Hydrocephalus treatment
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Here is a comprehensive overview of hydrocephalus treatment based on authoritative neurology textbooks.
Hydrocephalus Treatment
Core Principle
The definitive treatment for hydrocephalus is surgical diversion (shunting) of CSF. Medical management has very limited efficacy in most forms.
1. Surgical Treatment
Ventriculoperitoneal (VP) Shunt — Primary Approach
- A catheter is inserted into the lateral ventricle (preferably the anterior horn of the right ventricle, where there is no choroid plexus) to reduce catheter blockage.
- CSF is diverted to the peritoneal cavity via a tube with a one-way pressure-sensitive valve.
- This is the most common shunt type in both adults and children.
Key technical points:
- Meticulous aseptic technique + peri/postoperative antibiotics reduce infection risk.
- Adjustable valves allow the opening pressure to be modified non-invasively after placement.
- Anti-siphon devices prevent excessive CSF drainage when the patient is upright (important in the "slit ventricle" syndrome in children).
Ventriculoatrial (VA) Shunt
- CSF diverted to the right atrium — less common.
- Rare complications include pulmonary hypertension, pulmonary embolism, and nephritis (due to low-grade Staphylococcal infection of the shunt).
Endoscopic Third Ventriculostomy (ETV)
- The floor of the third ventricle is perforated endoscopically, creating an alternative CSF drainage pathway.
- Best suited for obstructive (non-communicating) hydrocephalus.
- Can be effective for shunt failure, though long-term results when used as a primary approach have been mixed.
- "Puncture of the floor of the third ventricle by endoscopic techniques ('third ventriculostomy') has been explored as an alternative to shunting... sometimes an effective treatment of shunt failure" — Adams and Victor's Principles of Neurology
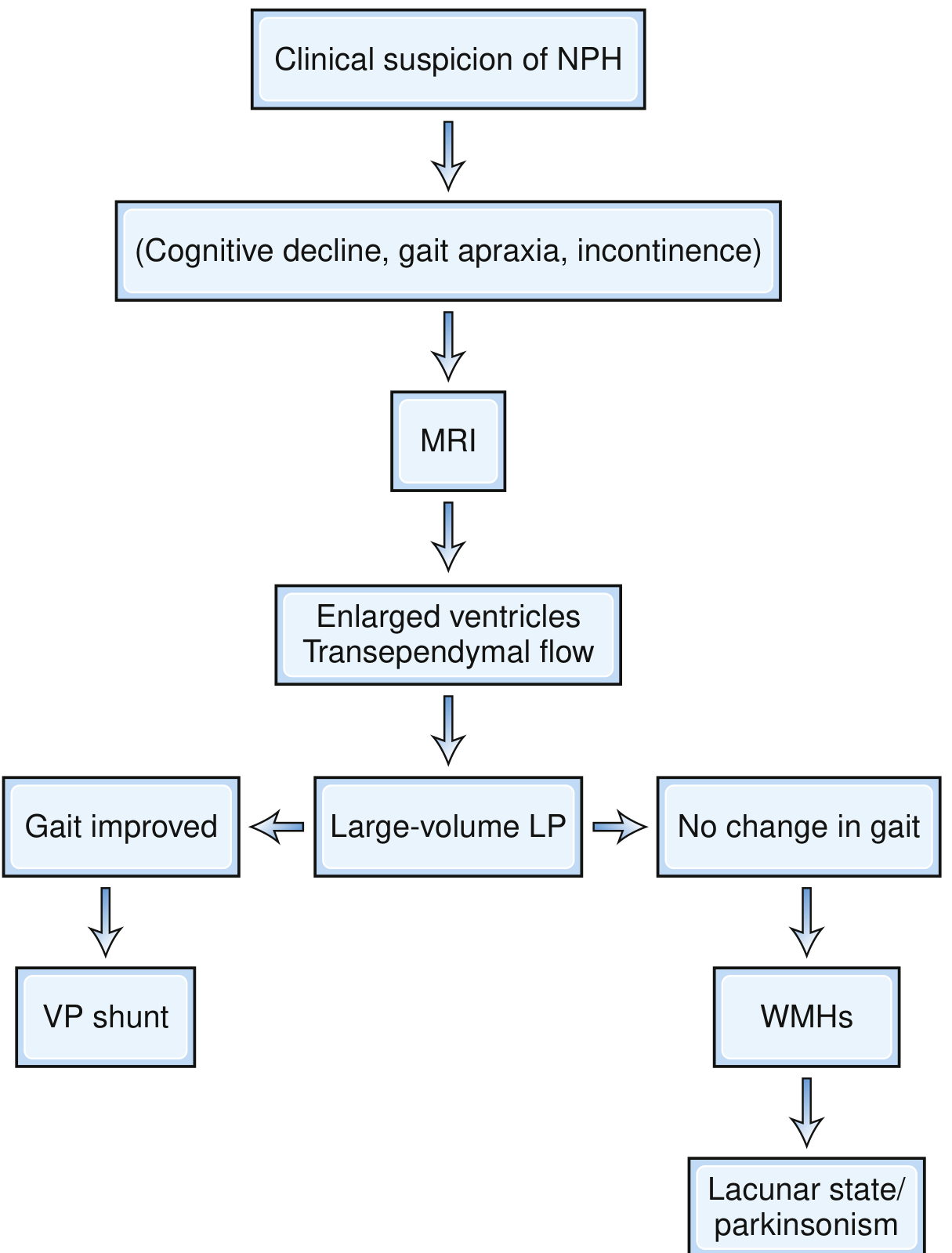
2. Normal-Pressure Hydrocephalus (NPH)
NPH presents with the classic triad: gait disturbance (apraxic, "magnetic" gait), cognitive impairment (subcortical dementia), and urinary incontinence.
Patient Selection for VP Shunt (Algorithm)
- FLAIR MRI — look for: enlarged ventricles (especially temporal horns), transependymal CSF absorption, and disproportionate cortical atrophy relative to age.
- Large-volume LP (tap test) — remove 30–50 mL CSF and observe gait over several days.
- Gait improvement → proceed to VP shunt (good predictor of response).
- Patients with extensive white-matter changes likely have lacunar state or vascular parkinsonism and may not benefit from shunting.
- Other methods: ICP monitoring, CSF infusion tests, cisternography, regional cerebral blood flow (increased CBF after CSF removal predicts shunt response).
Outcomes
- Approximately 80% improvement in carefully selected patients (some series).
- Gait disturbance responds better and faster than cognitive impairment.
- Clinical improvement may occur within weeks; ventricular shrinkage usually follows within 1–2 weeks of shunting.
3. Infantile and Childhood Hydrocephalus
Management is more complex, with additional challenges:
| Complication | Management |
|---|---|
| Catheter obstruction / migration | Shunt revision |
| Peritoneal pseudocysts | Shunt revision / repositioning |
| Slit ventricle syndrome (over-drainage, low-pressure headaches in upright position) | Replace valve with higher-pressure valve; add anti-siphon device |
| Cranial growth failure | Early intervention to normalize ICP |
- ~72% of shunted hydrocephalic children achieve IQ 70–100; a minority achieve normal intellect.
- Whether to shunt all hydrocephalic infants soon after birth remains controversial, as outcomes vary.
4. Acute / Emergency Hydrocephalus
- Caused by obstructive masses (colloid cyst of the third ventricle, ependymoma, cerebellar hemorrhage/infarction, intraventricular cysticercosis).
- Emergency external ventricular drain (EVD) or urgent VP shunt placement to decompress.
- Cerebellar hemorrhage compressing the brainstem: ventricular catheter for decompression → posterior fossa craniectomy to remove the mass.
5. Medical Management
- Acetazolamide (carbonic anhydrase inhibitor) — reduces CSF production; used in NPH and posthemorrhagic hydrocephalus of prematurity but clinical effects have been minimal in controlled trials.
- Steroids — useful when hydrocephalus is caused by inflammation (e.g., neurosarcoidosis, neurocysticercosis).
- Medical treatment is not definitive; most cases ultimately require surgical intervention.
6. Shunt Complications
| Complication | Notes |
|---|---|
| Shunt infection | Most commonly Staphylococcus epidermidis; occurs mostly soon after placement |
| Shunt obstruction | Most common cause of shunt failure; presents with recurrence of ICP symptoms |
| Subdural hematoma | From over-drainage |
| Slit ventricle syndrome | Over-drainage in children |
| Bowel/stomach perforation | Rare VP shunt complication |
| Pulmonary complications | Pleural effusion (VP shunt tip migration), pulmonary hypertension (VA shunt) |
Sources: Adams and Victor's Principles of Neurology, 12th Ed. | Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.