Double elevator palsy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Searching Images
double elevator palsy monocular elevation deficiency
Loading Image
Now I have comprehensive information to provide a thorough answer on double elevator palsy.
Double Elevator Palsy (Monocular Elevation Deficiency)
Definition
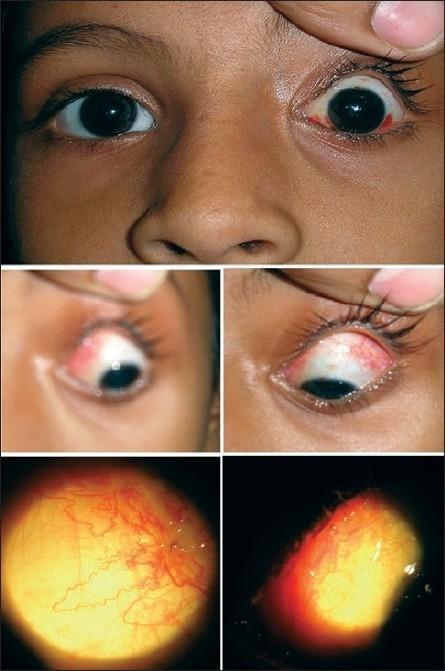
Double elevator palsy (DEP), also termed monocular elevation deficiency (MED) or monocular elevator palsy, is a condition characterized by unilateral limitation of elevation in all fields of gaze — both in adduction and abduction. Both elevators of the eye (superior rectus and inferior oblique) are functionally impaired, hence "double" elevator palsy.
This distinguishes it from Brown syndrome, where limitation of elevation is predominantly in adduction (not all fields).
Etiology
DEP can be supranuclear, infranuclear, or restrictive in origin:
Supranuclear (most common in acquired cases)
- Pretectal lesions contralateral to the paretic eye, or ipsilateral lesions interrupting efferents from the rostral interstitial nucleus of the MLF (riMLF) to the superior rectus and inferior oblique subnuclei
- Bell phenomenon (reflex upgaze on eye closure) is often intact in supranuclear lesions, distinguishing them from infranuclear causes
- May represent an asymmetric upgaze palsy presenting clinically as monocular elevation paresis in the more severely affected eye
- Paramedian midbrain infarcts affecting the lateral fascicular portion of the oculomotor nerve
Infranuclear / Neuromuscular
- Fascicular lesions of the oculomotor nerve
- Myasthenia gravis
- Orbital floor fractures (restrictive)
- Thyroid orbitopathy
- Infiltrative orbital disease
Congenital
- Most cases are congenital, likely supranuclear (congenital unilateral midbrain lesion)
- Over time, the inferior rectus undergoes restriction and fibrosis, preventing reflex elevation — even Bell phenomenon becomes absent in longstanding cases
Clinical Features
| Feature | Detail |
|---|---|
| Elevation deficit | Unilateral, equal in adduction and abduction |
| Hypotropia | Involved eye deviated down; increases in upgaze |
| Ptosis or pseudoptosis | Ptosis may be true (levator involvement) or pseudo (lid follows hypotropic eye in fixation with the fellow eye) |
| Head position | Chin-up posture to maintain fusion |
| Bell phenomenon | May be absent (infranuclear/restrictive) or preserved (supranuclear) |
| Amblyopia | Common in congenital cases |
| Convergence abnormalities | May be present in congenital cases |
Key clinical pearl: When the patient fixates with the hypotropic eye, pseudoptosis disappears. When they fixate with the fellow eye, the lid follows the hypotropic eye and appears ptotic.
Pathophysiology
The two elevators of the eye are:
- Superior rectus — innervated by CN III (contralateral superior rectus subnucleus)
- Inferior oblique — innervated by CN III (ipsilateral inferior oblique subnucleus)
Supranuclear control of upgaze involves the riMLF projecting bilaterally to both elevator muscle subnuclei. A lesion in this pathway can selectively impair monocular elevation.
In congenital cases, prolonged disuse leads to secondary inferior rectus contracture/fibrosis, adding a restrictive component on top of the original paretic/supranuclear cause.
Investigations
- Forced duction testing — critical for distinguishing the two mechanisms:
- Positive (restricted): inferior rectus fibrosis/restriction
- Negative (not restricted): superior rectus and inferior oblique paresis
- MRI brain/orbits — for acquired, atypical, or progressive cases to identify midbrain/thalamic lesions
- CT orbits — if orbital floor fracture suspected
- Tensilon (edrophonium) test / anti-AChR antibodies — if myasthenia suspected
- Thyroid function tests / orbital imaging — if thyroid orbitopathy suspected
Treatment
Treatment is indicated for:
- Cosmetically significant head posture (chin-up)
- Significant hypotropia in primary gaze
Surgery — Knapp Procedure (procedure of choice)
- Full transposition of the medial and lateral rectus muscles to the insertion of the superior rectus (adjacent to it)
- This converts the horizontal recti into supplementary elevators
- Works regardless of the underlying mechanism (paretic or restrictive)
If inferior rectus restriction is identified:
- Inferior rectus recession ± Knapp procedure
Ptosis correction:
- Addressed after the vertical deviation is corrected, as pseudoptosis may resolve
- True ptosis requires levator resection or frontalis sling (if poor levator function)
Summary
| Aspect | Key Point |
|---|---|
| Core deficit | Unilateral elevation limitation in all gaze positions |
| Both elevators affected | Superior rectus + inferior oblique (hence "double") |
| Differentiator from Brown syndrome | Brown is limited to elevation in adduction only |
| Congenital vs acquired | Usually congenital; acquired → rule out midbrain lesion |
| Bell phenomenon intact | Suggests supranuclear etiology |
| Forced ductions | Distinguish restrictive (IR fibrosis) from paretic cause |
| Surgery of choice | Knapp procedure (transposition of MR + LR to SR insertion) |
Sources: The Wills Eye Manual, 8e; Bradley and Daroff's Neurology in Clinical Practice; Localization in Clinical Neurology, 8e
This is a shared conversation. Sign in to Orris to start your own chat.