Principles and management of blunt injury abdomen with flow chats and images in detail for 10 marks long question of pg
Reading File
Finding Sources
Finding Sources
Searching Images
blunt abdominal trauma management flowchart FAST scan
Reading File
Reading File
Reading File
Searching Images
FAST examination zones abdominal trauma diagnostic algorithm
Reading File
Finding Sources
Searching Images
splenic laceration liver laceration CT grading abdominal trauma organ injury scale
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent! I now have all the key content and images needed. Let me compile a comprehensive, detailed PG-level 10-marks answer.
Blunt Injury Abdomen: Principles and Management
1. INTRODUCTION & EPIDEMIOLOGY
Blunt abdominal trauma (BAT) accounts for ~75% of all abdominal injuries in major trauma registries. Motor vehicle collisions (MVCs) are responsible for the majority of cases; falls, direct blows, and sports-related compression constitute the remainder. Despite advances in imaging, blunt injuries can be occult and deceptively benign initially, making systematic evaluation mandatory. The spleen is the most commonly injured solid organ (in ~2/3 of cases, as an isolated injury), followed by the liver; hollow viscus injury occurs in only 1–5% but is associated with high morbidity if missed.
— Rosen's Emergency Medicine, pp. 488–490; Mulholland & Greenfield's Surgery 7e, p. 1258
2. MECHANISMS OF INJURY
Three fundamental force patterns operate in blunt abdominal trauma:
| Mechanism | Effect |
|---|---|
| Compressive (crush) | Solid organ rupture (spleen, liver, kidney); bowel rupture from sudden rise in intraluminal pressure |
| Deceleration (shear) | Tearing at fixed points — hepatic veins, mesentery, renal pedicle |
| Direct blow | Contusion, subcapsular haematoma, parenchymal laceration |
The solid organs (spleen, liver, kidney) are vulnerable to compression and deceleration. The retroperitoneal duodenum and pancreas are protected by the spine and become injured when crushed against it. The hollow viscera may rupture from sudden rise in intraluminal pressure or devascularisation at mesenteric attachment points.
3. PATHOPHYSIOLOGY OF INJURY
Solid organ injury → parenchymal laceration → intraperitoneal haemorrhage (hemoperitoneum) → haemorrhagic shock.
Hollow viscus injury → perforation → faecal/biliary peritonitis → sepsis/SIRS → multi-organ dysfunction.
Retroperitoneal injury (duodenum, pancreas, major vessels, kidneys) → may be occult; no free peritoneal spillage; delayed presentation.
Diaphragmatic rupture → most commonly left-sided (buttressed on right by liver); may present acutely or be missed and present years later with visceral herniation/strangulation.
4. CLINICAL ASSESSMENT
4a. History
- Mechanism: speed of impact, seat-belt use, steering wheel deformation, airbag deployment
- Time of injury, pre-hospital vital signs, amount of fluid administered en route
- Comorbidities, anticoagulants, prior abdominal surgery
4b. Physical Examination
Clinical accuracy in BAT is only 55–65% — the initial presentation may be deceptively benign, especially with altered sensorium (intoxicants, head injury, distracting injuries).
Key findings on examination:
| Sign | Significance |
|---|---|
| Guarding, rigidity, rebound tenderness | Peritoneal irritation — blood or enteric spillage |
| Grey Turner's sign (flank bruising) | Retroperitoneal haematoma (delayed, 24–48 h) |
| Cullen's sign (periumbilical bruising) | Retroperitoneal blood tracking anteriorly |
| Kehr's sign (left shoulder pain) | Diaphragmatic irritation — splenic injury |
| Seat-belt sign (abdominal wall bruising) | ↑ risk of hollow viscus and mesenteric injury |
| Tenderness over lower ribs (left) | Splenic injury |
| Distended abdomen | Massive haemoperitoneum |
| Haematuria | Renal or bladder trauma |
| Blood at urethral meatus | Urethral injury — do NOT catheterise |
— Rosen's Emergency Medicine, pp. 491–492
5. INVESTIGATIONS
5a. Laboratory
- FBC (serial haematocrit trending), coagulation profile
- Arterial blood gas (base deficit and lactate as markers of shock severity)
- Serum amylase/lipase (pancreatic injury — not sensitive in isolation)
- LFTs, urinalysis
- Group & crossmatch, massive transfusion protocol activation if needed
5b. FAST Examination (Focused Assessment with Sonography for Trauma)
The first-line bedside investigation performed simultaneously with resuscitation.
Four standard FAST windows:
- Pericardial (subxiphoid)
- Right upper quadrant — Morison's pouch (hepatorenal space)
- Left upper quadrant — splenorenal recess
- Pelvis — pouch of Douglas / rectovesical pouch
Extended FAST (eFAST) adds bilateral thoracic views for pneumo/haemothorax.
Positive FAST = anechoic free fluid in dependent peritoneal spaces = hemoperitoneum

FAST pitfalls: Suboptimal for retroperitoneal injury and hollow viscus injury. Negative FAST does not exclude significant injury — sensitivity is ~85% for hemoperitoneum of >500 mL.
5c. CT Abdomen & Pelvis (with IV Contrast)
Gold standard for evaluating BAT in the haemodynamically stable patient. Sensitivity ~95% for solid organ injuries; sensitivity for hollow viscus injury ~80% (imperfect — free fluid without solid organ injury on CT mandates high suspicion for hollow viscus perforation).
CT findings suggesting injury:
- Free fluid (hyperdense in acute haemorrhage) — most common finding
- Parenchymal laceration (hypodense), subcapsular haematoma
- Active contrast extravasation ("blush") — indicates ongoing arterial bleeding
- Free air — hollow viscus perforation
- Bowel wall thickening, mesenteric stranding/haematoma — hollow viscus/mesenteric injury
- Pancreatic oedema, disruption of pancreatic duct


5d. Diagnostic Peritoneal Lavage (DPL)
Now largely replaced by FAST and CT but retains value where these are unavailable.
Positive DPL criteria:
- Gross blood on aspiration (≥10 mL)
- RBC >100,000/mm³
- WBC >500/mm³ (after 3 hours)
- Bile, bacteria, food fibres
Highly sensitive (>98%) but non-specific; does not identify retroperitoneal injuries; contraindicated with prior abdominal surgery.
5e. Plain X-rays (Erect CXR & AXR)
- Free gas under the diaphragm — hollow viscus perforation
- Rib fractures (lower left → spleen risk; lower right → liver risk)
- Pelvic fractures
- Lost psoas shadow → retroperitoneal haematoma
- Elevated hemidiaphragm → diaphragmatic rupture or subphrenic pathology
6. ORGAN INJURY GRADING (AAST-OIS Scale)
The American Association for the Surgery of Trauma Organ Injury Scale (AAST-OIS) guides management decisions.
Liver Injury Scale
| Grade | Description |
|---|---|
| I | Subcapsular haematoma <10% surface area; capsular laceration <1 cm deep |
| II | Subcapsular haematoma 10–50%; laceration 1–3 cm deep, <10 cm long |
| III | Subcapsular haematoma >50% / expanding / ruptured; laceration >3 cm deep |
| IV | Parenchymal disruption 25–75% of hepatic lobe |
| V | Parenchymal disruption >75% of lobe; retrohepatic vena cava / hepatic vein injury |
| VI | Hepatic avulsion (lethal) |
Splenic Injury Scale
| Grade | Description |
|---|---|
| I | Subcapsular haematoma <10%; capsular laceration <1 cm deep |
| II | Subcapsular haematoma 10–50%; laceration 1–3 cm deep not involving trabecular vessels |
| III | Subcapsular haematoma >50% / expanding; laceration >3 cm deep or involving trabecular vessels |
| IV | Laceration involving segmental or hilar vessels → >25% devascularisation |
| V | Shattered spleen or hilar vascular injury → total devascularisation |
— Mulholland & Greenfield's Surgery 7e, pp. 1279–1293
7. MANAGEMENT — OVERVIEW
The cornerstone of management rests on the haemodynamic status of the patient. Two pathways diverge:
FLOWCHART 1 — Blunt Abdominal Trauma (BAT) Algorithm
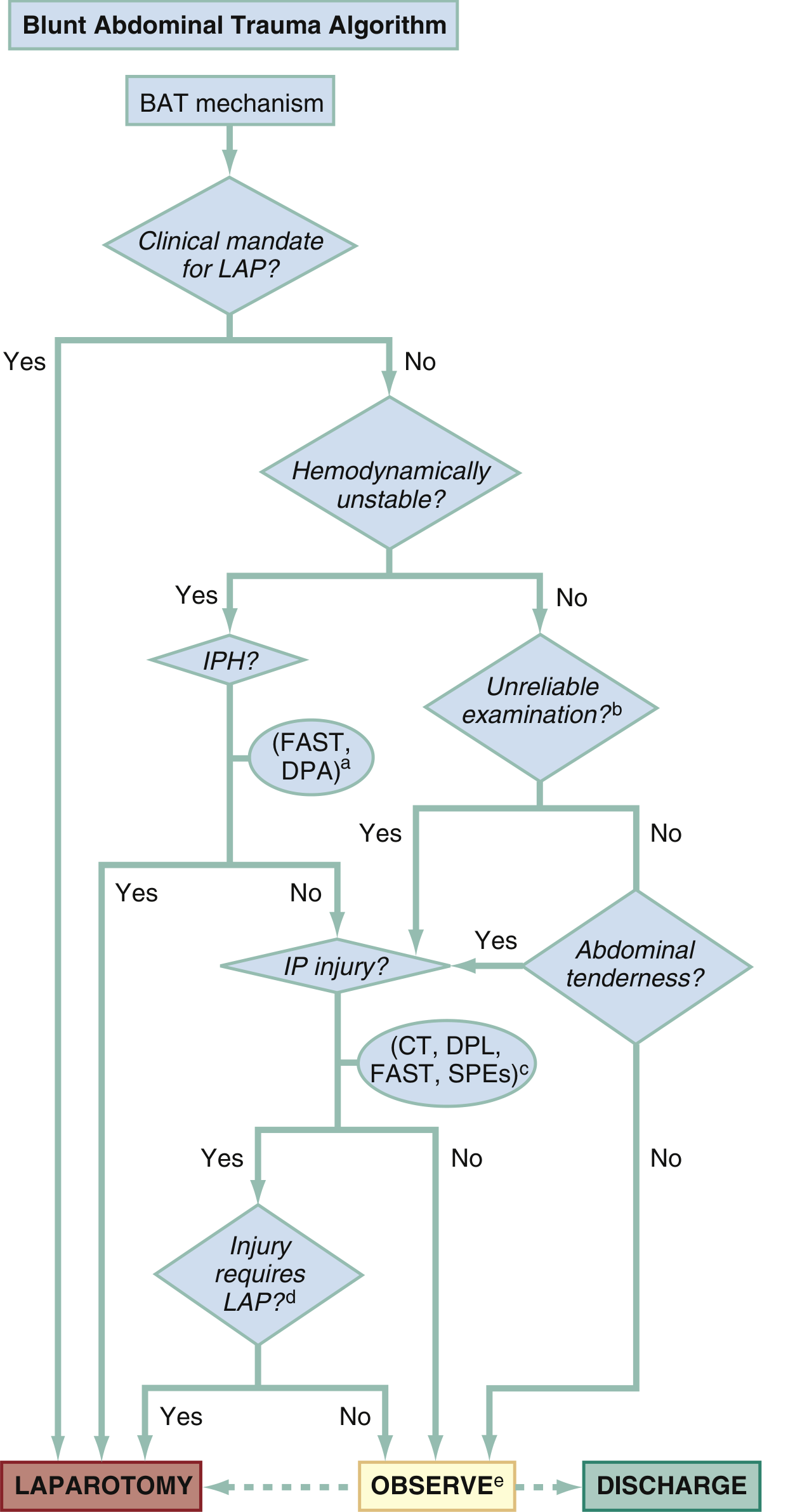
BAT Algorithm: Management of blunt abdominal trauma based on clinical mandate for laparotomy, haemodynamic stability, FAST/DPA findings, CT, and reliability of examination. Outcomes: Laparotomy / Observe / Discharge. (From Rosen's Emergency Medicine)
FLOWCHART 2 — Haemodynamically Stable Patient Decision Flow
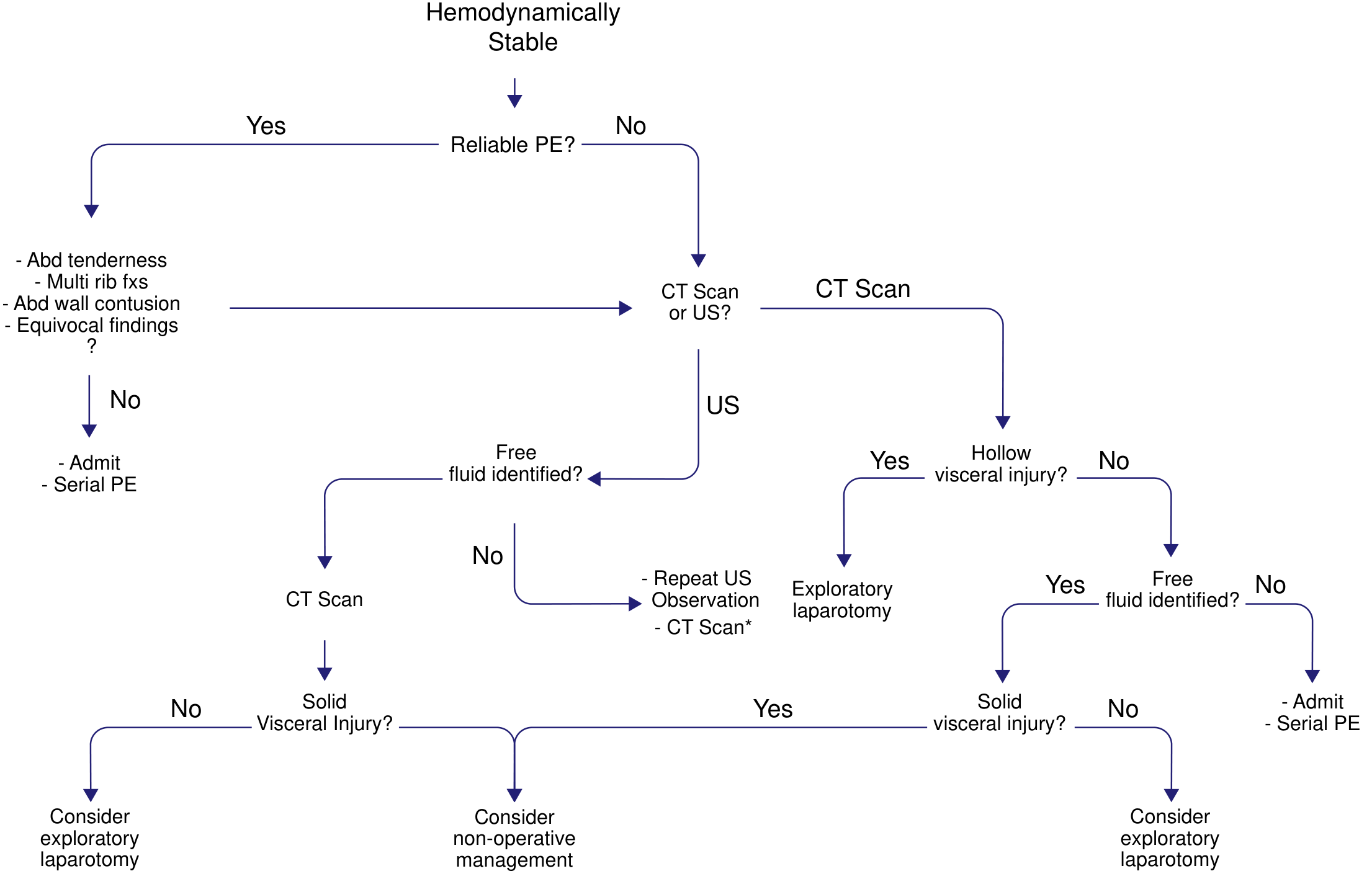
Management algorithm for hemodynamically stable blunt abdominal trauma: reliable physical exam guides CT vs ultrasound; findings dictate non-operative management, exploratory laparotomy, or observation with serial exams.
8. INITIAL RESUSCITATION (ATLS PRINCIPLES)
A — Airway with C-spine control (jaw thrust, intubation if GCS ≤8)
B — Breathing: tension pneumothorax, haemothorax excluded/treated
C — Circulation: two large-bore IVs; blood products — 1:1:1 ratio (PRBCs:FFP:platelets) = Damage Control Resuscitation
Key principle: permissive hypotension (SBP 80–90 mmHg) may be tolerated briefly before definitive haemorrhage control to avoid dilutional coagulopathy — though evidence mandating this practice is still evolving.
- Nasogastric tube decompression (orogastric if midface fracture suspected)
- Urinary catheterisation for hourly urine output monitoring (do not catheterise if blood at meatus)
- Massive Transfusion Protocol (MTP) activated if ≥10 units PRBCs anticipated in 24 h
9. OPERATIVE MANAGEMENT
Indications for Emergency Laparotomy in BAT
| Clinical Finding | Notes |
|---|---|
| Haemodynamic instability + positive FAST | Source is intraperitoneal haemorrhage |
| Peritonitis (rigid abdomen, diffuse rebound) | Hollow viscus injury |
| Pneumoperitoneum on X-ray/CT | Hollow viscus perforation |
| Evisceration | |
| Diaphragmatic rupture | Prevent herniation/strangulation |
| FAST + uncontrolled chest haemorrhage requiring OR | Combined injuries |
| DPL gross blood or >100,000 RBC/mm³ | Where FAST/CT unavailable |
— Rosen's Emergency Medicine, p. 495; Mulholland & Greenfield's Surgery 7e, p. 1261
Operative Approach
Positioning: Supine, arms abducted 90°; torso, neck, upper thighs prepped.
Incision: Full midline laparotomy (xiphoid to pubis); allows access to all quadrants, extension into thorax, groin or retroperitoneum as needed.
Damage Control Laparotomy (DCL)
Indicated when the patient is physiologically depleted — the "lethal triad" of:
- Hypothermia (<35°C)
- Acidosis (pH <7.2, base deficit >–6)
- Coagulopathy (INR >1.5)
Three phases of Damage Control Surgery:
- Phase I — abbreviated laparotomy: Pack bleeding quadrants, control haemorrhage with clamps/sutures (not formal repair), control contamination (staple off perforations), temporary abdominal closure (TAC)
- Phase II — ICU resuscitation: Correct coagulopathy, hypothermia, acidosis; ventilation, vasopressors, warming
- Phase III — definitive repair: Return to OR in 24–48 hours for formal bowel anastomosis, vascular repair, abdominal closure
Angioembolisation is a critical adjunct — particularly for ongoing hepatic, splenic, or pelvic arterial bleeding in damage-control patients.
Abdominal Compartment Syndrome (ACS)
Intra-abdominal pressure >20 mmHg + new organ dysfunction = ACS. Prevent by monitoring bladder pressures post-laparotomy; treat with decompressive laparotomy.
10. NON-OPERATIVE MANAGEMENT (NOM)
Prerequisites for NOM:
- Haemodynamic stability (SBP >90 mmHg, HR <100)
- Reliable clinical examination (alert, cooperative patient)
- No peritonitis
- No hollow viscus injury on CT
- Institution capable of close monitoring (trauma surgeon, blood bank, OR on standby)
NOM success rates:
- Blunt spleen injuries: ~80% in adults, 90–95% in children
- Blunt liver injuries: ~95% success for grades I–III
NOM monitoring protocol:
- Serial abdominal examinations (4–6 hourly) by same examiner
- Serial haematocrit (4–6 hourly)
- Strict bed rest; nil by mouth initially
- Repeat CT if clinical deterioration
- Consider angioembolisation for CT "blush" (active arterial bleeding) even in haemodynamically stable patients — avoids laparotomy
Failure of NOM → haemodynamic compromise, falling haematocrit, worsening abdominal signs → emergency laparotomy.
11. SPECIFIC ORGAN INJURIES
Spleen
- Most commonly injured organ in BAT
- NOM preferred for grades I–III in stable adults; grades IV–V often require intervention
- Splenic artery angioembolisation (SAE) preserves immunological function and avoids splenectomy
- Splenorrhaphy (repair) preferred over splenectomy when feasible to preserve immunity
- If splenectomy performed → vaccines for Streptococcus pneumoniae, Haemophilus influenzae, Neisseria meningitidis + lifelong penicillin prophylaxis (OPSI — Overwhelming Post-Splenectomy Infection)
Liver
- Second most commonly injured solid organ in BAT; most common in penetrating
- 90–95% managed non-operatively
- Complications of liver injury: haemobilia, biloma, delayed haemorrhage, hepatic necrosis, bile duct injury
Pancreas
- Protected retroperitoneally; injury usually requires significant force (handlebar injury in children)
- Main duct integrity guides management:
- ERCP or MRCP for ductal assessment
- Grade I–II (no ductal injury): wide external drainage
- Grade III (distal duct transaction): distal pancreatectomy ± splenectomy
- Grade IV–V (proximal transaction, ampullary injury): Whipple procedure or damage control + delayed reconstruction
Kidney
- Haematuria (macro or micro) key indicator
- CT urogram gold standard
- Grades I–III: NOM; Grades IV–V: may need embolisation or nephrectomy
Hollow Viscus (Small Bowel, Colon)
- Low incidence (1–5%) but devastating if missed
- Free fluid without solid organ injury on CT = high suspicion for hollow viscus injury
- CT sensitivity only ~80%
- Seat-belt sign, mesenteric stranding, bowel wall thickening are indirect CT signs
- All hollow viscus injuries require operative repair
Diaphragm
- Left-sided rupture 3× more common (liver buttresses right)
- CXR: elevated hemidiaphragm, stomach/bowel loops in chest, NG tube in chest
- CT: best with multiplanar reconstruction
- Repair urgently to prevent strangulation
12. COMPLICATIONS
| Early | Late |
|---|---|
| Haemorrhagic shock | Delayed splenic rupture (days–weeks) |
| Hollow viscus perforation | Post-splenectomy sepsis (OPSI) |
| Abdominal compartment syndrome | Biloma / biliary fistula |
| Missed injury (retroperitoneum) | Pancreatic pseudocyst |
| Coagulopathy (lethal triad) | Hepatic necrosis / abscess |
| Diaphragmatic hernia | Stricture / obstruction |
13. SUMMARY TABLE
| Parameter | Haemodynamically Unstable | Haemodynamically Stable |
|---|---|---|
| First investigation | eFAST (bedside) | eFAST → CT abdomen/pelvis |
| If FAST positive | Emergency laparotomy | CT scan for grading |
| If FAST negative | DPA / DPL → look for extra-abdominal source | Serial exams ± CT |
| Solid organ injury | Damage control laparotomy | NOM ± angioembolisation |
| Hollow viscus | Laparotomy, repair | Laparotomy (all cases) |
| Damage control | Indicated — lethal triad | Not usually required |
KEY POINTS FOR PG EXAM
- Spleen = most commonly injured organ in BAT; liver = most common in penetrating trauma.
- FAST is the first bedside tool; CT is the gold standard in stable patients.
- Clinical examination accuracy in BAT is only 55–65% — do not rely on it alone.
- Positive FAST + haemodynamic instability = immediate laparotomy — do not waste time with CT.
- NOM success rate: 80% spleen (adults), 95% liver — requires institutional readiness.
- Damage control surgery corrects the lethal triad: hypothermia + acidosis + coagulopathy.
- Free fluid without solid organ injury on CT = hollow viscus injury until proven otherwise.
- Post-splenectomy: vaccinate against encapsulated organisms + lifelong prophylaxis.
- Seat-belt sign = strong indicator of hollow viscus and mesenteric injury.
- Angioembolisation is a modern adjunct that can avoid laparotomy in selected cases.
Sources: Rosen's Emergency Medicine 9e (Ch. 38); Mulholland & Greenfield's Surgery 7e (Ch. 25); Current Surgical Therapy 14e; Roberts & Hedges' Clinical Procedures in Emergency Medicine
Principles and management of blunt injury abdomen with flow chats and images in detail for 10 marks long question of pg
The detailed answer has already been provided above in full. Here it is again, cleanly presented for your reference:
Blunt Injury Abdomen — Principles & Management
(10-Mark PG Long Answer)
1. INTRODUCTION & EPIDEMIOLOGY
Blunt abdominal trauma (BAT) accounts for ~75% of all abdominal injuries. Motor vehicle collisions (MVCs) are the most common cause; falls, direct blows, and sports injuries account for the rest. The spleen is the most frequently injured solid organ (in ~2/3 as isolated injury), followed by the liver. Hollow viscus injury occurs in only 1–5% but is associated with high morbidity when missed. Clinical accuracy of physical examination alone is only 55–65%, mandating systematic investigation.
2. MECHANISMS OF INJURY
| Mechanism | Organs Injured |
|---|---|
| Compressive / Crush | Spleen, liver, kidney; bowel rupture from sudden ↑ intraluminal pressure |
| Deceleration / Shear | Hepatic veins, mesentery, renal pedicle at fixed attachment points |
| Direct blow | Contusion, subcapsular haematoma, parenchymal laceration |
| Crush against spine | Pancreas, duodenum (retroperitoneal organs) |
3. PATHOPHYSIOLOGY
- Solid organ injury → parenchymal laceration → hemoperitoneum → haemorrhagic shock
- Hollow viscus perforation → faecal/biliary peritonitis → sepsis → MODS
- Retroperitoneal injury (pancreas, duodenum, great vessels) → occult presentation, delayed diagnosis
- Diaphragmatic rupture → left-sided 3× more common (liver protects right); may present late with visceral herniation
4. CLINICAL ASSESSMENT
History
- Mechanism, speed of impact, seat-belt use, steering-wheel deformation, airbag deployment
- Pre-hospital vitals, fluids given, time elapsed
- Anticoagulants, prior abdominal surgery, comorbidities
Key Signs
| Sign | Significance |
|---|---|
| Guarding, rigidity, rebound tenderness | Peritoneal irritation — blood or enteric content |
| Kehr's sign (left shoulder pain, ↑ in Trendelenburg) | Splenic injury — diaphragmatic irritation |
| Grey Turner's sign (flank bruising, 24–48 h) | Retroperitoneal haematoma |
| Cullen's sign (periumbilical bruising) | Retroperitoneal blood tracking anteriorly |
| Seat-belt sign (abdominal wall ecchymosis) | ↑↑ risk of hollow viscus & mesenteric injury |
| Haematuria | Renal / bladder trauma |
| Blood at urethral meatus | Urethral injury — do NOT catheterise |
| Left lower rib fractures | Splenic injury |
| Right lower rib fractures | Hepatic injury |
5. INVESTIGATIONS
5a. Laboratory
- Serial FBC (haematocrit trending), coagulation profile (PT/APTT/INR)
- Arterial blood gas — base deficit and lactate as shock markers
- Serum amylase/lipase (pancreatic injury)
- LFTs, urinalysis, group & crossmatch
- Activate Massive Transfusion Protocol (MTP) if ≥10 units PRBCs anticipated in 24 h
5b. eFAST Examination
The first-line bedside investigation, performed simultaneously with resuscitation — answers one question: Is there free intraperitoneal fluid (hemoperitoneum)?
Four standard windows + extended (eFAST):
| Window | Structure Examined |
|---|---|
| Subxiphoid (pericardial) | Pericardial effusion / cardiac tamponade |
| Right upper quadrant | Morison's pouch — hepatorenal space |
| Left upper quadrant | Splenorenal recess |
| Suprapubic (pelvic) | Pouch of Douglas / rectovesical pouch |
| Bilateral thoracic | Pneumothorax / haemothorax (eFAST) |
Positive FAST = anechoic (black) free fluid between organs = hemoperitoneum
FAST pelvis: Anechoic free fluid adjacent to bladder indicating hemoperitoneum
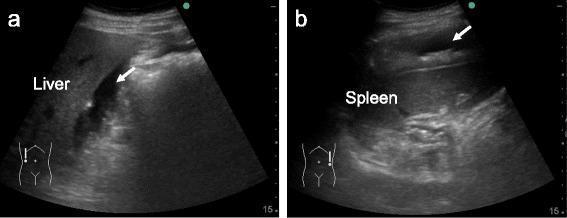
(a) Free fluid in Morison's pouch between liver and right kidney; (b) perisplenic free fluid — both confirm hemoperitoneum
Limitations: Suboptimal for retroperitoneal and hollow viscus injuries. Negative FAST does not exclude significant injury.
5c. CT Abdomen & Pelvis with IV Contrast
Gold standard for BAT in the haemodynamically stable patient.
- Sensitivity ~95% for solid organ injuries
- Sensitivity ~80% for hollow viscus injury (imperfect)
- Free fluid without solid organ injury = high suspicion for hollow viscus perforation
Key CT findings:
| Finding | Implication |
|---|---|
| Hyperdense free fluid | Hemoperitoneum |
| Parenchymal laceration (hypodense) | Solid organ injury |
| Active contrast "blush" | Ongoing arterial bleeding → angioembolisation |
| Free air | Hollow viscus perforation |
| Mesenteric stranding / haematoma | Mesenteric / hollow viscus injury |
| Pancreatic oedema / ductal disruption | Pancreatic injury |
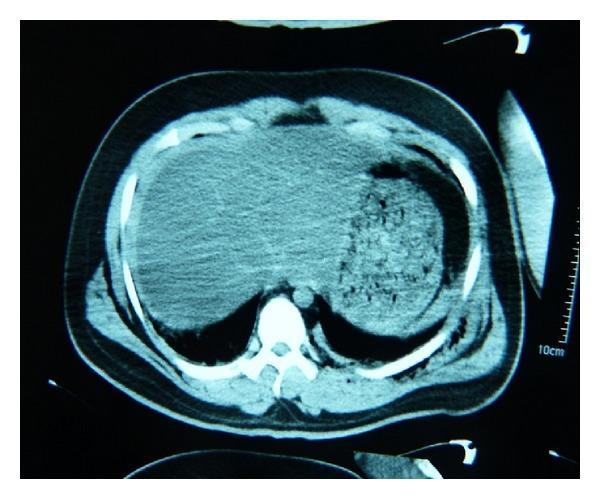
CT axial: Hypodense perihepatic and perisplenic free fluid (hemoperitoneum)
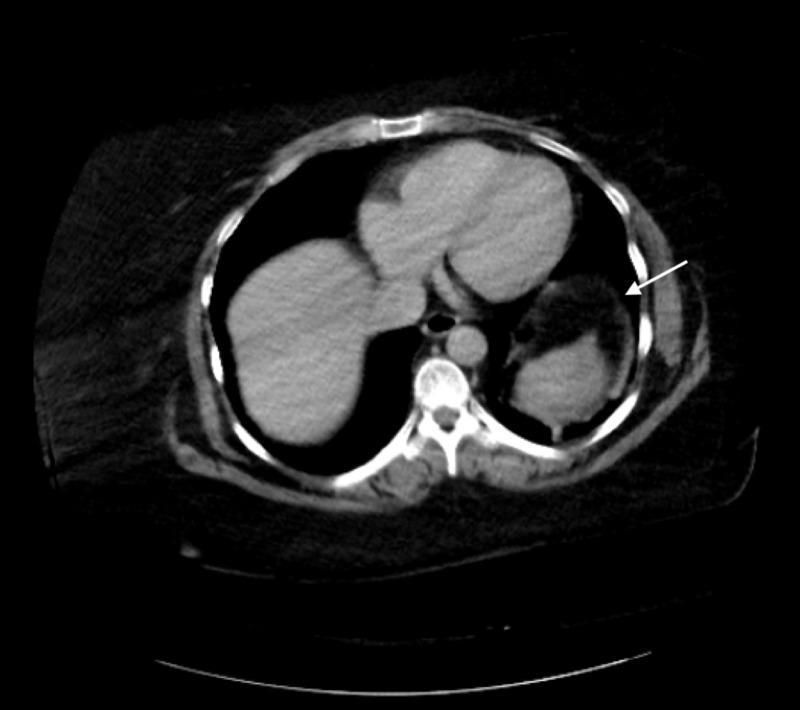
CT: Grade III splenic laceration — subcapsular hematoma with parenchymal tear >3 cm
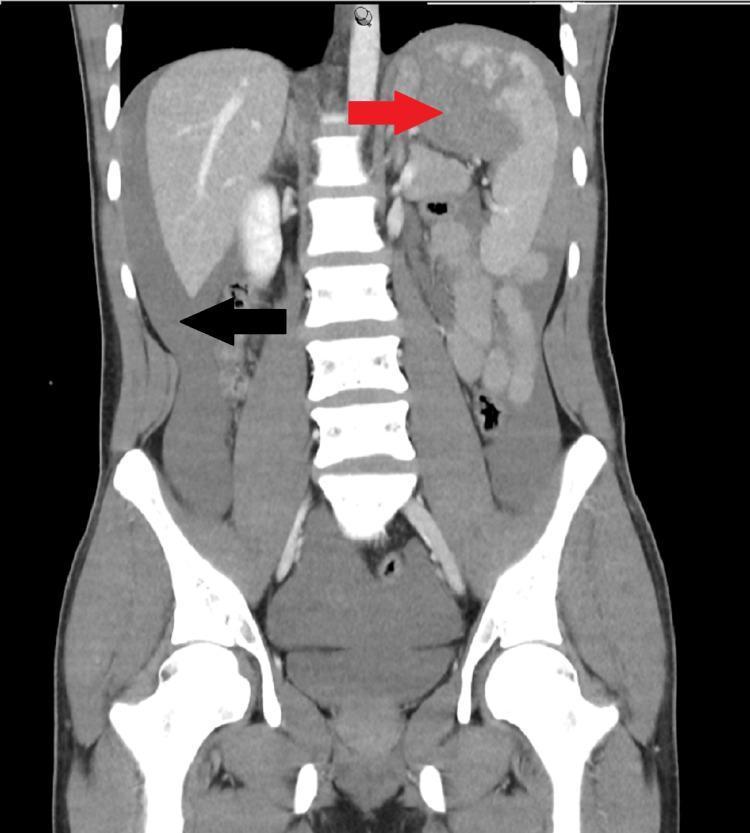
CT coronal: Grade IV splenic laceration (red arrow) with massive hemoperitoneum in paracolic gutters (black arrow)
CT: Pancreatic laceration (hypodense, body-tail junction) with surrounding free fluid
5d. Diagnostic Peritoneal Lavage (DPL)
Largely replaced by FAST + CT but useful when these are unavailable.
Positive criteria:
- Gross blood on aspiration (≥10 mL)
- RBC >100,000/mm³
- WBC >500/mm³ (after 3 hours)
- Bile, bacteria, food fibres
Sensitivity >98%; does NOT detect retroperitoneal injuries; cannot identify organ-specific injury.
5e. Plain Radiographs
- CXR: Pneumothorax, haemothorax, rib fractures, elevated hemidiaphragm, bowel loops in chest
- AXR: Free gas under diaphragm (perforation), loss of psoas shadow (retroperitoneal haematoma), pelvic fractures
6. AAST ORGAN INJURY GRADING
Liver (AAST-OIS)
| Grade | Injury |
|---|---|
| I | Subcapsular haematoma <10% surface; capsular tear <1 cm deep |
| II | Subcapsular haematoma 10–50%; laceration 1–3 cm deep, <10 cm long |
| III | Subcapsular haematoma >50% or ruptured; laceration >3 cm deep |
| IV | Parenchymal disruption 25–75% of a hepatic lobe |
| V | >75% lobar disruption; retrohepatic IVC / major hepatic vein injury |
| VI | Hepatic avulsion (universally lethal) |
Spleen (AAST-OIS)
| Grade | Injury |
|---|---|
| I | Subcapsular haematoma <10%; capsular laceration <1 cm deep |
| II | Subcapsular haematoma 10–50%; laceration 1–3 cm deep, not involving trabecular vessels |
| III | Subcapsular haematoma >50% or expanding; laceration >3 cm involving trabecular vessels |
| IV | Injury involving segmental/hilar vessels → >25% devascularisation |
| V | Shattered spleen; hilar vascular injury → complete devascularisation |
7. MANAGEMENT FLOWCHARTS
FLOWCHART 1 — Master BAT Algorithm (Rosen's Emergency Medicine)
BAT Algorithm: Starting with BAT mechanism → clinical mandate for laparotomy? → haemodynamic stability? → FAST/DPA → CT/DPL/SPEs → decision: Laparotomy / Observe / Discharge
FLOWCHART 2 — Haemodynamically Stable Patient
Stable patient: Reliable PE? → CT or ultrasound → free fluid/hollow viscus/solid organ findings guide exploratory laparotomy vs. non-operative management vs. admission with serial PE
8. INITIAL RESUSCITATION (ATLS Framework)
A — Airway + C-spine control (jaw thrust; intubate if GCS ≤8)
B — Breathing: decompress tension pneumothorax, drain haemothorax
C — Circulation: 2 large-bore IVs; Damage Control Resuscitation — blood products in 1:1:1 ratio (PRBCs : FFP : Platelets)
Permissive hypotension (SBP 80–90 mmHg) may be tolerated briefly before definitive haemorrhage control to reduce dilutional coagulopathy — prevents clot disruption while awaiting OR.
- NGT decompression (OGT if midface fracture)
- Urinary catheter for hourly urine output (minimum 0.5 mL/kg/h)
- Warming (prevent hypothermia — part of lethal triad)
- Activate MTP early if haemodynamically unstable
9. OPERATIVE MANAGEMENT
Indications for Emergency Laparotomy in BAT
| Indication | Note |
|---|---|
| Haemodynamic instability + positive FAST | Source = intraperitoneal haemorrhage |
| Peritonitis (rigid abdomen, diffuse rebound) | Hollow viscus injury |
| Pneumoperitoneum | Hollow viscus perforation |
| Evisceration | Immediate surgery |
| Diaphragmatic rupture | Prevent strangulation |
| DPL gross blood or RBC >100,000/mm³ | Where FAST/CT unavailable |
| FAST + concomitant life-threatening injury requiring OR | Combined injuries |
Operative Steps
- Position: Supine, arms abducted 90°; chest, abdomen, pelvis prepped
- Incision: Midline laparotomy — xiphoid to pubis
- Initial control: Four-quadrant packing — control haemorrhage first
- Systematic exploration: All 9 abdominal regions, retroperitoneum, mesentery
- Contamination control: Staple/close perforations rapidly
- Definitive repair or damage control decision
Damage Control Surgery (DCS) — The "Lethal Triad"
Indicators: Any two of:
- Hypothermia (<35°C)
- Acidosis (pH <7.2, base deficit >−6, lactate >5)
- Coagulopathy (INR >1.5, PT >50% above normal)
Three-Phase DCS:
Phase I (OR) ─────────────────────────────────────────────────
│ Haemorrhage control (pack, clip, vascular shunts)
│ Contamination control (staple off perforations)
│ Temporary abdominal closure (TAC — Bogotá bag / vacuum)
▼
Phase II (ICU) ────────────────────────────────────────────────
│ Correct hypothermia (warm IV fluids, warming blankets)
│ Correct coagulopathy (FFP, platelets, cryoprecipitate)
│ Correct acidosis (resuscitation, vasopressors)
│ Ventilatory support, renal support
▼
Phase III (Return to OR at 24–48 h) ──────────────────────────
Definitive bowel anastomosis
Formal vascular repair
Fascial closure (or staged closure)
Angioembolisation — critical adjunct for ongoing hepatic, splenic, or pelvic arterial haemorrhage; can be performed alongside or instead of operative intervention.
Abdominal Compartment Syndrome (ACS)
- IAP >20 mmHg + new organ dysfunction = ACS
- Monitor with bladder pressure post-laparotomy
- Treat with decompressive laparotomy
10. NON-OPERATIVE MANAGEMENT (NOM)
Prerequisites
- Haemodynamic stability (SBP >90 mmHg, HR <100)
- Reliable, evaluable patient (alert, cooperative)
- No peritonitis
- No hollow viscus injury on CT
- Institutional readiness: trauma surgeon available, blood bank, OR on standby
Success Rates
- Blunt splenic injury: ~80% adults, 90–95% children
- Blunt hepatic injury: ~95% for grades I–III
NOM Monitoring Protocol
- Serial abdominal examination every 4–6 hours by same examiner
- Serial haematocrit every 4–6 hours
- Strict bed rest; nil by mouth initially
- Repeat CT if haemodynamic or clinical deterioration
- Angioembolisation for CT "blush" (arterial extravasation) even in stable patients
Failure of NOM → Emergency Laparotomy
- Haemodynamic compromise
- Falling haematocrit despite transfusion
- Worsening abdominal signs
- New peritonitis
11. SPECIFIC ORGAN MANAGEMENT
Spleen
- NOM: grades I–III in stable adults; grades IV–V may need intervention
- Splenic artery angioembolisation (SAE): Preserves immunological function; reduces failure of NOM in high-grade injuries
- Splenorrhaphy (repair) preferred over splenectomy when feasible
- Post-splenectomy: Vaccinate against S. pneumoniae, H. influenzae type b, N. meningitidis + lifelong prophylactic penicillin (prevents OPSI)
Liver
- ~95% managed non-operatively
- Complications: haemobilia, biloma, bile leak, delayed haemorrhage, hepatic abscess
- Angioembolisation for active arterial bleeding
- Surgery: Pringle manoeuvre (hepatoduodenal ligament compression), packing, tractotomy
Pancreas (AAST Grading Guides Management)
| Grade | Injury | Management |
|---|---|---|
| I–II | Contusion/superficial laceration; duct intact | External drainage |
| III | Distal ductal transaction | Distal pancreatectomy ± splenectomy |
| IV | Proximal ductal injury / ampullary involvement | Wide drainage; consider Whipple |
| V | Massive head disruption | Damage control → staged Whipple |
Hollow Viscus (Small Bowel / Colon)
- All require operative repair — no NOM
- CT signs: free fluid without solid organ injury, mesenteric stranding, bowel wall thickening, free air
- Small bowel: primary repair (if <50% circumference) or segmental resection + anastomosis
- Colon: primary repair (right/transverse); Hartmann's or diversion for left colon in contaminated field
Kidney
- AAST Grade I–III: NOM (>95% success)
- Grade IV–V: angioembolisation or nephrectomy
- Always perform one-shot IVP (10 mL/kg IV contrast, KUB at 10 min) pre-operatively if time allows, to confirm contralateral kidney function
Diaphragm
- CXR: nasogastric tube in chest, bowel loops above diaphragm, elevated hemidiaphragm
- CT with multiplanar reconstruction: best diagnostic modality
- Repair urgently — risk of visceral herniation and strangulation
12. COMPLICATIONS
| Early (<48 h) | Late (>48 h) |
|---|---|
| Haemorrhagic shock, DIC | Delayed splenic rupture |
| Hollow viscus missed injury | Post-splenectomy sepsis (OPSI) |
| Abdominal compartment syndrome | Biloma / biliary fistula |
| Lethal triad | Pancreatic pseudocyst / fistula |
| Vascular injury, aortic disruption | Hepatic necrosis / abscess |
| Diaphragmatic herniation | Adhesive bowel obstruction |
13. SUMMARY — THE DECISIVE PIVOT POINT
BLUNT ABDOMINAL TRAUMA
│
▼
HAEMODYNAMICALLY
UNSTABLE?
┌─────┴─────┐
YES NO
│ │
▼ ▼
eFAST CT Abdomen/Pelvis
(+ve) (Gold Standard)
│ │
▼ ┌───┴────┐
EMERGENCY NOM Laparotomy
LAPAROTOMY │ (hollow viscus,
+ DCL Angio- peritonitis,
embolism failure NOM)
KEY PG EXAM POINTS
- Spleen = most commonly injured in BAT; liver = most common in penetrating trauma
- Clinical exam accuracy in BAT = only 55–65% — never rely on it alone
- FAST + haemodynamic instability = immediate laparotomy — no time for CT
- CT is gold standard in stable patients; sensitivity ~95% solid organs, ~80% hollow viscus
- Free fluid without solid organ injury on CT = hollow viscus injury until proven otherwise
- Seat-belt sign = strong predictor of hollow viscus and mesenteric injury
- NOM success: ~80% spleen (adults), ~95% liver — institution must be prepared
- Damage control surgery for lethal triad: hypothermia + coagulopathy + acidosis
- Angioembolisation — modern alternative/adjunct; avoids laparotomy, preserves organs
- Post-splenectomy: vaccinate (pneumococcal, Hib, meningococcal) + prophylactic penicillin lifelong
Sources: Rosen's Emergency Medicine 9e (Ch. 38); Mulholland & Greenfield's Surgery 7e (Ch. 25); Current Surgical Therapy 14e; Roberts & Hedges' Clinical Procedures in Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.