roof | Tegmen tympani — thin bone separating from middle cranial fossa |
| Floor | Thin bone overlying the jugular fossa |
| Anterior | Opening of pharyngotympanic tube; canal for tensor tympani |
| Posterior | Aditus to mastoid antrum; pyramidal eminence (for stapedius) |
Ossicular Chain
Three bones transmit vibrations from the tympanic membrane to the oval window:
- Malleus (hammer) — handle (manubrium) attached to tympanic membrane; head in the epitympanic recess
- Incus (anvil) — articulates with malleus (incudomalleolar joint) and stapes (incudostapedial joint)
- Stapes (stirrup) — footplate seals the oval window via the annular ligament

Fig. Middle ear ossicular chain — CT and finite element model
Middle Ear Muscles
- Tensor tympani — arises from cartilaginous part of pharyngotympanic tube; inserts on handle of malleus; pulls malleus medially, tensing the tympanic membrane; innervated by medial pterygoid nerve (V3)
- Stapedius — smallest skeletal muscle in the body; arises from pyramidal eminence; inserts on neck of stapes; pulls stapes posteriorly, dampening oscillations; innervated by facial nerve [VII]. The acoustic reflex (contraction of stapedius to loud sounds) protects the cochlea.
Pharyngotympanic (Eustachian/Auditory) Tube
- Connects the middle ear to the nasopharynx, equalizing air pressure on both sides of the tympanic membrane
- Bony part (1/3): near the middle ear
- Cartilaginous part (2/3): toward the nasopharynx
- Opens during swallowing and yawning; dysfunctional in otitis media with effusion ("glue ear")
V. INTERNAL EAR (LABYRINTH)
The internal ear is embedded in the petrous part of the temporal bone and consists of a bony labyrinth enclosing a membranous labyrinth.

Fig. Normal human inner ear — anatomical diagram and 3D FIESTA MRI
Bony Labyrinth
Contains perilymph (similar to ECF: high Na⁺, low K⁺). Consists of:
- Vestibule — central chamber; contains the oval window in its lateral wall; communicates anteriorly with the cochlea and posterosuperiorly with the semicircular canals
- Three semicircular canals — anterior (superior), posterior, and lateral (horizontal); each oriented at right angles to the others; each has one dilated ampulla; detect rotational (angular) acceleration
- Cochlea — anterior spiral structure, 2½–2¾ turns around a central bony column (the modiolus); the spiral lamina extends from the modiolus and partially divides the cochlear canal
Membranous Labyrinth
Contains endolymph (similar to ICF: high K⁺, low Na⁺, maintained by the stria vascularis). Consists of:
- Utricle and saccule (otolithic organs) — in the vestibule; contain the macula
- Utricle: detects linear acceleration in the horizontal plane and sideways head tilts
- Saccule: detects linear acceleration in the vertical plane (up-down, forward-back)
- Three semicircular ducts — within the bony canals; each ampulla contains a crista ampullaris (responds to angular/rotational acceleration)
- Cochlear duct (scala media) — contains the spiral organ of Corti (organ of hearing); bounded by Reissner's membrane (above), basilar membrane (below), and spiral ligament (laterally)

Fig. 3D statistical shape model of the bony labyrinth
Blood Supply to the Internal Ear
- Membranous labyrinth: supplied by the labyrinthine artery (usually a branch of the AICA or basilar artery), dividing into the common cochlear artery and anterior vestibular artery
- The blood–labyrinth barrier (analogous to BBB) maintains the unique ionic composition of endolymph
VI. VESTIBULOCOCHLEAR NERVE [VIII]
- Enters the internal acoustic meatus (IAC), accompanied by the facial nerve [VII]
- Divides into:
- Cochlear nerve — cell bodies in the spiral ganglion within the modiolus
- Vestibular nerve — cell bodies in the vestibular (Scarpa's) ganglion in the IAC; upper and lower divisions innervate the cristae and maculae
VII. PHYSIOLOGY OF THE AUDITORY ANALYZER
Sound Transmission (Conduction)
- Sound waves are collected by the auricle and travel through the external meatus to vibrate the tympanic membrane
- Vibrations are amplified and transmitted via the ossicular chain (malleus → incus → stapes) to the oval window
- The middle ear achieves a ~25 dB pressure gain via two mechanisms:
- Area ratio — tympanic membrane (~55 mm²) is ~17× larger than the oval window (~3.2 mm²)
- Lever action of the ossicular chain (~1.3:1)
- Stapes footplate vibration creates pressure waves in the perilymph of the scala vestibuli
- Waves travel up the scala vestibuli, around the helicotrema (apex), and down the scala tympani to the round window (which bulges to accommodate fluid displacement)
Cochlear Transduction (Sensory)
- Pressure differences across the basilar membrane cause it to deflect; the basilar membrane is tonotopically organized — high-frequency sounds (20 kHz) maximally stimulate the base, low-frequency sounds (20 Hz) the apex
- The spiral organ of Corti on the basilar membrane contains:
- Inner hair cells (IHCs) — single row; primary afferent sensory cells (~3,500); 95% of cochlear nerve fibers synapse here
- Outer hair cells (OHCs) — three rows (~12,000); electromotile amplifiers that sharpen frequency tuning via prestin-driven somatic motility
- Hair cell stereocilia are embedded in (OHC) or contact (IHC) the tectorial membrane; basilar membrane deflection shears the stereocilia
- Tip links between stereocilia open mechanically-gated MET channels, allowing K⁺ and Ca²⁺ influx from endolymph → depolarization → neurotransmitter (glutamate) release at the IHC base → activation of cochlear nerve fibers
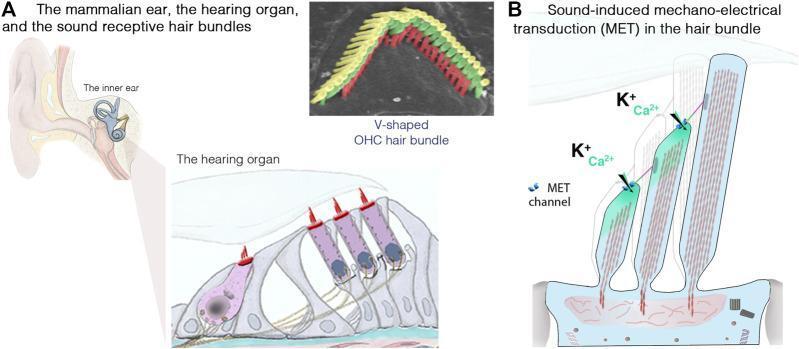
Fig. IHC/OHC anatomy and MET channel mechanism (stereocilia tip links, K⁺/Ca²⁺ influx)
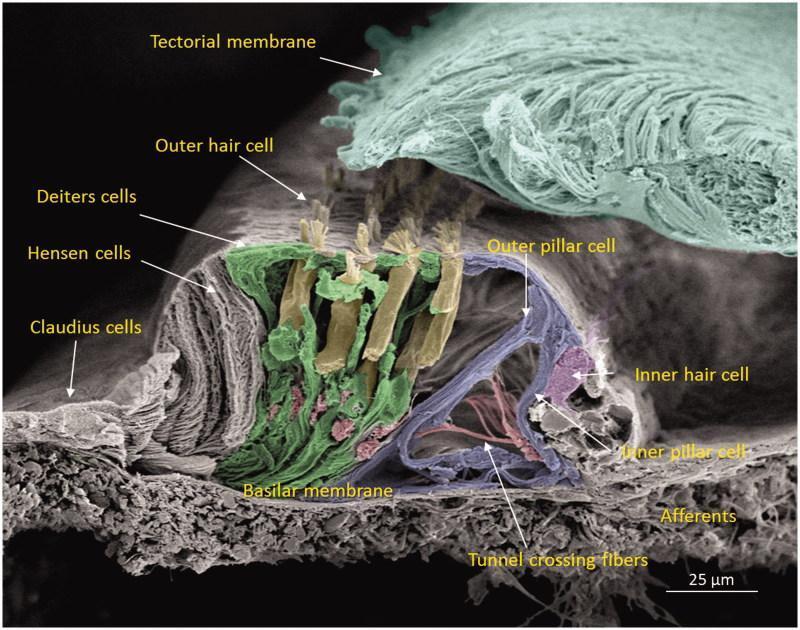
Fig. Colorized SEM: IHC, OHC rows, pillar cells (tunnel of Corti), Deiters cells, basilar membrane
Central Auditory Pathway
Cochlear nerve → cochlear nuclei (medulla) → superior olivary complex (bilateral, mediates sound localization) → lateral lemniscus → inferior colliculus (midbrain) → medial geniculate nucleus (thalamus) → primary auditory cortex (Heschl's gyri, superior temporal plane, areas 41 & 42)
VIII. PHYSIOLOGY OF THE VESTIBULAR ANALYZER
Otolithic Organs (Utricle & Saccule — Linear Acceleration)
- The macula contains hair cells embedded in a gelatinous membrane topped by otoconia (calcium carbonate crystals)
- When the head tilts or accelerates linearly, otoconia shift due to gravity/inertia → shear force on stereocilia → hair cell depolarization or hyperpolarization (depending on direction of deflection relative to the kinocilium)
Semicircular Canals (Angular Acceleration)
- The crista ampullaris in each ampulla bears hair cells embedded in the gelatinous cupula (which spans the full width of the ampullary lumen)
- Angular head rotation causes inertia-based endolymph lag → cupula deflection → hair cell transduction
- The three canals are orthogonally arranged; each canal works in a push-pull pair with its contralateral counterpart (lateral–lateral; anterior–contralateral posterior)
Vestibulo-Ocular Reflex (VOR)
Vestibular input → vestibular nuclei (brainstem) → motor neurons of extraocular muscles → compensatory eye movement opposite to head rotation; stabilizes the visual image on the retina. Gain ≈ 1 (equal and opposite).
Central Vestibular Pathway
Vestibular nerve → vestibular nuclei (pontomedullary junction: superior/inferior/medial/lateral [Deiters']) → cerebellum (flocculus, nodulus), spinal cord (vestibulospinal tracts for postural control), thalamus, parieto-insular vestibular cortex
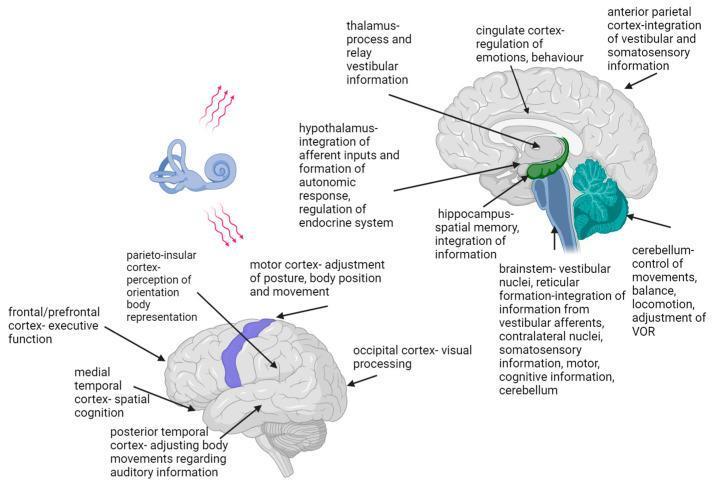
Fig. Vestibular network: brainstem, cerebellum, thalamus, cortical projections
IX. RESEARCH AND CLINICAL METHODS
Auditory Assessment
| Method | Principle | Clinical Use |
|---|---|---|
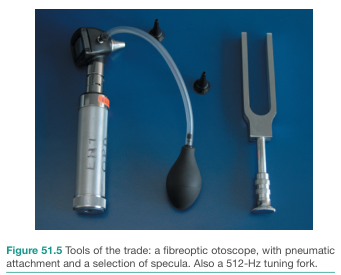
| Tuning fork tests (Rinne, Weber) | Compares air vs. bone conduction (Rinne); lateralization (Weber) | Distinguish conductive vs. sensorineural hearing loss (SNHL) |
| Pure tone audiometry (PTA) | Thresholds at 250–8,000 Hz via air and bone conduction headphones | Gold standard; defines type and degree of hearing loss |
| Speech audiometry | Speech reception threshold (SRT), word recognition score | Functional hearing assessment |
| Tympanometry | Air-pressure changes in sealed canal; measures TM and middle ear compliance | Detects effusion (flat type B), eardrum perforation, ossicular fixation |
| Acoustic reflex testing | Stapedius contraction to loud tones (70–85 dB above threshold) | Assesses CN VII, CN VIII, brainstem integrity; absent in facial palsy |
| Otoacoustic emissions (OAEs) | Sounds generated by OHC electromotility, detected by microphone in canal | Newborn hearing screening; differentiates OHC loss (absent OAE) from neural pathology |
| Auditory brainstem response (ABR/BERA) | Click-evoked brainstem potentials (waves I–V) | Threshold estimation in infants; detects retrocochlear lesions; intraoperative monitoring |
| Electrocochleography (ECoG) | Summating potential (SP) and action potential (AP) ratio | Menière's disease diagnosis (elevated SP/AP ratio >0.4) |
Vestibular Assessment
| Method | Principle | Clinical Use |
|---|---|---|
| Caloric testing | Irrigation of EAC with warm (44°C) or cool (30°C) water creates endolymph convection in the lateral SCC, producing nystagmus | Assesses each labyrinth independently; canal paresis in unilateral loss |
| Video Head Impulse Test (vHIT) | High-velocity, small-amplitude head rotations recorded by high-speed camera; corrective saccades indicate VOR deficit | Tests all six semicircular canals; sensitive for acute vestibular neuritis |
| Videonystagmography (VNG) | Records eye movements during caloric, gaze, and positional testing | Comprehensive peripheral/central vestibular evaluation |
| Dix-Hallpike maneuver | Provokes geotropic/apogeotropic nystagmus with rapid positioning | Diagnoses BPPV (posterior canal most common) |
| Vestibular Evoked Myogenic Potentials (VEMPs) | Loud clicks/tones evoke sacculocollic (cVEMP, via SCM) or utriculoocular (oVEMP, via inferior oblique) responses | Assesses saccule and utricle function; detects dehiscence, hydrops |
| Posturography (SOT) | Platform tests proprioceptive, visual, and vestibular contributions to balance | Quantifies functional balance impairment |
| Rotary chair testing | Sinusoidal/trapezoidal rotation in darkness at low frequencies | Tests bilateral vestibular loss; VOR gain, phase, and symmetry |
| MRI temporal bone | 3D FIESTA/CISS sequences | Detects endolymphatic hydrops (Menière's), acoustic neuroma, labyrinthine aplasia |
| CT temporal bone (HRCT) | High-resolution bone algorithm | Otosclerosis, semicircular canal dehiscence, ossicular chain lesions |
X. KEY CLINICAL CORRELATIONS
| Condition | Anatomical/Physiological Basis |
|---|---|
| Otitis media | Pharyngotympanic tube dysfunction → middle ear effusion → conductive hearing loss |
| Otosclerosis | Abnormal bone remodeling at oval window → stapes fixation → conductive loss |
| Cholesteatoma | Pars flaccida retraction pocket → keratin debris accumulation → erosion of ossicles, labyrinth |
| Presbycusis | Progressive OHC loss at the basal cochlea → high-frequency SNHL |
| Menière's disease | Endolymphatic hydrops (excess endolymph) → episodic vertigo, fluctuating SNHL, tinnitus, aural fullness |
| BPPV | Displaced otoconia (from utricle) into posterior SCC → abnormal cupulolithiasis/canalolithiasis |
| Vestibular neuritis | Viral inflammation of superior vestibular nerve → acute unilateral VOR failure, spontaneous nystagmus |
| Acoustic neuroma (vestibular schwannoma) | Schwann cell tumor of CN VIII at IAC/CPA → unilateral SNHL, tinnitus, unsteadiness |
| Mastoiditis | Infection spreads from middle ear → mastoid air cells (same mucosal lining) → risk of intracranial spread |
Sources: Gray's Anatomy for Students — Chapter 8 (Head and Neck), pp. 1093–1111; K.J. Lee's Essential Otolaryngology; Bailey and Love's Short Practice of Surgery, 28th ed.
This is a shared conversation. Sign in to Orris to start your own chat.