Brachial plexus clinical correlations
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
I now have rich, comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Brachial Plexus - Clinical Correlations
Anatomy Overview
The brachial plexus is formed by the anterior rami of C5-T1, passing between the anterior and middle scalene muscles before entering the axilla. Its organization follows a consistent pattern:

Fig. 7.52 - Gray's Anatomy for Students: Brachial plexus components including roots, trunks, divisions, and cords in the neck and axilla
| Level | Structure | Composition |
|---|---|---|
| Roots | Anterior rami | C5, C6, C7, C8, T1 |
| Trunks | Superior | C5 + C6 |
| Middle | C7 alone | |
| Inferior | C8 + T1 | |
| Divisions | Anterior + Posterior | From each trunk |
| Cords | Lateral | Anterior divisions of superior + middle trunks |
| Medial | Anterior division of inferior trunk | |
| Posterior | All three posterior divisions |
The cords are named for their relationship to the axillary artery. Terminal branches arise from the cords: musculocutaneous (lateral cord), axillary and radial (posterior cord), and median (lateral + medial cords) and ulnar (medial cord).
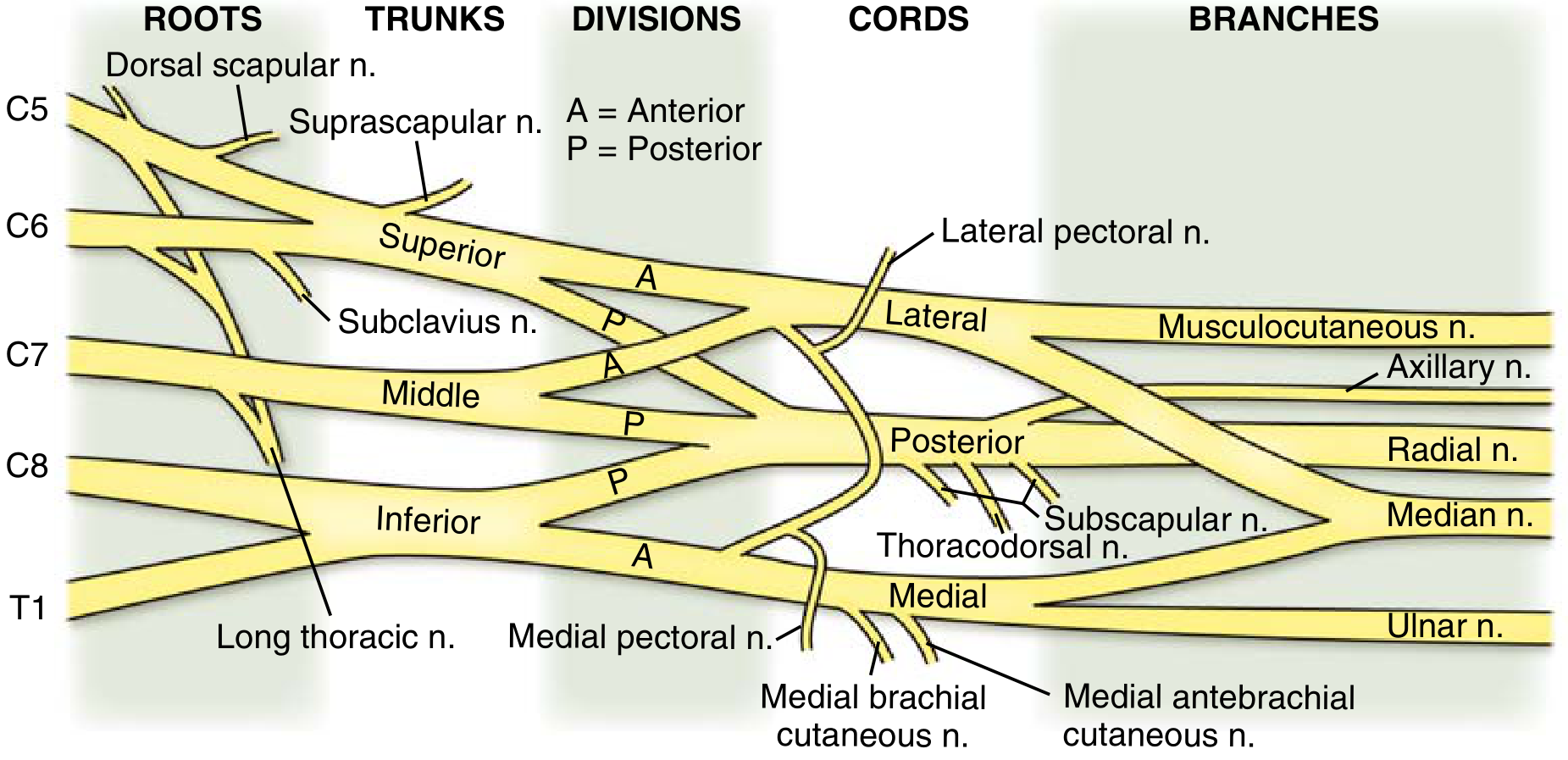
Miller's Review of Orthopaedics: Complete brachial plexus schematic from C5-T1 roots to terminal nerves
Pre-Trunk Branches (Supraclavicular)
These arise proximal to the trunks and are clinically important because their injury helps localize the lesion level:
| Nerve | Origin | Muscle | Clinical sign |
|---|---|---|---|
| Dorsal scapular n. | C5 root | Rhomboids | Winging of scapula (with serratus palsy) |
| Long thoracic n. | C5, C6, C7 roots | Serratus anterior | Winging of scapula - the vertebral border becomes prominent |
| Suprascapular n. | Upper trunk (C5, C6) | Supraspinatus, Infraspinatus | Shoulder abduction and external rotation weakness |
| Nerve to subclavius | Upper trunk (C5, C6) | Subclavius | Clinically silent |
Classic Plexus Injury Syndromes
1. Erb's Palsy (Erb-Duchenne) - Upper Trunk Injury (C5, C6)
Mechanism: Forcible widening of the angle between the neck and shoulder. Occurs in:
- Difficult delivery (head pulled while shoulder is arrested) - commonest obstetric injury, 0.4-4% of live births
- Fall of a load on the shoulder
- Motorcycle accidents; forced shoulder depression
Structures damaged: Superior trunk (C5, C6) - suprascapular nerve, musculocutaneous nerve, and axillary nerve are most affected.
Deformity - "Waiter's tip" / "Policeman's tip" position:
- Arm hangs adducted and internally rotated at the shoulder (deltoid + supraspinatus weakness)
- Elbow extended (loss of biceps/brachialis)
- Forearm pronated (loss of supinator)
- Wrist and fingers are in slight flexion (extensors are weakened)
Motor losses:
- Deltoid (axillary n.) - abduction of arm above 15°
- Supraspinatus/infraspinatus (suprascapular n.) - abduction initiation, external rotation
- Biceps/brachialis (musculocutaneous n.) - elbow flexion
- Brachioradialis - weakened
Reflexes lost: Biceps jerk (C5, C6), brachioradialis reflex
Sensory loss: Lateral aspect of arm and forearm (C5, C6 dermatomes)
Obstetric Erb's palsy prognosis: Over 90% resolve by 3 months. Biceps function is the key prognostic indicator. Surgical plexus reconstruction is considered at 3 months if no spontaneous recovery. - Miller's Review of Orthopaedics, p. 156; Bradley and Daroff's Neurology, p. 2870
2. Klumpke's Palsy - Lower Trunk Injury (C8, T1)
Mechanism: Forcible hyperabduction of the arm (e.g., catching a support while falling, birth traction with arm over head). Less common than Erb's palsy.
Structures damaged: Inferior trunk (C8, T1) → medial cord → ulnar nerve and medial head of median nerve are primarily affected.
Deformity - "Claw hand" (Main en griffe):
- Hyperextension at metacarpophalangeal joints
- Flexion at proximal and distal interphalangeal joints
- Due to paralysis of intrinsic hand muscles (interossei and lumbricals)
- The flexor digitorum profundus and superficialis are intact, but unopposed - they pull the IP joints into flexion; the absent intrinsics cannot extend the IP joints
Motor losses:
- All intrinsic muscles of the hand (interossei, hypothenar, thenar - especially abductor pollicis brevis)
- Flexors of the wrist and fingers may be affected in severe cases
Reflexes lost: Finger jerk; triceps jerk may be affected if C8 root is involved
Sensory loss: Medial aspect of the forearm and hand (C8, T1) - ulnar 1.5 digits and medial forearm
Horner's syndrome: When T1 root is avulsed, sympathetic fibers (which travel with T1 gray rami communicantes to the stellate ganglion) are disrupted → ipsilateral ptosis, miosis, enophthalmos, and anhidrosis - S Das Manual of Clinical Surgery, p. 127; Schwartz's Principles of Surgery, p. 1876
3. Complete Brachial Plexus Injury (C5-T1)
- Rarest and most severe type
- Flail arm: total loss of motor function in the upper limb
- Complete sensory loss
- Associated with high-velocity trauma (motorcyclists)
- Horner's syndrome indicates root avulsion at T1
Individual Nerve Injury Correlations
Axillary Nerve (C5, C6) - Posterior cord
Common causes: Anterior shoulder dislocation, fracture of the surgical neck of humerus, intramuscular injections in the deltoid (quinine), direct blows to the lateral shoulder
Deficits:
- Deltoid paralysis → loss of arm abduction beyond 15° and forward flexion
- Teres minor paralysis → loss of external rotation
- Sensory loss: "Regimental badge area" - lateral aspect of the proximal arm
Test: Ask patient to abduct the arm against resistance. Look for flattening of the shoulder contour.
Musculocutaneous Nerve (C5, C6, C7) - Lateral cord
Common causes: Coracobrachialis entrapment, penetrating injuries
Deficits:
- Biceps and brachialis paralysis → loss of elbow flexion (most powerful in supination)
- Coracobrachialis weakness
- Sensory loss: Lateral forearm (lateral cutaneous nerve of the forearm)
Radial Nerve (C5-T1) - Posterior cord
Classic injury site - Spiral groove of humerus (mid-shaft humeral fracture or "Saturday night palsy"):
Deficits:
- Wrist drop - inability to extend the wrist; the hand hangs limp in flexion at the wrist
- Loss of finger and thumb extension (extensor digitorum, extensor pollicis longus/brevis)
- Weakened elbow flexion in the mid-prone position (brachioradialis)
- Triceps is spared in spiral groove injuries (triceps branch arises more proximally)
Axillary injury (above spiral groove, e.g., crutch palsy): Triceps weakness is added to the above picture.
Posterior interosseous nerve (deep branch): No sensory loss; only finger drop (cannot extend MCPJs); wrist can still be extended (radial wrist extensors are spared because they arise before the nerve enters the radial tunnel).
Sensory loss: Dorsum of hand and lateral 3.5 digits (superficial radial nerve)
- Schwartz's Principles of Surgery, p. 1876
Median Nerve (C6-T1) - Lateral + Medial cords
Carpal tunnel (most common entrapment site):
- Night pain, waking from sleep, shaking the hand for relief
- Thenar wasting (abductor pollicis brevis)
- Positive Tinel's and Phalen's tests
- Sensory loss: Lateral 3.5 digits (palm side)
Anterior interosseous nerve syndrome (pure motor branch):
- Loss of flexor pollicis longus + flexor digitorum profundus to index and middle fingers
- "OK sign" failure - patient cannot make a precise pinch (the distal phalanges extend instead of flexing, producing a flattened pinch)
High median nerve injury (above elbow, e.g., supracondylar fracture):
- All above + loss of wrist flexion (flexor carpi radialis)
- Partial loss of finger flexion (FDP to ring/little = intact, supplied by ulnar)
- "Pointing index" / "Pope's blessing" deformity: When trying to make a fist, the index and middle fingers remain relatively extended because their FDP is non-functional, but the ring and little fingers flex normally
Sensory loss: Lateral palm, lateral 3.5 digits including tips of index and thumb (critical for fine sensation)
Ulnar Nerve (C8, T1) - Medial cord
Common injury sites:
- Medial epicondyle / cubital tunnel (most common entrapment)
- Guyon's canal at the wrist
Deficits:
- Claw hand - particularly pronounced in ring and little fingers (ulnar two digits); less severe than Klumpke's because the lumbricals to index and middle fingers (supplied by median nerve) still function → "ulnar paradox" (low ulnar lesion produces a worse claw than high ulnar lesion, because high lesion also paralyzes FDP to ring/little, partially equalizing finger IP flexion force)
- Hypothenar wasting (abductor digiti minimi, opponens digiti minimi)
- First dorsal interosseous wasting (visible in the first web space)
- Loss of finger abduction/adduction (all interossei)
- Froment's sign: Patient compensates for paralyzed adductor pollicis by flexing the IP joint of the thumb (flexor pollicis longus, median nerve) when gripping a piece of paper
Sensory loss: Medial 1.5 digits and medial palm; at elbow level the dorsum of the hand is also affected
Special Clinical Syndromes
Pancoast Tumor (Superior Sulcus Tumor)
An apical lung tumor that invades the lower trunk of the brachial plexus from below.
Pancoast's Syndrome:
- Insidious onset of pain in the upper arm / medial forearm
- Sensory disturbance in the medial forearm and hand (C8, T1 distribution)
- Weakness and atrophy of intrinsic hand muscles (lower trunk involvement)
- Ipsilateral Horner's syndrome - ptosis, miosis, enophthalmos, anhidrosis (pressure on the stellate ganglion / sympathetic chain)
- Distension of veins of the face, neck and thorax (superior vena cava compression in advanced disease)
Key point: Pancoast tumor invades the lower trunk (C8-T1). Contrast with radiation-induced plexopathy (which tends to affect the upper trunk, C5-C6, after treatment of breast or lung cancer). - S Das Manual, p. 413; Harrison's 22E, p. 3658
Thoracic Outlet Syndrome (TOS)
Mechanism: Compression of the lower trunk of the brachial plexus (or subclavian vessels) at the thoracic outlet - between the clavicle and first rib, or by a cervical rib.
Key feature - neurogenic TOS:
- Weakness of all intrinsic hand muscles (not restricted to a single nerve distribution)
- Sensory loss mainly in ulnar distribution (C8, T1 sensory fibers travel in the lower trunk, but median sensory fibers to the hand ascend through the middle trunk, which is spared)
- Low-amplitude median and ulnar compound motor action potentials on EMG/NCS
- Cervical rib may be present on imaging but is often asymptomatic
"Thoracic outlet syndrome is an overdiagnosed condition" - Bradley and Daroff's Neurology
Parsonage-Turner Syndrome (Neuralgic Amyotrophy / Immune-Mediated Brachial Plexus Neuropathy)
Hallmark: Acute, severe, burning shoulder pain lasting days to weeks, followed by weakness and sensory loss as the pain subsides.
Mechanism: Immune-mediated (can follow viral illness, surgery, vaccination, or occur idiopathically)
Pattern: Most commonly affects the upper trunk - suprascapular nerve (shoulder weakness), long thoracic nerve (winging of scapula), or axillary nerve. The phrenic and anterior interosseous nerves may also be affected.
Management: Empirical glucocorticoids for severe pain in the acute phase; physiotherapy for recovery. Attacks may recur (hereditary neuralgic amyotrophy - SEPT9 mutation). - Harrison's 22E, p. 3658
Obstetric Brachial Plexus Palsy
| Feature | Erb's Palsy | Klumpke's Palsy |
|---|---|---|
| Roots | C5, C6 | C8, T1 |
| Mechanism | Shoulder dystocia, lateral neck traction | Arm forced over head |
| Frequency | Common (20x more frequent) | Rare |
| Deformity | Waiter's tip / policeman's tip | Claw hand |
| Reflexes lost | Biceps, brachioradialis | Finger jerk |
| Horner's | No | Yes (if T1 root avulsed) |
| Prognosis | >90% resolve by 3 months | Worse, incomplete recovery common |
| Prognostic marker | Biceps function recovery by 2-4 weeks | - |
- Bradley and Daroff's Neurology in Clinical Practice, p. 2870; Miller's Review of Orthopaedics, p. 156
Long Thoracic Nerve Injury (C5, C6, C7 roots)
Causes: Carrying heavy loads on the shoulder, radical mastectomy, spontaneous (Parsonage-Turner)
Deficits: Paralysis of serratus anterior → winging of scapula (vertebral border of the scapula becomes prominent, especially when pushing against a wall)
Clinical test: Ask the patient to push against a wall with both arms extended - the medial scapular border lifts off on the affected side.
Summary Table - Nerve Injuries and Characteristic Signs
| Nerve | Common cause | Motor deficit | Sensory loss | Classic sign |
|---|---|---|---|---|
| Axillary | Shoulder dislocation | Deltoid, teres minor | Lateral arm | "Regimental badge" area loss |
| Musculocutaneous | Coracobrachialis entrapment | Biceps, brachialis | Lateral forearm | Weak supinated elbow flexion |
| Radial (spiral groove) | Midshaft humerus #, Saturday night palsy | Wrist/finger extensors | Dorsum hand | Wrist drop; triceps intact |
| Radial (axillary) | Crutch palsy | + Triceps | Dorsum hand | Wrist drop + triceps weakness |
| Median (wrist) | Carpal tunnel syndrome | Thenar (APB) | Lateral 3.5 digits | Thenar wasting, Tinel's/Phalen's |
| Median (elbow) | Supracondylar fracture | +FPL, FDP index/middle | Lateral palm + digits | Pointing index / Pope's blessing |
| Ulnar (elbow) | Cubital tunnel | Intrinsics, hypothenar | Medial 1.5 digits + dorsum | Claw hand, Froment's sign |
| Long thoracic | Carrying heavy loads | Serratus anterior | None | Winging of scapula |
| Upper trunk (C5-6) | Delivery, fall on shoulder | Deltoid, biceps, spinati | C5/6 dermatomal | Waiter's tip (Erb's palsy) |
| Lower trunk (C8-T1) | Hyperabduction, Pancoast | Intrinsic hand muscles | C8/T1 dermatomal | Claw hand ± Horner's |
Sources:
- Gray's Anatomy for Students, pp. 858, 1170
- Schwartz's Principles of Surgery 11e, p. 1876
- Miller's Review of Orthopaedics 9e, p. 156
- Bradley and Daroff's Neurology in Clinical Practice, pp. 2869-2870
- Harrison's Principles of Internal Medicine 22E, p. 3658
- S Das Manual on Clinical Surgery 13e, pp. 127, 413
This is a shared conversation. Sign in to Orris to start your own chat.