Bp rate is 156/63 ,an 80+ years old patient complain about dizziness
Reading File
Finding Sources
Finding Sources
Searching PubMed
isolated systolic hypertension elderly dizziness management
Finding Sources
Finding Sources
Searching PubMed
hypertension elderly octogenarian treatment
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Searching the Web
2025 hypertension guidelines elderly 80 years old isolated systolic hypertension dizziness management
I now have comprehensive information to provide a detailed clinical answer. Here is my full response:
Clinical Assessment: BP 156/63 mmHg + Dizziness in an 80+ Year-Old Patient
What This Blood Pressure Pattern Means
This patient has Isolated Systolic Hypertension (ISH) with a wide pulse pressure of 93 mmHg (normal is ~40 mmHg). In patients over 80, this pattern is caused by progressive aortic stiffness and arteriosclerosis - the large arteries lose compliance, so systolic pressure rises while diastolic stays low or normal. This is the most common form of hypertension in the very elderly.
Key observations:
- SBP 156 mmHg - elevated, above the HYVET trial's treatment threshold of 150 mmHg
- DBP 63 mmHg - already on the lower end; must not be pushed further down
- Pulse pressure 93 mmHg - markedly widened, indicating significant arterial stiffness
Why the Dizziness? - Differential Diagnosis
Dizziness in this context has several likely causes that must be distinguished:
| Cause | Mechanism | Key Feature |
|---|---|---|
| Orthostatic hypotension | BP drops on standing due to blunted baroreflexes | Dizziness on standing up |
| Postprandial hypotension | Splanchnic pooling after meals | Dizziness 30-60 min after eating |
| Cerebral hypoperfusion | Low DBP reduces coronary/cerebral perfusion | Can occur even with high SBP |
| Over-treatment / J-curve effect | DBP pushed too low by antihypertensives | Worse on medication |
| Vertebrobasilar insufficiency | Atherosclerosis of posterior circulation | Positional, with nystagmus |
| Cardiac arrhythmia | Common at this age | Check ECG |
| Anemia / dehydration | Reduced perfusion globally | Lab work needed |
| White coat hypertension | BP is actually lower at home | 24-hr ABPM resolves this |
The 24-hour ambulatory BP monitoring (ABPM) tracing below illustrates exactly this clinical picture - a frail elderly patient with labile hypertension and dizziness, showing postprandial drops (blue arrows) and orthostatic drops when walking to the bathroom (red arrow):
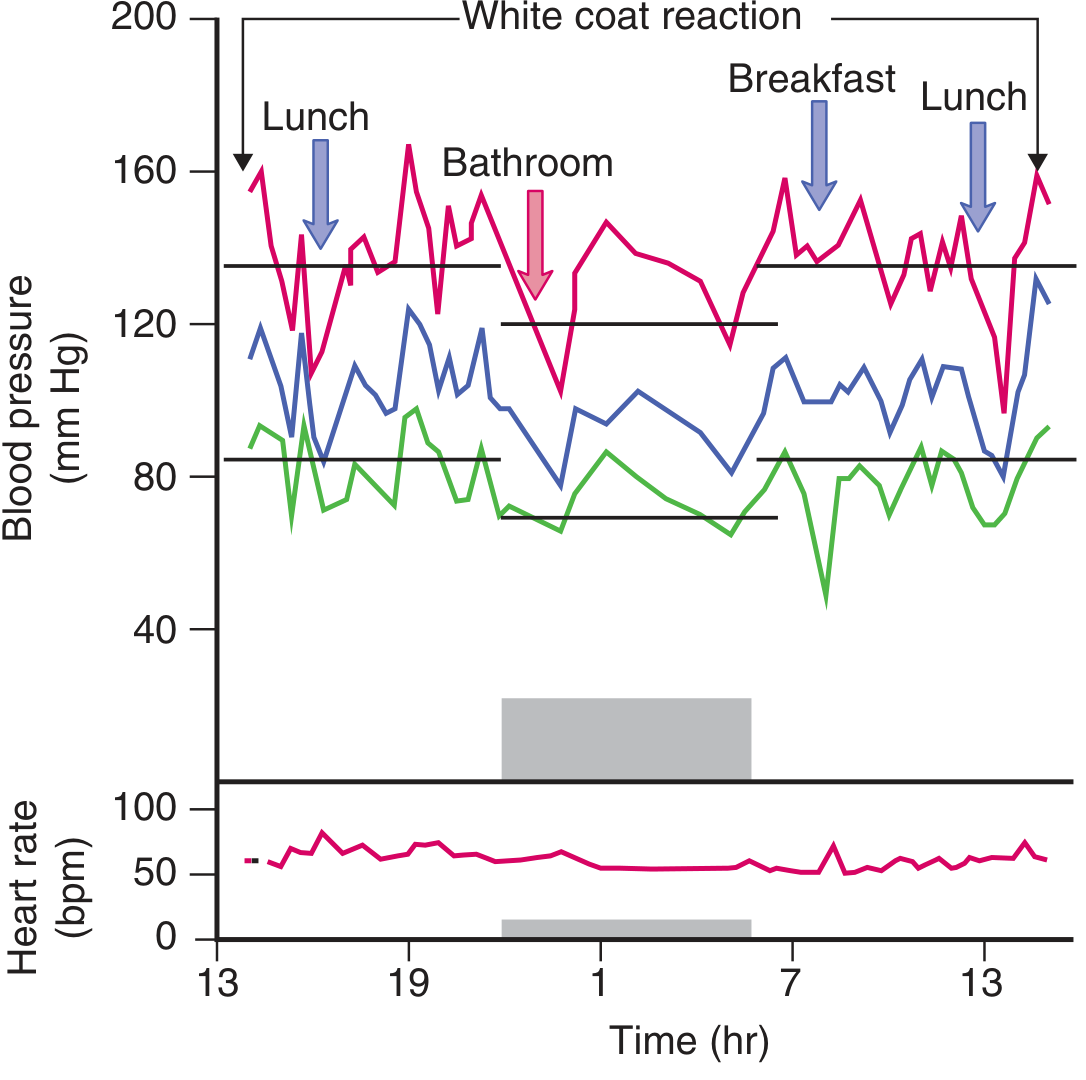
(Goldman-Cecil Medicine - 24-hr BP monitor of a frail 70-year-old with labile hypertension and dizziness. Similar pattern applies to this 80+ patient.)
Blood Pressure Treatment Targets in the Very Elderly (80+)
The landmark HYVET trial (2008) enrolled ~4,000 patients aged 80+ with systolic BP ≥160 mmHg. Targeting SBP < 150/80 mmHg using indapamide ± perindopril reduced:
- Stroke by 30%
- All-cause mortality by 21%
- Heart failure by 64%
Current guideline targets for age 80+:
| Guideline | SBP Target |
|---|---|
| 2025 AHA/ACC | <130/80 mmHg (risk-based; in fit patients) |
| 2024 ESC / ESH | 140-150 mmHg (ALARA principle for frail/very elderly) |
| HYVET evidence | <150/80 mmHg is well-supported |
| JNC 7 minimum DBP | Do not let DBP drop below 60 mmHg (65 mmHg if CAD present) |
The 2025 AHA/ACC vs ESC debate shows divergence here: the ESC explicitly uses ALARA ("as low as reasonably achievable") for the very elderly and accepts less stringent targets, while AHA/ACC still pursues <130 mmHg in fit patients. Given this patient's DBP is already 63 mmHg, aggressive lowering carries real risk.
Critical J-curve concern: In patients with isolated systolic hypertension, reducing diastolic BP too far can cause myocardial ischemia. The identified nadir is ~119/84 mmHg in CAD patients; below a DBP of 60-65 mmHg, coronary perfusion is compromised. - Brenner and Rector's The Kidney, 2-Volume Set
Immediate Workup Recommended
- Orthostatic BP check - measure BP lying, sitting, and standing (after 1 and 3 minutes). A drop of >20 mmHg systolic or >10 mmHg diastolic on standing = orthostatic hypotension
- 12-lead ECG - rule out arrhythmia, LVH, ischemia
- 24-hr ambulatory BP monitoring (ABPM) - look for postprandial/orthostatic drops, white coat effect, and true BP burden
- Basic labs - CBC (anemia), BMP (renal function, electrolytes), BG (hypoglycemia)
- Medication review - is patient already on antihypertensives, alpha-blockers, diuretics, or other agents that could cause BP drops?
- Echocardiogram - if LVH, diastolic dysfunction, or aortic stenosis suspected (aortic stenosis is common in this age group and causes ISH + dizziness)
Treatment Approach
First, confirm this is not over-treated ISH causing dizziness. If the patient is already on antihypertensives and the DBP is 63, the dizziness may be the J-curve effect.
If treatment/intensification is needed:
- Preferred drugs for ISH in the elderly: Thiazide-like diuretics (indapamide, chlorthalidone) and long-acting dihydropyridine CCBs (amlodipine) - these have the strongest trial evidence (SHEP, Syst-Eur, HYVET trials)
- ACE inhibitor can be added as second agent (as per HYVET protocol: indapamide + perindopril)
- Avoid: Beta-blockers as first line (less effective for ISH), alpha-blockers (worsen orthostatic hypotension), short-acting CCBs
- Start low, go slow - frail elderly have reduced baroreceptor reflexes and are highly susceptible to over-correction
Non-pharmacological:
- Rise from sitting/lying slowly
- Small, frequent meals (reduces postprandial hypotension)
- Adequate hydration
- Compression stockings if orthostatic hypotension confirmed
- Fall risk assessment - dizziness in this age group = fracture risk
Bottom Line
This patient's BP of 156/63 with dizziness in an 80+ year-old is a classic picture of isolated systolic hypertension with wide pulse pressure and likely orthostatic or postprandial hypotension causing the dizziness. The SBP of 156 does warrant treatment (above the HYVET threshold of 150), but the already-low DBP of 63 means treatment must be cautious. Check orthostatic vitals and a 24-hr ABPM before adjusting medications. Target SBP < 150 mmHg without letting DBP fall below 60-65 mmHg.
Note: This information is for clinical guidance only. Management decisions must be individualized by the treating physician based on the full clinical picture, comorbidities, frailty status, and patient preferences.
This is a shared conversation. Sign in to Orris to start your own chat.