Multiple small vessel ischemic lesions in bilateral centrum semiovale and basal ganglia -Periventricular white matter ischemia . -Cerebral and cerebellar atrophy
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Here is a structured interpretation of this MRI report, grounded in authoritative sources.
MRI Brain Report — Interpretation & Clinical Significance
What the Findings Mean
1. Multiple Small Vessel Ischemic Lesions — Bilateral Centrum Semiovale & Basal Ganglia
These are lacunar infarcts and white matter hyperintensities (WMH) caused by cerebral small vessel disease (SVD). The centrum semiovale and basal ganglia are the territories supplied by deep penetrating arterioles — the vessels most vulnerable to arteriolosclerosis (thickening and narrowing from plasma protein infiltration into vessel walls).
On MRI:
- Appear as T2/FLAIR hyperintensities — patchy or confluent
- Chronic lacunar infarcts show a hyperintense rim with a hypointense cavitated core (3–15 mm)
- Microinfarcts <3 mm may appear as punctate DWI hyperintensities acutely
The primary pathological substrate is focal demyelination and gliosis from gradual narrowing or occlusion of vessels <200 μm in diameter.
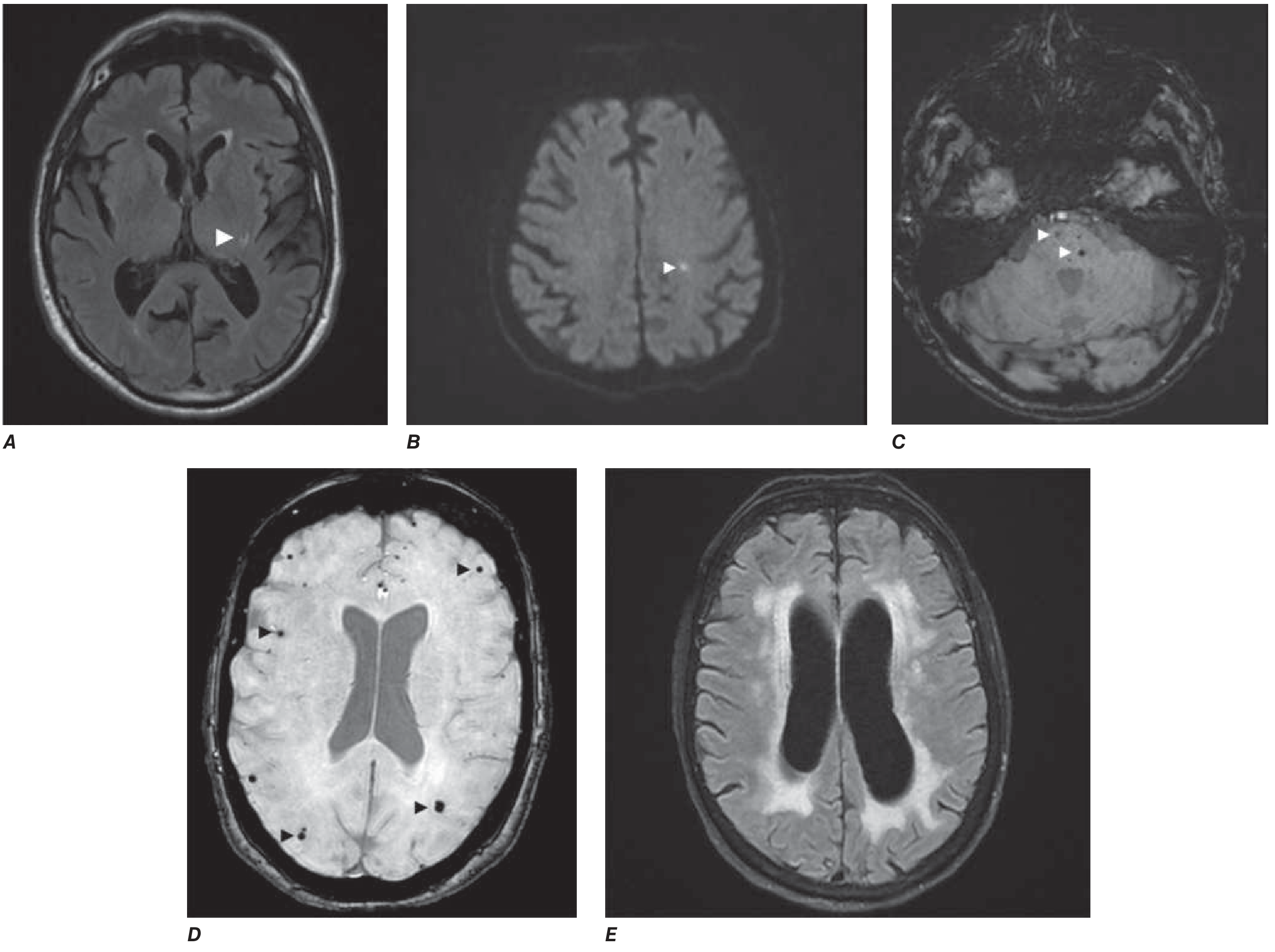
2. Periventricular White Matter Ischemia
Periventricular WMH represent the most severe end of the small vessel disease spectrum. When confluent and extensive, this pattern is termed Binswanger's disease (subcortical arteriosclerotic encephalopathy) — characterized by gradual cognitive deterioration and progressive periventricular/subcortical white matter change with hypoperfusion and hypometabolism.
Even when not yet confluent, periventricular lesions beyond the age-adjusted norm (roughly one WMH per decade of life) are pathological and carry clinical significance.
3. Cerebral & Cerebellar Atrophy
Generalized atrophy co-existing with ischemic white matter disease reflects:
- Wallerian degeneration — downstream axonal loss from ischemic injury to white matter tracts
- Neuronal loss in regions deprived of functional connectivity
- Higher lesion load is consistently associated with greater degree of central (brain volume) atrophy
- Cerebellar atrophy may reflect crossed cerebellar diaschisis from supratentorial lesions, or independent age/vascular effects
Risk Factors to Evaluate
| Risk Factor | Relevance |
|---|---|
| Hypertension | #1 driver of arteriolosclerosis and deep SVD |
| Diabetes mellitus | Accelerates microvascular disease |
| Hyperlipidemia / dyslipidemia | Increases WMH burden |
| Smoking | Independent risk factor for WMH |
| Age | Incidence rises sharply after age 40 |
Clinical Consequences
Depending on lesion burden and location, the patient may have or be at risk for:
| Domain | Impact |
|---|---|
| Cognition | Executive dysfunction, processing speed slowing, memory impairment → Vascular Cognitive Impairment & Dementia (VCID) |
| Gait | Small-stepped, apraxic gait; balance difficulty |
| Bladder | Urgency incontinence (leukoaraiosis disrupts pontine–frontal micturition pathways) |
| Mood | Depression, emotional lability |
| Stroke risk | Elevated risk of future symptomatic lacunar or cortical stroke |
Management Priorities
- Aggressive vascular risk factor control — blood pressure is the most modifiable target (target <130/80 mmHg)
- Diabetes and dyslipidemia management
- Antiplatelet therapy — if symptomatic lacunar infarcts are present
- Cognitive assessment — baseline neuropsychological evaluation; monitor for VCID progression
- Lifestyle — smoking cessation, physical activity, Mediterranean diet
- Fall prevention — given gait and balance risk
Sources: Harrison's Principles of Internal Medicine 22E, Ch. 444 (VCID & Small Vessel Disease) | Bradley and Daroff's Neurology in Clinical Practice, Ch. 40 (Cerebrovascular Occlusive Disease) | Textbook of Family Medicine 9E
This is a shared conversation. Sign in to Orris to start your own chat.