Multiple small vessel ischemic lesions in bilateral centrum semiovale and basal ganglia -Periventricular white matter ischemia . -Cerebral and cerebellar atrophy
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive interpretation of this MRI report:
MRI Brain Findings: Interpretation & Clinical Significance
What the Report Describes
The three findings together paint a classic picture of cerebral small vessel disease (SVD) — a pattern of age- and vascular risk factor-related microvascular injury to the brain's deep structures.
1. Multiple Small Vessel Ischemic Lesions — Bilateral Centrum Semiovale & Basal Ganglia
These are lacunar infarcts and/or microinfarcts resulting from occlusion of small deep-penetrating arteries (diameter < 200 µm), specifically the lenticulostriate arteries supplying the basal ganglia and medullary perforators supplying the centrum semiovale.
Pathophysiology:
- The primary mechanism is arteriolosclerosis — thickening and hyalinization of arteriolar walls from infiltration of plasma proteins, driven by chronic hypertension and diabetes
- This causes progressive narrowing → in situ thrombosis → focal infarction
- Lesions in the basal ganglia (caudate, putamen, thalamus) and centrum semiovale (subcortical white matter core) are characteristic locations
On MRI:
- Chronic lacunes: FLAIR hyperintense rim with hypointense cavitated core, typically 3–15 mm (Panel A in image above)
- Acute microinfarcts: punctate DWI hyperintensities (Panel B)
- Bilateral distribution indicates systemic vascular risk factors rather than focal embolic disease
"Lacunar ischemic strokes constitute 20–25% of all strokes and are typically seen in patients with hypertension and diabetes... Most common locations include basal ganglia, internal capsule, and thalamus." — Bradley and Daroff's Neurology in Clinical Practice
2. Periventricular White Matter Ischemia (Leukoaraiosis)
This refers to T2/FLAIR hyperintensities in the white matter adjacent to the lateral ventricles — also called leukoaraiosis or white matter hyperintensities (WMH).
Pathophysiology:
- Same underlying arteriolosclerotic process affecting end-arterioles of the deep white matter
- Results in focal demyelination, axonal loss, and gliosis
- Lesions are chronic, have diffuse "cotton-wool" borders, no mass effect, no edema
- Distribution: periventricular zone → deep white matter → can become confluent (Panel E in image above)
Grading severity:
- Mild: scattered punctate lesions
- Moderate: partial confluence
- Severe/confluent (Binswanger's disease): "gradual cognitive deterioration and notable white matter changes of small-vessel ischemic disease" with hypoperfusion and hypometabolism on functional imaging
Risk factors (per multiple sources):
| Risk Factor | Significance |
|---|---|
| Hypertension | Strongest modifiable risk factor |
| Diabetes mellitus | Independent risk factor |
| Hypercholesterolemia | Contributing factor |
| Age | Universal; incidence rises sharply after age 40 |
| Smoking | Additional vascular burden |
"While age by itself can cause such changes... there are several other risk factors that can make them more numerous. These include hypertension, diabetes, hypercholesterolemia, and smoking." — Bradley and Daroff's Neurology in Clinical Practice
3. Cerebral and Cerebellar Atrophy
Atrophy in this context is not simply age-related — it reflects volume loss secondary to ongoing small vessel disease, with:
- Loss of white matter from ischemic injury → secondary cortical thinning
- Associated with higher lesion burden
- Cerebellar atrophy in this context may reflect disconnection from supratentorial networks or direct small vessel involvement of cerebellar penetrators
MRI Markers of Cerebral Small Vessel Disease (Harrison's 2025)
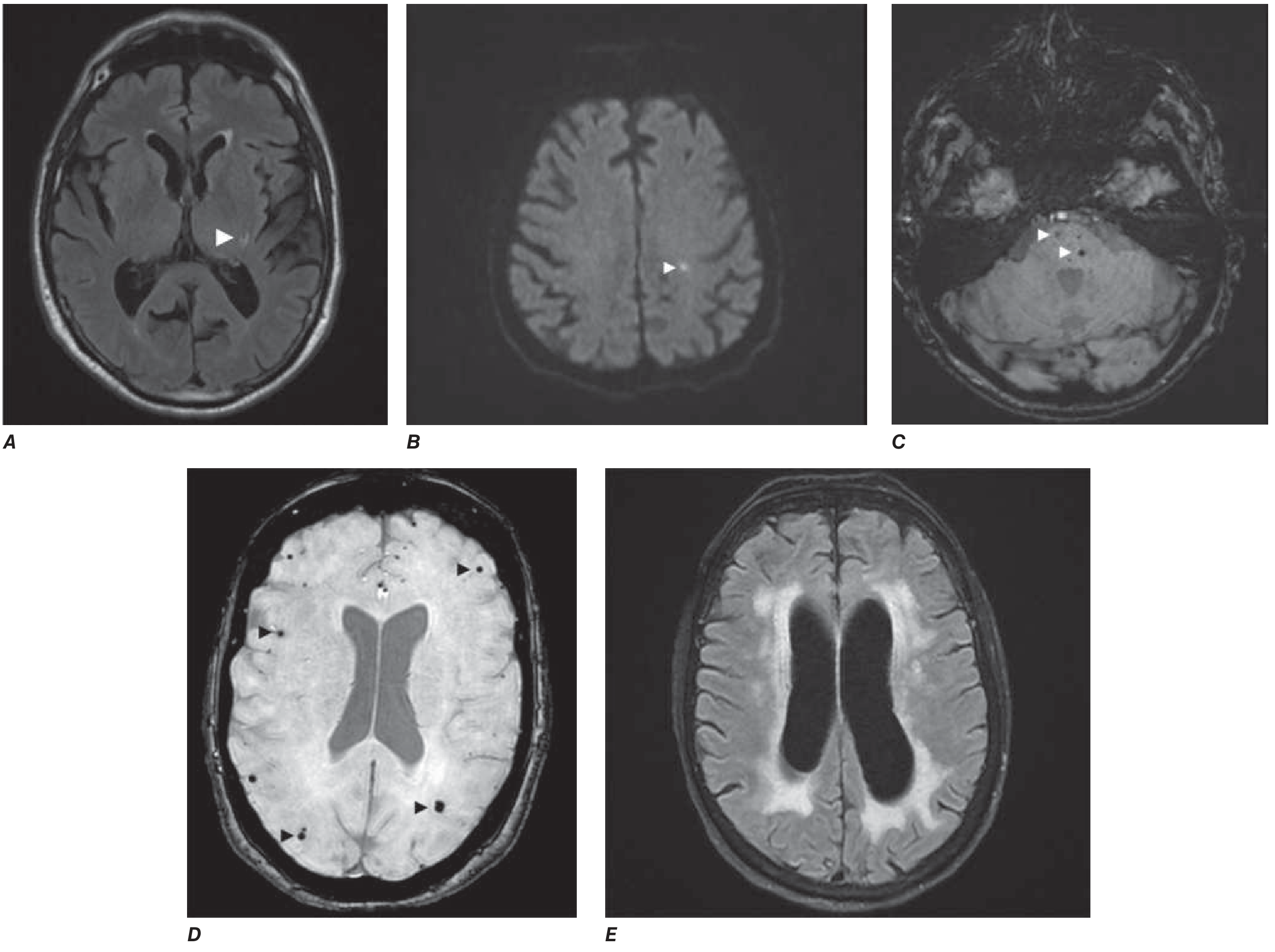
A = Lacunar infarct (FLAIR, left thalamus) | B = Acute microinfarct (DWI, centrum semiovale) | C = Deep microbleeds (T2, pons) | D = Lobar microbleeds | E = Confluent white matter hyperintensities (FLAIR)*
Clinical Implications
| Domain | Risk/Consequence |
|---|---|
| Cognitive function | Executive dysfunction, psychomotor slowing; thalamic/putaminal lacunes carry worse cognitive prognosis than capsular ones |
| Dementia | 47% of small subcortical stroke patients have MCI; recurrent strokes → 33% develop dementia |
| Gait | White matter burden independently associated with gait decline and falls |
| Depression | WMH associated with incident late-life depression |
| Stroke risk | Presence of these lesions = biomarker for more extensive cerebrovascular disease; silent infarcts double dementia risk |
Management Priorities
Based on the underlying pathophysiology, management centers on aggressive vascular risk factor control:
- Blood pressure control — the single most important intervention; target < 130/80 mmHg
- Glycemic control — if diabetic
- Statin therapy — for hyperlipidemia
- Antiplatelet therapy — aspirin or clopidogrel if there has been symptomatic lacunar stroke
- Lifestyle modification — smoking cessation, regular aerobic exercise
- Cognitive surveillance — periodic neuropsychological assessment
- Screen for atrial fibrillation — rule out cardioembolic contribution (bilateral lesions can occasionally be embolic)
"The mainstay of treatment includes control of hypertension, diabetes, hyperlipidemia, and atrial fibrillation." — Textbook of Family Medicine, 9th Edition
Sources: Harrison's Principles of Internal Medicine 22E (2025) | Bradley and Daroff's Neurology in Clinical Practice | Textbook of Family Medicine 9E
This is a shared conversation. Sign in to Orris to start your own chat.