MetforminMetformin (oral) High No Neutral (potential for modest loss) Potential benefit Neutral Neutral Contraindicated with Neutral eGFR <30 mL/min/1.73 m² SGLT2 inhibitors (oral) Intermediate to high No Loss (intermediate) Benefit: Benefit: canagliflozin, empagliflozin canagliflozin, dapagliflozin, empagliflozin, Benefit: canagliflozin, empagliflozin, dapagliflozin ertugliflozin See labels of individ- Unknown ual agents for dosage considerations for kidney function Glucose-lowering effect is minimal at eGFR <45 ml/min/ 1.73 m² and lower; continue or start for cardiovascular and kidney benefit if eGFR >20 ml/min/1.73 m². May continue until dialysis or transplantation Clinical considerations and adverse effects Gl side effects: mitigate with slow dose titration, extended-release formula- tions, and administration with food Potential for vitamin B12 deficiency: monitor and replete as appropriate DKA risk in individuals with insulin deficiency (rare in 12D): discontinue, evaluate, and treat promptly if sus- pected; be aware of predis-posing risk factors and clini cal presentations (including euglycemic DKA); mitigate risk with sick-day planning discontinue before sched- uled surgery (e.g., 3-4 days), during critical illness, fasting or during prolonged fasting Genital mycotic infections: mitigate risk with genital hygiene and avoid use in high-risk individuals Urosepsis and pyelonephri tis: evaluate individuals for signs and symptoms of urinary tract infections and treat promptly Necrotizing fascitis in the perineum (Fournier gangrene): rare; prompt treatment if suspected Intravascular volume deple tion: attention to volume status and blood pressure, particularly when ill or fast-ing; adjust other volume- contracting agents as appli-cable; monitor kidney func tion upon initiation Continued on. Give me dosage, how many times a day , titration, maximum dosages, how long and indication and contraindications of Metformin
metformin dosing type 2 diabetes guidelines
metformin dosage titration maximum dose indication contraindications 2025 ADA guidelines
https://www.ncbi.nlm.nih.gov/books/NBK518983
Metformin - Complete Clinical Reference
Indications
- First-line pharmacotherapy for Type 2 Diabetes Mellitus (T2DM) - recommended as the starting agent for most patients without comorbidities driving another agent choice (per 2025 ADA Standards)
- Add-on therapy alongside SGLT2 inhibitors, GLP-1 RAs, and insulin when initiating insulin (continue metformin)
- Off-label / additional uses: Polycystic ovary syndrome (PCOS) - to restore ovulation; prevention of T2DM in high-risk prediabetes; antipsychotic-induced weight gain
Dosage, Frequency & Titration
Immediate-Release (IR) - Adults
| Phase | Dose | Frequency |
|---|---|---|
| Starting dose | 500 mg OR 850 mg | Once or twice daily with meals |
| Titration | Increase by 500 mg/week OR 850 mg every 2 weeks | As tolerated |
| Maintenance | 850-1000 mg | Twice daily (with meals) |
| Maximum dose | 2550 mg/day | Divided into 2-3 doses with meals |
Significant glycemic responses are typically not seen below 1500 mg/day; doses above 2000 mg add little extra efficacy and worsen tolerability.
Extended-Release (ER) - Adults
| Phase | Dose | Frequency |
|---|---|---|
| Starting dose | 500-1000 mg | Once daily with the evening meal |
| Titration | Increase by 500 mg/week | As tolerated |
| Maintenance | 1000-2000 mg | Once daily (evening meal) |
| Maximum dose | 2000 mg/day | Once daily; may split to 1000 mg twice daily if needed |
Switching from IR to ER: use the same total daily dose (up to 2000 mg), given once daily.
Pediatric Dosing (ages 10+)
| Phase | Dose |
|---|---|
| Starting dose | 500 mg twice daily with meals |
| Titration | 500 mg/week increments |
| Maximum dose | 2000 mg/day |
Duration of Use
Titration Timeline Summary
- Week 1: 500 mg once or twice daily
- Week 2: 500 mg twice daily (if starting once daily)
- Week 3-4: 1000 mg in the morning + 500 mg in the evening
- Week 6-8: 1000 mg twice daily (target maintenance for most patients)
- Slow titration over 4-8 weeks significantly reduces GI side effects.
Mechanism of Action
Contraindications
| Contraindication | Details |
|---|---|
| eGFR < 30 mL/min/1.73 m² | Absolute contraindication - drug is renally eliminated unchanged; accumulation causes lactic acidosis |
| eGFR 30-45 | Not recommended to initiate; use caution if already on it; some guidelines allow 500 mg daily with close monitoring |
| Metabolic acidosis / Lactic acidosis | Any active form of acidosis |
| Hepatic insufficiency | Impaired lactate clearance raises lactic acidosis risk |
| Hypersensitivity to metformin | Any documented allergic reaction |
| Severe hypoxemia | e.g., respiratory failure, severe CHF, sepsis |
| Alcohol abuse | Potentiates lactic acidosis risk |
| Iodinated contrast administration | Withhold metformin for 48 hours after IV contrast in patients with renal risk |
| Surgical procedures | Discontinue 3-4 days before scheduled surgery; hold during critical illness or prolonged fasting |
| Pregnancy (T2DM/GDM) | Not recommended as first-line per ADA 2025 - lifestyle + insulin preferred; if on metformin for PCOS, stop after 1st trimester |
| SCr ≥ 1.5 mg/dL (men) or ≥ 1.4 mg/dL (women) | Traditional creatinine-based cutoff (older labeling) |
Key Adverse Effects
| Effect | Notes |
|---|---|
| GI symptoms (nausea, diarrhea, abdominal cramping, metallic taste) | Most common; mitigate with slow titration, ER formulation, and taking with food |
| Lactic acidosis | Rare but serious; almost exclusively in renal insufficiency |
| Vitamin B12 deficiency | Long-term use reduces B12 absorption; monitor levels and replete as needed |
| No hypoglycemia risk | As monotherapy; does not raise insulin levels |
Renal Dose Adjustments
| eGFR (mL/min/1.73 m²) | Action |
|---|---|
| > 60 | No adjustment; monitor annually |
| 45-60 | No adjustment; monitor every 3-6 months |
| 30-45 | Do not initiate; if already on drug, reassess risk vs. benefit |
| < 30 | Contraindicated - discontinue |
Key Clinical Pearls (2025 ADA)
- Metformin fits as an add-on to SGLT2-i or GLP-1 RA when those are selected first for CV/renal benefit, and as the starting agent when no comorbidities drive another choice first.
- Continue metformin when initiating insulin; stop sulfonylureas and DPP-4 inhibitors.
- Extended-release reduces GI side effects substantially and is preferred for patients who cannot tolerate IR.
From Ada 2026 guidelines
ADA 2026 Standards of Medical Care Diabetes metformin dosage guidelines
ADA 2026 pharmacologic approaches glycemic treatment metformin section 9
https://sentucuman.com.ar/docs/standards-of-care-2026.pdf
ADA 2026 Standards Care metformin table 9.2 dosing contraindication eGFR site:diabetesjournals.org OR site:care.diabetesjournals.org
https://sentucuman.com.ar/docs/standards-of-care-2026.pdf
Metformin - ADA 2026 Standards of Care
Indications (ADA 2026)
| Setting | Role |
|---|---|
| Type 2 Diabetes (no comorbidities) | First-line / starting agent |
| T2DM with ASCVD, HF, or CKD | Add-on to SGLT2-i or GLP-1 RA (which are now chosen first for organ-protective benefit) |
| Prediabetes prevention (Rec. 3.7) | Consider in high-risk adults, especially age 25-59, BMI ≥35 kg/m², FPG ≥110 mg/dL, A1C ≥6.0%, or prior GDM - Evidence Level A |
| PI3Kα inhibitor-induced hyperglycemia (Rec. 3.8 - NEW 2026) | Consider to prevent hyperglycemia in those on alpelisib or inavolisib - Evidence Level B |
| High-dose glucocorticoid-induced hyperglycemia (Rec. 3.9 - NEW 2026) | Consider to prevent/treat glucocorticoid-induced hyperglycemia - Evidence Level B |
| mTOR/PI3K inhibitor hyperglycemia (Rec. 9.35a - NEW 2026) | First-line treatment |
| Stable Heart Failure | Continue if eGFR >30 mL/min/1.73 m²; avoid in unstable HF or patients hospitalized for HF |
| Continue when insulin is initiated | Do not stop metformin when starting insulin |
Dosage, Frequency & Titration
Immediate-Release (IR)
| Phase | Dose | Frequency |
|---|---|---|
| Initial | 500 mg | Once or twice daily with meals |
| Titration | Increase by 500 mg every week (or 850 mg every 2 weeks) | As tolerated to minimize GI side effects |
| Maintenance | 1000-1500 mg | Twice daily with meals |
| Maximum | 2550 mg/day | 2-3 divided doses with meals |
Extended-Release (ER)
| Phase | Dose | Frequency |
|---|---|---|
| Initial | 500-1000 mg | Once daily with evening meal |
| Titration | Increase by 500 mg weekly | As tolerated |
| Maximum | 2000 mg/day | Once daily; may split to 1000 mg twice daily if glycemic control insufficient |
ADA 2026 guidance: Meaningful glycemic effect typically requires ≥1500 mg/day. Doses >2000 mg provide minimal additional benefit and worse GI tolerability.
Duration
Renal Dose Adjustments (ADA 2026)
| eGFR (mL/min/1.73 m²) | Action |
|---|---|
| >60 | No adjustment needed; monitor annually |
| 45-60 | No dose adjustment; monitor every 3-6 months |
| 30-45 | Do NOT initiate; reassess risk/benefit if already on it |
| <30 | Contraindicated - discontinue |
| Dialysis / transplant | Contraindicated |
ADA 2026 also notes: glucose-lowering effect is minimal at eGFR <45 mL/min/1.73 m²; the drug may be continued for cardiovascular/kidney benefit in SGLT2-i context if eGFR >20 (this applies to SGLT2-i, not metformin).
Contraindications (ADA 2026)
| Contraindication | Notes |
|---|---|
| eGFR <30 mL/min/1.73 m² | Primary absolute contraindication |
| Metabolic/lactic acidosis | Any active form |
| Hepatic insufficiency | Impairs lactate clearance |
| Severe hypoxemia | Respiratory failure, severe decompensated HF, sepsis |
| Unstable or hospitalized heart failure | Avoid; may continue in stable HF if eGFR >30 |
| Iodinated IV contrast (eGFR 30-60) | Temporarily discontinue at time of procedure; restart 48 hours after if renal function stable |
| Surgery / critical illness / prolonged fasting | Discontinue 3-4 days before elective surgery; hold during critical illness |
| Alcohol abuse | Increases lactic acidosis risk |
| Hypersensitivity to metformin | Any prior allergic reaction |
| Pregnancy (T2DM/GDM) | Not recommended first-line per ADA 2026 - lifestyle + insulin preferred; if on metformin for PCOS, stop after 1st trimester |
Key Adverse Effects & Monitoring (ADA 2026)
| Issue | ADA 2026 Guidance |
|---|---|
| GI side effects (nausea, diarrhea, abdominal cramping, metallic taste) | Mitigate with slow titration, ER formulation, taking with food |
| Vitamin B12 deficiency | Monitor periodically in chronic users, especially if dose ≥1500 mg/day, duration >4-5 years, or risk factors present (anemia, neuropathy, CKD, vegan diet). ADA 2026 annual labs table flags: "Vitamin B12 if taking metformin >5 years" |
| Hypoglycemia | Not associated as monotherapy - does not stimulate insulin secretion |
| Lactic acidosis | Rare; almost exclusively in patients with renal impairment - avoided by adherence to eGFR thresholds |
New 2026-Specific Updates on Metformin
- Rec. 3.8 (NEW): Use metformin to prevent hyperglycemia in patients on PI3Kα inhibitors (alpelisib, inavolisib) for cancer treatment.
- Rec. 3.9 (NEW): Use metformin to prevent glucocorticoid-induced hyperglycemia in high-risk patients on high-dose steroids.
- Rec. 9.35a (NEW): Metformin is first-line for hyperglycemia caused by mTOR or PI3K inhibitors.
- Figure 9.4 updated to show GIP/GLP-1 RAs added for symptomatic HFpEF, MASLD/MASH, and obesity - metformin remains add-on in these contexts.
- When insulin is initiated, continue metformin (and SGLT2-i, GLP-1 RA); stop sulfonylureas, meglitinides, and DPP-4 inhibitors.
Create me a flowchart for the Metformin which recently you gave
A clean, professional medical flowchart for Metformin (ADA 2026 Guidelines) with the following structure and content: Title at top: "METFORMIN - ADA 2026 Clinical Flowchart" FLOW: Box 1 (START - green): "Patient with Type 2 Diabetes or Indication for Metformin" Arrow down to Diamond 1 (yellow decision): "Any Contraindication Present?" From Diamond 1 - YES arrow right to Red Box: "CONTRAINDICATED - Do NOT Use Metformin" with list: - eGFR <30 mL/min/1.73 m² - Metabolic/lactic acidosis - Hepatic insufficiency - Severe hypoxemia - Hypersensitivity to metformin - Alcohol abuse - Unstable/hospitalized Heart Failure - Pregnancy (T2DM/GDM) From Diamond 1 - NO arrow down to Diamond 2 (yellow): "Check eGFR" From Diamond 2 - three arrows: - Arrow LEFT labeled "eGFR <30" → Red box: "STOP / Do Not Start" - Arrow MIDDLE labeled "eGFR 30-45" → Orange box: "Do NOT initiate. If already on it, reassess risk/benefit. Monitor every 3 months" - Arrow RIGHT labeled "eGFR 45-60" → Yellow box: "No dose adjustment. Monitor every 3-6 months" - Arrow DOWN labeled "eGFR >60" → Green box: "No adjustment. Monitor annually" All eGFR >45 paths merge down to Blue Box: "INITIATE METFORMIN" Two columns inside: LEFT - "Immediate-Release (IR): Start: 500 mg once or twice daily with meals | Titrate: +500 mg/week as tolerated | Maintenance: 1000-1500 mg twice daily | MAX: 2550 mg/day (2-3 divided doses)" RIGHT - "Extended-Release (ER): Start: 500-1000 mg once daily with evening meal | Titrate: +500 mg/week as tolerated | Maintenance: 1000-2000 mg once daily | MAX: 2000 mg/day" Arrow down to Purple Box: "MONITORING" - Vitamin B12: check if dose ≥1500 mg/day or >4-5 years use - eGFR: annually (more often if CKD) - GI side effects: mitigate with slow titration, ER form, food - No hypoglycemia risk as monotherapy Arrow down to Orange Box: "SPECIAL SITUATIONS - Hold/Discontinue" - Surgery: stop 3-4 days before - IV contrast (eGFR 30-60): hold at time of procedure, restart 48h after - Critical illness / prolonged fasting: hold - Unstable HF or hospitalization: hold Arrow down to Dark Blue Box: "CONTINUE METFORMIN WHEN…" - Starting insulin therapy - Adding SGLT2 inhibitors or GLP-1 RAs - Stable Heart Failure (if eGFR >30) Small box at bottom right labeled "NEW ADA 2026" in red: - Rec 3.8: Use to prevent PI3Kα inhibitor hyperglycemia - Rec 3.9: Use to prevent glucocorticoid-induced hyperglycemia - Rec 9.35a: First-line for mTOR/PI3K inhibitor hyperglycemia Use a white background, color-coded boxes (green=go, red=stop, yellow=caution, blue=action, purple=monitoring), clear arrows with labels, professional medical style, readable font sizes. Make it well-spaced and easy to follow.
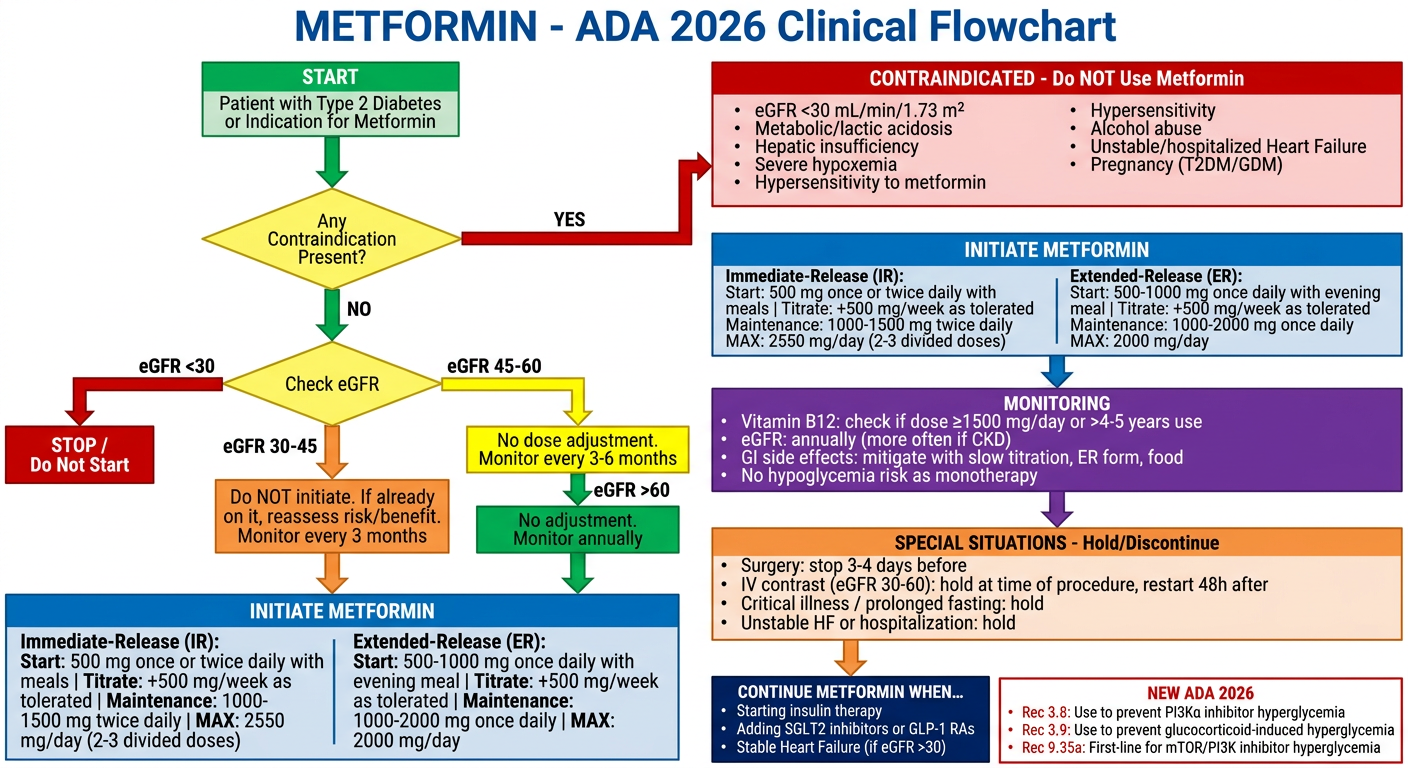
- Contraindication screening before initiating
- eGFR-based decision pathway (the key renal cutoffs: <30, 30-45, 45-60, >60)
- Dosing initiation and titration for both IR and ER formulations with maximum doses
- Monitoring requirements (B12, eGFR, GI effects)
- When to hold/discontinue (surgery, contrast, critical illness)
- When to continue (with insulin, SGLT2-i, GLP-1 RA, stable HF)
- New 2026 recommendations (PI3Kα inhibitors, glucocorticoids, mTOR/PI3K inhibitors)
Give me dosage, how many times a day , titration, maximum dosages, how long and indication and contraindications from Ada 2026 guidelines
Give me dosage, how many times a day , titration, maximum dosages, how long and indication and contraindications from Ada 2026 guidelines for SGLT2 AND make me a flowchart image like before
ADA 2026 Standards Care SGLT2 inhibitors dosage titration indication contraindication table 9.2
SGLT2 inhibitors canagliflozin dapagliflozin empagliflozin ertugliflozin dosage ADA 2026 eGFR contraindications
http://saigaiin.sakura.ne.jp/sblo_files/saigaiin/image/DM20E…
https://www.ncbi.nlm.nih.gov/books/NBK576405
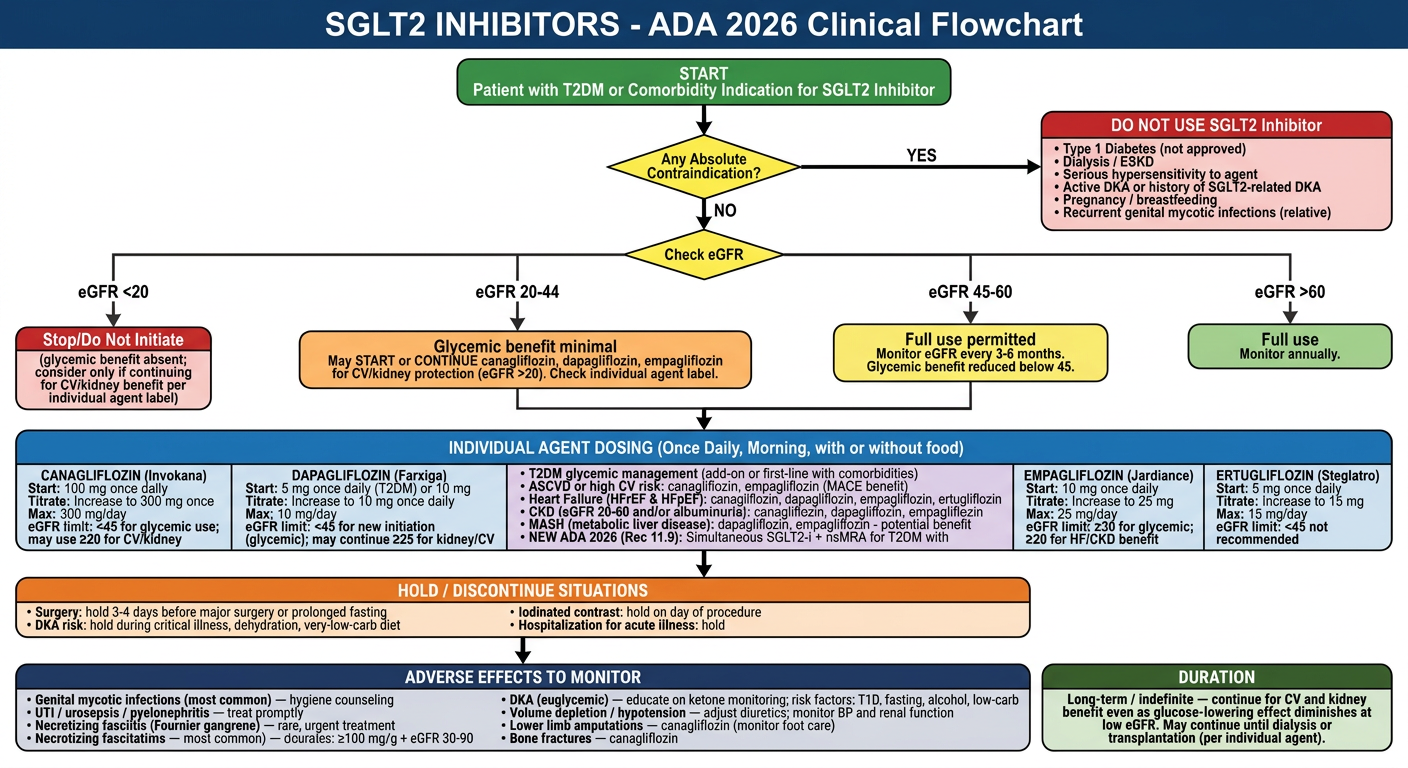
A clean, professional medical flowchart titled "SGLT2 INHIBITORS - ADA 2026 Clinical Flowchart" on a white background. Color-coded boxes with clear arrows. Professional medical style. Well-spaced and easy to follow. Layout from top to bottom: TOP - GREEN BOX (START): "Patient with T2DM or Comorbidity Indication for SGLT2 Inhibitor" Arrow down to YELLOW DIAMOND: "Any Absolute Contraindication?" YES arrow right → RED BOX "DO NOT USE SGLT2 Inhibitor: • Type 1 Diabetes (not approved) • Dialysis / ESKD • Serious hypersensitivity to agent • Active DKA or history of SGLT2-related DKA • Pregnancy / breastfeeding • Recurrent genital mycotic infections (relative)" NO arrow down → YELLOW DIAMOND: "Check eGFR" From eGFR diamond, 4 paths: LEFT path: "eGFR <20" → RED BOX "Stop/Do Not Initiate (glycemic benefit absent; consider only if continuing for CV/kidney benefit per individual agent label)" CENTER-LEFT: "eGFR 20-44" → ORANGE BOX "Glycemic benefit minimal. May START or CONTINUE canagliflozin, dapagliflozin, empagliflozin for CV/kidney protection (eGFR >20). Check individual agent label." CENTER-RIGHT: "eGFR 45-60" → YELLOW BOX "Full use permitted. Monitor eGFR every 3-6 months. Glycemic benefit reduced below 45." RIGHT path: "eGFR >60" → GREEN BOX "Full use. Monitor annually." All paths eGFR >20 merge → BLUE BOX "INDIVIDUAL AGENT DOSING (Once Daily, Morning, with or without food)" 4 columns: Column 1 - CANAGLIFLOZIN (Invokana): Start: 100 mg once daily | Titrate: Increase to 300 mg once daily if needed | Max: 300 mg/day | eGFR limit: <45 for glycemic use; may use ≥20 for CV/kidney Column 2 - DAPAGLIFLOZIN (Farxiga): Start: 5 mg once daily (T2DM) or 10 mg once daily (HF/CKD) | Titrate: Increase to 10 mg once daily | Max: 10 mg/day | eGFR limit: <45 for new initiation (glycemic); may continue ≥25 for kidney/CV Column 3 - EMPAGLIFLOZIN (Jardiance): Start: 10 mg once daily | Titrate: Increase to 25 mg once daily | Max: 25 mg/day | eGFR limit: ≥30 for glycemic; ≥20 for HF/CKD benefit Column 4 - ERTUGLIFLOZIN (Steglatro): Start: 5 mg once daily | Titrate: Increase to 15 mg once daily | Max: 15 mg/day | eGFR limit: <45 not recommended Arrow down → PURPLE BOX "INDICATIONS (ADA 2026)" • T2DM glycemic management (add-on or first-line with comorbidities) • ASCVD or high CV risk: canagliflozin, empagliflozin (MACE benefit) • Heart Failure (HFrEF & HFpEF): canagliflozin, dapagliflozin, empagliflozin, ertugliflozin • CKD (eGFR 20-60 and/or albuminuria): canagliflozin, dapagliflozin, empagliflozin • MASH (metabolic liver disease): dapagliflozin, empagliflozin - potential benefit • NEW ADA 2026 (Rec 11.9): Simultaneous SGLT2-i + nsMRA for T2DM with uACR ≥100 mg/g + eGFR 30-90 Arrow down → ORANGE BOX "HOLD / DISCONTINUE SITUATIONS" • Surgery: hold 3-4 days before major surgery or prolonged fasting • DKA risk: hold during critical illness, dehydration, very-low-carb diet • Iodinated contrast: hold on day of procedure • Hospitalization for acute illness: hold Arrow down → DARK BLUE BOX "ADVERSE EFFECTS TO MONITOR" • Genital mycotic infections (most common) — hygiene counseling • UTI / urosepsis / pyelonephritis — treat promptly • Necrotizing fasciitis (Fournier gangrene) — rare, urgent treatment • DKA (euglycemic) — educate on ketone monitoring; risk factors: T1D, fasting, alcohol, low-carb • Volume depletion / hypotension — adjust diuretics; monitor BP and renal function • Lower limb amputations — canagliflozin (monitor foot care) • Bone fractures — canagliflozin Small box bottom right labeled "DURATION" in dark green: "Long-term / indefinite — continue for CV and kidney benefit even as glucose-lowering effect diminishes at low eGFR. May continue until dialysis or transplantation (per individual agent)." Use white background, color-coded boxes, clear directional arrows with labels, readable fonts, professional clean medical layout.
SGLT2 Inhibitors - ADA 2026 Standards of Care
Indications (ADA 2026)
| Clinical Setting | Agents with Proven Benefit |
|---|---|
| T2DM - glycemic management (add-on or first-line with comorbidities) | All agents |
| ASCVD / High CV risk - MACE reduction | Canagliflozin, Empagliflozin |
| Heart Failure (HFrEF & HFpEF) | Canagliflozin, Dapagliflozin, Empagliflozin, Ertugliflozin |
| CKD (eGFR 20-60 and/or albuminuria) - slow CKD progression | Canagliflozin, Dapagliflozin, Empagliflozin |
| MASH/MASLD (metabolic liver disease) | Dapagliflozin, Empagliflozin (potential benefit) |
| NEW 2026 (Rec 11.9): T2DM + uACR ≥100 mg/g + eGFR 30-90 on RAS blocker | Simultaneous SGLT2-i + nsMRA initiation now recommended |
ADA 2026 key position: In T2DM with ASCVD, HF, or CKD - SGLT2-i should be chosen independent of A1C for organ protection.
Individual Agent Dosing - All Once Daily (Morning, With or Without Food)
Canagliflozin (Invokana)
| Phase | Dose | Frequency |
|---|---|---|
| Starting | 100 mg | Once daily before first meal |
| Titration | Increase to 300 mg if tolerated and additional control needed | Once daily |
| Maximum | 300 mg/day | Once daily |
| eGFR limit | <45: do not start for glycemic use; ≥20: may start/continue for CV/kidney benefit | - |
Dapagliflozin (Farxiga)
| Phase | Dose | Frequency |
|---|---|---|
| Starting (T2DM glycemic) | 5 mg | Once daily (morning) |
| Starting (HF or CKD indication) | 10 mg | Once daily (morning) |
| Titration | Increase to 10 mg if additional glycemic control needed | Once daily |
| Maximum | 10 mg/day | Once daily |
| eGFR limit | <45: do not initiate for glycemic use; may continue if eGFR drops to ≥25 for kidney/CV benefit | - |
Empagliflozin (Jardiance)
| Phase | Dose | Frequency |
|---|---|---|
| Starting | 10 mg | Once daily (morning) |
| Titration | Increase to 25 mg if additional glycemic control needed | Once daily |
| Maximum | 25 mg/day | Once daily |
| eGFR limit | <30: insufficient data for T2DM+CVD; <20: insufficient data for HF; ≥20 for CKD/CV benefit | - |
Ertugliflozin (Steglatro)
| Phase | Dose | Frequency |
|---|---|---|
| Starting | 5 mg | Once daily (morning) |
| Titration | Increase to 15 mg if additional glycemic control needed | Once daily |
| Maximum | 15 mg/day | Once daily |
| eGFR limit | <45: do not initiate; no established CV/kidney outcomes trial evidence at low eGFR | - |
eGFR Decision Guide (ADA 2026)
| eGFR (mL/min/1.73 m²) | Action |
|---|---|
| >60 | Full use; all agents; monitor annually |
| 45-60 | Full use; glycemic benefit starts declining; monitor every 3-6 months |
| 20-44 | Glycemic benefit minimal - but continue or start for CV/kidney protection (cana, dapa, empa); check individual agent label |
| <20 | Do not initiate; limited evidence; consider only if already on therapy and continuing for non-glycemic benefit per label |
| Dialysis/ESKD | Contraindicated |
Contraindications (ADA 2026)
| Contraindication | Notes |
|---|---|
| Type 1 Diabetes | Not FDA-approved; high DKA risk (~4% incidence; 5-17x higher than T1DM without SGLT2-i) |
| Active DKA or history of SGLT2-related DKA | Do not restart |
| Dialysis / ESKD | Contraindicated for all agents |
| Serious hypersensitivity to specific agent | Avoid that agent and related compounds |
| Pregnancy / breastfeeding | Avoid |
| Severe volume depletion | Correct before initiating |
When to Hold / Discontinue (ADA 2026)
| Situation | Action |
|---|---|
| Major surgery / prolonged fasting | Hold 3-4 days before |
| Critical illness, dehydration, severe vomiting | Hold immediately (sick-day rules) |
| Iodinated contrast procedure | Hold on day of procedure |
| Hospitalization for acute illness | Hold during admission |
| Very-low-carbohydrate diet / prolonged fast | High DKA risk - hold or avoid |
Key Adverse Effects to Monitor
| Effect | Management |
|---|---|
| Genital mycotic infections (most common) | Hygiene counseling; avoid in high-risk individuals |
| UTI / urosepsis / pyelonephritis | Evaluate and treat promptly |
| Necrotizing fasciitis - Fournier gangrene | Rare; urgent surgical + antibiotic treatment |
| Euglycemic DKA | Educate on ketone monitoring; risk factors: fasting, alcohol, low-carb, insulin deficiency. Up to 71% present with glucose ≤250 mg/dL |
| Volume depletion / hypotension | Adjust diuretics; monitor BP and renal function on initiation |
| Lower limb amputations | Canagliflozin - monitor foot care closely |
| Bone fractures | Canagliflozin - monitor in osteoporosis risk patients |
| Transient eGFR dip on initiation | Expected hemodynamic effect; do not stop unless severe |
Duration
GLP-1 RAS (SQ; High to very high No Loss (intermediate to very high) Benefit: dulaglutide, semaglutide also available in oral formulation) CV effects Kidney effects Progression of Effect on MACE iraglutide, semaglutide (SQ and oral) Effect on HF CKD Dosing/use considerations MASH effects Benefit: Benefit for See labels of individ Benefit: semaglutide (SQ) kidney end ual agents for dosage points in CVOTs, driven considerations for semaglutide (SQ) kidney function No dose adjustment Neutral: exenatide once weekly, lixisenatide Dual GIP and Very high GLP-1 RA (SQ) No Loss (very high) Under investigation Benefit: tirzepatide by albuminuria outcomes: dulaglutide, liraglutide, semaglutide (SQ) Demonstrated benefit for progression of CKD for semaglutide (sa) Potential benefit for dulaglutide, liraglutide, or semaglutide Monitor kidney function when initiat- ing or escalating doses in individuals with kidney impair-ment reporting severe adverse Gl reactions See labels of individ Potential benefit ual agents for dosage considerations for kidney function No dose adjustment Monitor kidney function when initiating or esca lating doses in individu- als with kidney impair ment reporting severe adverse Gl reactions 12/33 Clinical considerations and adverse effects Thyroid C-cell tumors identi fied in rodents; human rele- vance not determined Provide guidance on discon tinuation prior to surgical procedures to mitigate potential for pulmonary aspiration with general anesthesia or deep sedation Pancreatitis: acute pancrea-titis has been reported, but causality has not been established; do not initiate if at high risk for pancreatitis, and discontinue if pancreati tis is suspected Biliary disease: evaluate for gallbladder disease if chole-lithiasis or cholecystitis is suspected; avoid use in at-risk individuals Ileus: reported, but risk level is not well established Diabetic retinopathy: close monitoring of retinopathy in those at high risk (older individuals and those with longer duration of T2D (≥10 years]) Nonarteritic anterior ische- mic optic neuropathy (NAION) reported (rare inci- dence); monitor for NAION during eye examinations Impact on drug absorption: orally administered drug ab sorption may be impaired during dose titration (includ- ing oral contraceptives) Gl side effects: counsel on potential for GI side effects; provide guidance on dietary modifications to mitigate Gl side effects (reduction in meal size, mindful eating practices [e.g., stop eating Continued Give me dosage, how many times a day , titration, maximum dosages, how long and indication and contraindications from Ada 2026 guidelines for GLP-1 RAS (SQ; AND Dual GIP and Very high GLP-1 RA (SQ) make me a flowchart image like before if possible both in same image
ADA 2026 GLP-1 RA semaglutide dulaglutide liraglutide dosage titration maximum dose indication contraindication table 9.2
ADA 2026 tirzepatide GIP GLP-1 dual agonist dosage titration indication contraindication guidelines
https://pmc.ncbi.nlm.nih.gov/articles/PMC12690185
https://www.dralo.net/blog/diabetes-guidelines-2026
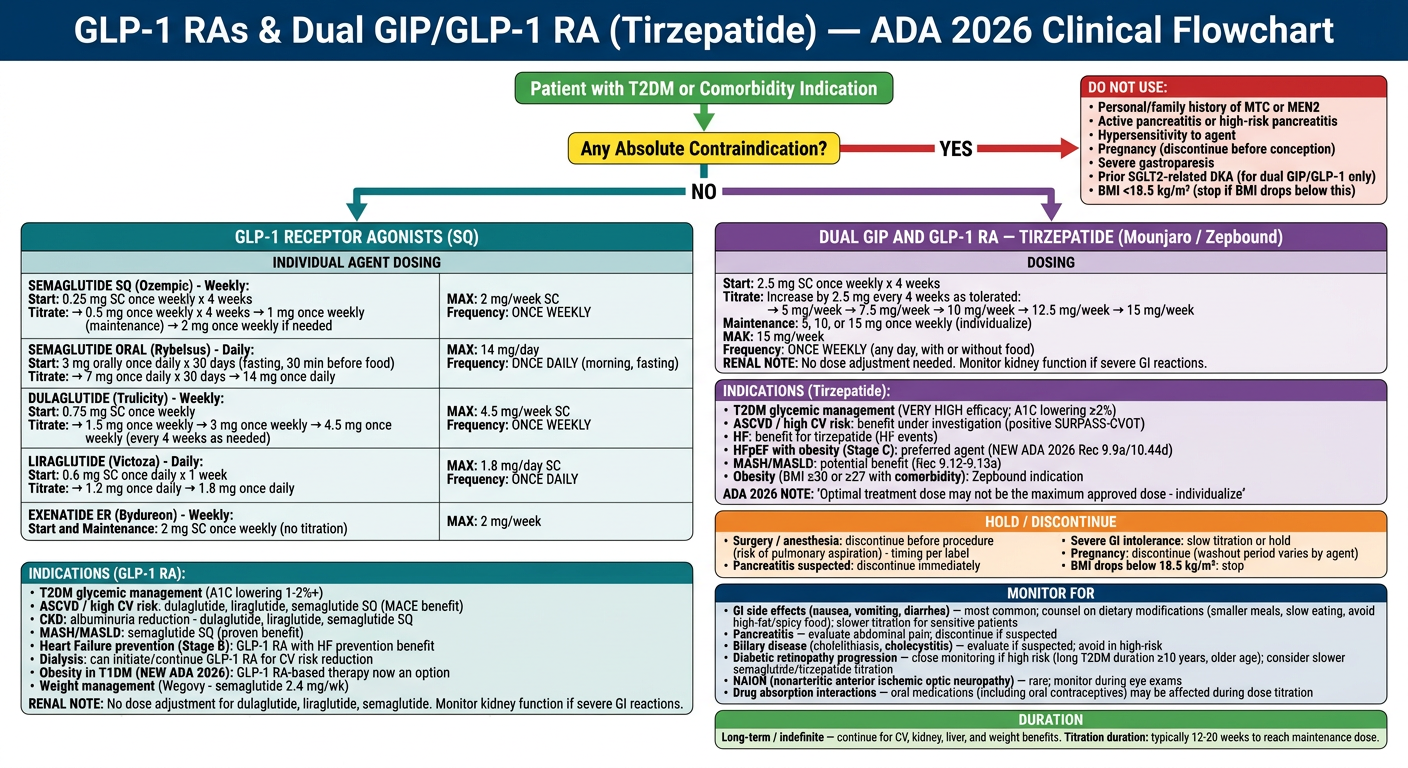
A large, clean, professional medical flowchart on white background titled "GLP-1 RAs & Dual GIP/GLP-1 RA (Tirzepatide) — ADA 2026 Clinical Flowchart". Two clearly separated color-coded sections side by side. Professional medical style with readable fonts, color-coded boxes, clear arrows. The chart has TWO PARALLEL COLUMNS after a shared top section: ===TOP SHARED SECTION=== GREEN START BOX (top center): "Patient with T2DM or Comorbidity Indication" Arrow down to YELLOW DIAMOND: "Any Absolute Contraindication?" YES → RED BOX (right): "DO NOT USE: • Personal/family history of MTC or MEN2 • Active pancreatitis or high-risk pancreatitis • Hypersensitivity to agent • Pregnancy (discontinue before conception) • Severe gastroparesis • Prior SGLT2-related DKA (for dual GIP/GLP-1 only) • BMI <18.5 kg/m² (stop if BMI drops below this)" NO → Arrow splits into TWO COLUMNS: ===LEFT COLUMN: GLP-1 RAs (SQ + Oral Semaglutide)=== Header box (TEAL/DARK CYAN): "GLP-1 RECEPTOR AGONISTS (SQ)" Sub-box labeled "INDIVIDUAL AGENT DOSING": Row 1 - SEMAGLUTIDE SQ (Ozempic) - Weekly: Start: 0.25 mg SC once weekly x 4 weeks Titrate: → 0.5 mg once weekly x 4 weeks → 1 mg once weekly (maintenance) → 2 mg once weekly if needed MAX: 2 mg/week SC Frequency: ONCE WEEKLY Row 2 - SEMAGLUTIDE ORAL (Rybelsus) - Daily: Start: 3 mg orally once daily x 30 days (fasting, 30 min before food) Titrate: → 7 mg once daily x 30 days → 14 mg once daily MAX: 14 mg/day Frequency: ONCE DAILY (morning, fasting) Row 3 - DULAGLUTIDE (Trulicity) - Weekly: Start: 0.75 mg SC once weekly Titrate: → 1.5 mg once weekly → 3 mg once weekly → 4.5 mg once weekly (every 4 weeks as needed) MAX: 4.5 mg/week SC Frequency: ONCE WEEKLY Row 4 - LIRAGLUTIDE (Victoza) - Daily: Start: 0.6 mg SC once daily x 1 week Titrate: → 1.2 mg once daily → 1.8 mg once daily MAX: 1.8 mg/day SC Frequency: ONCE DAILY Row 5 - EXENATIDE ER (Bydureon) - Weekly: Start and Maintenance: 2 mg SC once weekly (no titration) MAX: 2 mg/week TEAL BOX - INDICATIONS (GLP-1 RA): • T2DM glycemic management (A1C lowering 1-2%+) • ASCVD / high CV risk: dulaglutide, liraglutide, semaglutide SQ (MACE benefit) • CKD: albuminuria reduction - dulaglutide, liraglutide, semaglutide SQ • MASH/MASLD: semaglutide SQ (proven benefit) • Heart Failure prevention (Stage B): GLP-1 RA with HF prevention benefit • Dialysis: can initiate/continue GLP-1 RA for CV risk reduction • Obesity in T1DM (NEW ADA 2026): GLP-1 RA-based therapy now an option • Weight management (Wegovy - semaglutide 2.4 mg/wk) RENAL NOTE: No dose adjustment for dulaglutide, liraglutide, semaglutide. Monitor kidney function if severe GI reactions. ===RIGHT COLUMN: DUAL GIP/GLP-1 RA (Tirzepatide)=== Header box (PURPLE): "DUAL GIP AND GLP-1 RA — TIRZEPATIDE (Mounjaro / Zepbound)" Sub-box "DOSING": Start: 2.5 mg SC once weekly x 4 weeks Titrate: Increase by 2.5 mg every 4 weeks as tolerated: → 5 mg/week → 7.5 mg/week → 10 mg/week → 12.5 mg/week → 15 mg/week Maintenance: 5, 10, or 15 mg once weekly (individualize) MAX: 15 mg/week Frequency: ONCE WEEKLY (any day, with or without food) RENAL NOTE: No dose adjustment needed. Monitor kidney function if severe GI reactions. PURPLE BOX - INDICATIONS (Tirzepatide): • T2DM glycemic management (VERY HIGH efficacy; A1C lowering ≥2%) • ASCVD / high CV risk: benefit under investigation (positive SURPASS-CVOT) • HF: benefit for tirzepatide (HF events) • HFpEF with obesity (Stage C): preferred agent (NEW ADA 2026 Rec 9.9a/10.44d) • MASH/MASLD: potential benefit (Rec 9.12-9.13a) • Obesity (BMI ≥30 or ≥27 with comorbidity): Zepbound indication • Obesity in T1DM (NEW ADA 2026) ADA 2026 NOTE: "Optimal treatment dose may not be the maximum approved dose - individualize" ===BOTTOM SHARED SECTION (spans both columns)=== ORANGE BOX - "HOLD / DISCONTINUE": • Surgery / anesthesia: discontinue before procedure (risk of pulmonary aspiration) - timing per label • Pancreatitis suspected: discontinue immediately • Severe GI intolerance: slow titration or hold • Pregnancy: discontinue (washout period varies by agent) • BMI drops below 18.5 kg/m²: stop DARK BLUE BOX - "MONITOR FOR": • GI side effects (nausea, vomiting, diarrhea) — most common; counsel on dietary modifications (smaller meals, slow eating, avoid high-fat/spicy food); slower titration for sensitive patients • Pancreatitis — evaluate abdominal pain; discontinue if suspected • Biliary disease (cholelithiasis, cholecystitis) — evaluate if suspected; avoid in high-risk • Diabetic retinopathy progression — close monitoring if high risk (long T2DM duration ≥10 years, older age); consider slower semaglutide/tirzepatide titration • NAION (nonarteritic anterior ischemic optic neuropathy) — rare; monitor during eye exams • Drug absorption interactions — oral medications (including oral contraceptives) may be affected during dose titration DURATION BOX (green): "Long-term / indefinite — continue for CV, kidney, liver, and weight benefits. Titration duration: typically 12-20 weeks to reach maintenance dose." White background, well-spaced, large readable text, color-coded headers, professional clean medical layout.
GLP-1 RAs & Dual GIP/GLP-1 RA — ADA 2026 Standards of Care
PART 1: GLP-1 RECEPTOR AGONISTS (Subcutaneous + Oral)
Individual Agent Dosing
Semaglutide SQ (Ozempic) — Once Weekly
| Phase | Dose | Duration at Each Step |
|---|---|---|
| Start | 0.25 mg SC once weekly | 4 weeks |
| Step 2 | 0.5 mg SC once weekly | 4 weeks (maintenance for many) |
| Step 3 | 1 mg SC once weekly | 4 weeks |
| Maximum | 2 mg SC once weekly | Maintenance |
Semaglutide Oral (Rybelsus) — Once Daily
| Phase | Dose | Duration at Each Step |
|---|---|---|
| Start | 3 mg orally once daily | 30 days (dose escalation only - not therapeutic) |
| Step 2 | 7 mg orally once daily | 30 days |
| Maximum | 14 mg orally once daily | Maintenance |
Dulaglutide (Trulicity) — Once Weekly
| Phase | Dose | Duration at Each Step |
|---|---|---|
| Start | 0.75 mg SC once weekly | 4 weeks |
| Step 2 | 1.5 mg SC once weekly | 4 weeks (maintenance for many) |
| Step 3 | 3 mg SC once weekly | 4 weeks |
| Maximum | 4.5 mg SC once weekly | Maintenance |
Liraglutide (Victoza) — Once Daily
| Phase | Dose | Duration at Each Step |
|---|---|---|
| Start | 0.6 mg SC once daily | 1 week (tolerance dose only) |
| Step 2 | 1.2 mg SC once daily | Maintenance for many |
| Maximum | 1.8 mg SC once daily | Maintenance |
Exenatide ER (Bydureon BCise) — Once Weekly
| Phase | Dose |
|---|---|
| Start & Maintenance | 2 mg SC once weekly (no titration) |
| Maximum | 2 mg/week |
GLP-1 RA Indications (ADA 2026)
| Indication | Agents |
|---|---|
| T2DM glycemic management | All agents; A1C lowering 1-2%+ |
| ASCVD / High CV risk - MACE reduction | Dulaglutide, Liraglutide, Semaglutide SQ & oral |
| CKD - albuminuria reduction / kidney endpoints | Dulaglutide, Liraglutide, Semaglutide SQ |
| Advanced CKD eGFR <30 | GLP-1 RA preferred over SGLT2-i for glycemic use |
| Dialysis | Can initiate/continue for CV risk reduction (Rec 11.11b) |
| MASH/MASLD | Semaglutide SQ (proven benefit); GLP-1 RA preferred (Rec 9.12) |
| Stage B HF (asymptomatic, high CV risk) | GLP-1 RA with HF prevention benefit (Rec 10.44c) |
| Obesity in T1DM (NEW ADA 2026) | GLP-1 RA-based therapy now a recognized option |
| Weight management | Semaglutide 2.4 mg/wk (Wegovy); liraglutide 3 mg/day (Saxenda) |
Renal Dosing (ADA 2026)
- No dose adjustment needed for dulaglutide, liraglutide, or semaglutide
- Monitor kidney function when initiating or escalating doses in patients with renal impairment who develop severe GI adverse reactions (dehydration risk)
PART 2: DUAL GIP AND GLP-1 RA — TIRZEPATIDE (Mounjaro / Zepbound)
Dosing — Once Weekly SQ
| Phase | Dose | Duration at Each Step |
|---|---|---|
| Start | 2.5 mg SC once weekly | 4 weeks |
| Step 2 | 5 mg SC once weekly | 4 weeks |
| Step 3 | 7.5 mg SC once weekly | 4 weeks |
| Step 4 | 10 mg SC once weekly | 4 weeks |
| Step 5 | 12.5 mg SC once weekly | 4 weeks |
| Maximum | 15 mg SC once weekly | Maintenance |
Renal Dosing (ADA 2026)
- No dose adjustment needed
- Monitor kidney function when initiating or escalating in patients with renal impairment with severe GI reactions
Tirzepatide Indications (ADA 2026)
| Indication | Notes |
|---|---|
| T2DM glycemic management | Very high efficacy; A1C lowering ≥2% |
| ASCVD / High CV risk | Benefit under investigation; positive SURPASS-CVOT vs dulaglutide |
| Heart Failure (general) | Benefit: tirzepatide |
| HFpEF with obesity (Stage C) - NEW ADA 2026 | Preferred dual GIP/GLP-1 RA (Rec 9.9a, 10.44d) |
| MASH/MASLD | Potential benefit; option for biopsy-proven MASH (Rec 9.13a) |
| Obesity (BMI ≥30 or ≥27 + comorbidity) | Zepbound indication |
| Obesity in T1DM - NEW ADA 2026 | Recognized treatment option |
SHARED CONTRAINDICATIONS (Both Classes — ADA 2026)
| Contraindication | Notes |
|---|---|
| Personal or family history of MTC | Medullary thyroid carcinoma - absolute contraindication |
| Multiple Endocrine Neoplasia type 2 (MEN2) | Absolute contraindication |
| Active pancreatitis | Do not initiate; discontinue if pancreatitis develops |
| High risk for pancreatitis | Do not initiate |
| Serious hypersensitivity to specific agent | Avoid that agent |
| Pregnancy | Discontinue; washout period required (varies by agent) |
| Severe gastroparesis | Avoid (GLP-1 RA slows gastric emptying) |
| BMI <18.5 kg/m² | Stop if BMI falls below this threshold |
When to Hold / Discontinue (ADA 2026)
| Situation | Action |
|---|---|
| Surgery / general anesthesia / deep sedation | Discontinue before procedure - risk of pulmonary aspiration (ADA 2026 specific guidance added); timing per individual agent label |
| Pancreatitis suspected | Discontinue immediately |
| Cholecystitis / cholelithiasis suspected | Evaluate; avoid in high-risk individuals |
| Severe vomiting/GI intolerance | Slow titration; hold if severe |
| Pregnancy planned | Discontinue with adequate washout |
Key Adverse Effects to Monitor (ADA 2026)
| Effect | Management |
|---|---|
| GI side effects (nausea, vomiting, diarrhea) - most common | Smaller meals, mindful eating, reduce high-fat/spicy food; slower titration; not recommended in gastroparesis |
| Pancreatitis | Evaluate abdominal pain; discontinue if confirmed |
| Biliary disease (gallstones, cholecystitis) | Evaluate if suspected; avoid in high-risk |
| Diabetic retinopathy progression | Close monitoring in high-risk (age, T2DM ≥10 years); consider slower semaglutide/tirzepatide titration to avoid rapid A1C drop |
| NAION (nonarteritic anterior ischemic optic neuropathy) | Rare; monitor during eye exams |
| Drug absorption | Orally administered drugs (including oral contraceptives) may have impaired absorption during dose titration |
| Thyroid C-cell tumors | Identified in rodents; human relevance not yet determined |
Duration


Add these two image as one image with same info
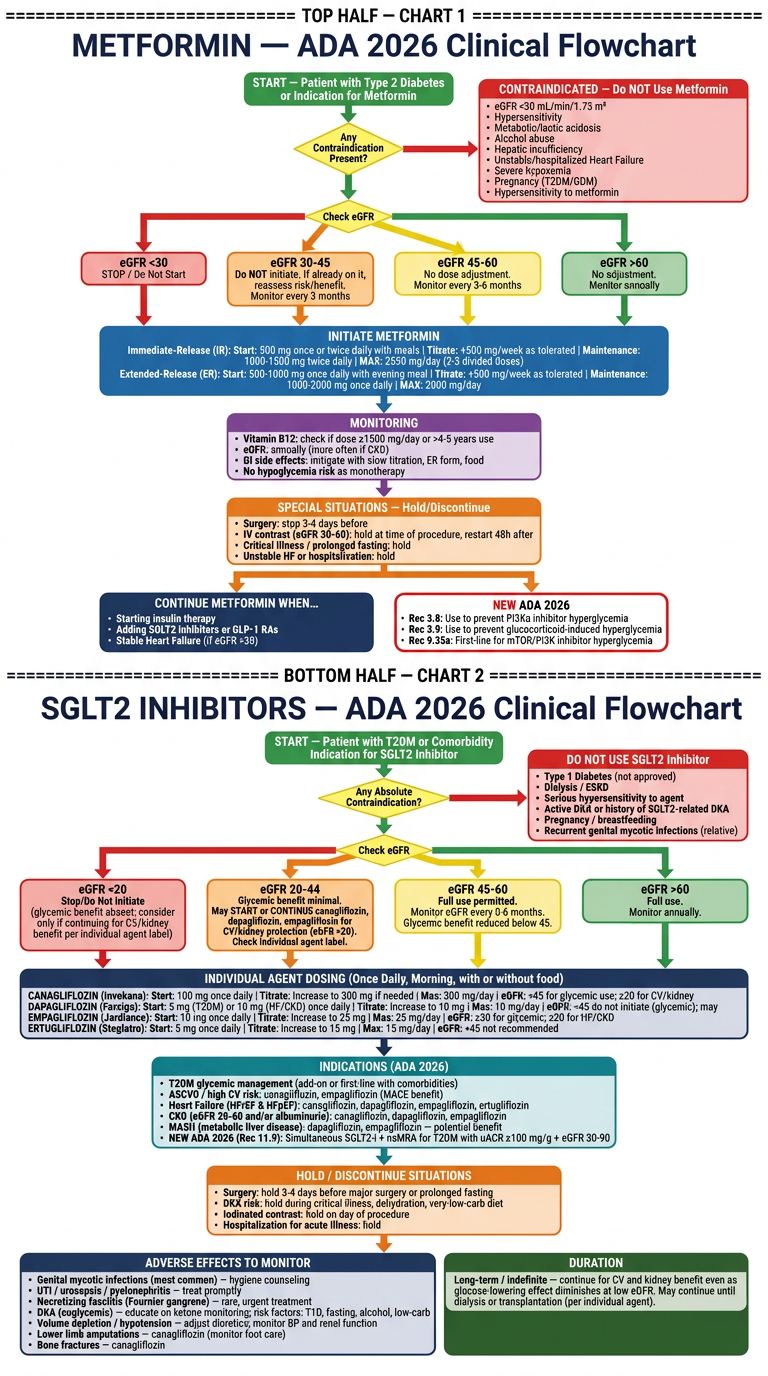
A very large, tall, professional medical reference poster on white background combining TWO complete clinical flowcharts stacked vertically. Both charts share the same professional style, color scheme, and formatting. Clean, readable fonts. All text must be legible. ======================================== TOP HALF — CHART 1 ======================================== TITLE (large dark blue bold): "METFORMIN — ADA 2026 Clinical Flowchart" LEFT SIDE - FLOWCHART PATH: GREEN box (START): "START — Patient with Type 2 Diabetes or Indication for Metformin" Arrow down to YELLOW DIAMOND: "Any Contraindication Present?" From diamond: - YES → thick red arrow RIGHT to RED box: "CONTRAINDICATED — Do NOT Use Metformin • eGFR <30 mL/min/1.73 m² • Hypersensitivity • Metabolic/lactic acidosis • Alcohol abuse • Hepatic insufficiency • Unstable/hospitalized Heart Failure • Severe hypoxemia • Pregnancy (T2DM/GDM) • Hypersensitivity to metformin" - NO → green arrow down to YELLOW DIAMOND: "Check eGFR" From eGFR diamond, 3 paths: - LEFT arrow "eGFR <30" → RED box: "STOP / Do Not Start" - MIDDLE arrow "eGFR 30-45" → ORANGE box: "Do NOT initiate. If already on it, reassess risk/benefit. Monitor every 3 months" - RIGHT arrow "eGFR 45-60" → YELLOW box: "No dose adjustment. Monitor every 3-6 months" - DOWN arrow "eGFR >60" → GREEN box: "No adjustment. Monitor annually" All eGFR >30 paths merge to BLUE box: "INITIATE METFORMIN Immediate-Release (IR): Start: 500 mg once or twice daily with meals | Titrate: +500 mg/week as tolerated | Maintenance: 1000-1500 mg twice daily | MAX: 2550 mg/day (2-3 divided doses) Extended-Release (ER): Start: 500-1000 mg once daily with evening meal | Titrate: +500 mg/week as tolerated | Maintenance: 1000-2000 mg once daily | MAX: 2000 mg/day" Arrow down to PURPLE box: "MONITORING • Vitamin B12: check if dose ≥1500 mg/day or >4-5 years use • eGFR: annually (more often if CKD) • GI side effects: mitigate with slow titration, ER form, food • No hypoglycemia risk as monotherapy" Arrow down to ORANGE box: "SPECIAL SITUATIONS — Hold/Discontinue • Surgery: stop 3-4 days before • IV contrast (eGFR 30-60): hold at time of procedure, restart 48h after • Critical illness / prolonged fasting: hold • Unstable HF or hospitalization: hold" Arrow down, splits to TWO boxes side by side: LEFT DARK BLUE box: "CONTINUE METFORMIN WHEN… • Starting insulin therapy • Adding SGLT2 inhibitors or GLP-1 RAs • Stable Heart Failure (if eGFR >30)" RIGHT RED-BORDERED box labeled "NEW ADA 2026": "• Rec 3.8: Use to prevent PI3Kα inhibitor hyperglycemia • Rec 3.9: Use to prevent glucocorticoid-induced hyperglycemia • Rec 9.35a: First-line for mTOR/PI3K inhibitor hyperglycemia" THICK HORIZONTAL DIVIDER LINE between Chart 1 and Chart 2 ======================================== BOTTOM HALF — CHART 2 ======================================== TITLE (large dark navy bold): "SGLT2 INHIBITORS — ADA 2026 Clinical Flowchart" GREEN box (START): "START — Patient with T2DM or Comorbidity Indication for SGLT2 Inhibitor" Arrow down to YELLOW DIAMOND: "Any Absolute Contraindication?" YES → RED box: "DO NOT USE SGLT2 Inhibitor: • Type 1 Diabetes (not approved) • Dialysis / ESKD • Serious hypersensitivity to agent • Active DKA or history of SGLT2-related DKA • Pregnancy / breastfeeding • Recurrent genital mycotic infections (relative)" NO → down to YELLOW DIAMOND: "Check eGFR" From eGFR diamond, 4 paths: - "eGFR <20" → RED box: "Stop/Do Not Initiate (glycemic benefit absent; consider only if continuing for CV/kidney benefit per individual agent label)" - "eGFR 20-44" → ORANGE box: "Glycemic benefit minimal. May START or CONTINUE canagliflozin, dapagliflozin, empagliflozin for CV/kidney protection (eGFR >20). Check individual agent label." - "eGFR 45-60" → YELLOW box: "Full use permitted. Monitor eGFR every 3-6 months. Glycemic benefit reduced below 45." - "eGFR >60" → GREEN box: "Full use. Monitor annually." All eGFR >20 paths merge to DARK BLUE box: "INDIVIDUAL AGENT DOSING (Once Daily, Morning, with or without food) CANAGLIFLOZIN (Invokana): Start: 100 mg once daily | Titrate: Increase to 300 mg if needed | Max: 300 mg/day | eGFR: <45 for glycemic use; ≥20 for CV/kidney DAPAGLIFLOZIN (Farxiga): Start: 5 mg (T2DM) or 10 mg (HF/CKD) once daily | Titrate: Increase to 10 mg | Max: 10 mg/day | eGFR: <45 do not initiate (glycemic); may continue ≥25 for kidney/CV EMPAGLIFLOZIN (Jardiance): Start: 10 mg once daily | Titrate: Increase to 25 mg | Max: 25 mg/day | eGFR: ≥30 for glycemic; ≥20 for HF/CKD ERTUGLIFLOZIN (Steglatro): Start: 5 mg once daily | Titrate: Increase to 15 mg | Max: 15 mg/day | eGFR: <45 not recommended" Arrow down to TEAL box: "INDICATIONS (ADA 2026) • T2DM glycemic management (add-on or first-line with comorbidities) • ASCVD / high CV risk: canagliflozin, empagliflozin (MACE benefit) • Heart Failure (HFrEF & HFpEF): canagliflozin, dapagliflozin, empagliflozin, ertugliflozin • CKD (eGFR 20-60 and/or albuminuria): canagliflozin, dapagliflozin, empagliflozin • MASH (metabolic liver disease): dapagliflozin, empagliflozin — potential benefit • NEW ADA 2026 (Rec 11.9): Simultaneous SGLT2-i + nsMRA for T2DM with uACR ≥100 mg/g + eGFR 30-90" Arrow down to ORANGE box: "HOLD / DISCONTINUE SITUATIONS • Surgery: hold 3-4 days before major surgery or prolonged fasting • DKA risk: hold during critical illness, dehydration, very-low-carb diet • Iodinated contrast: hold on day of procedure • Hospitalization for acute illness: hold" Arrow down to wide box split into two sections: LEFT DARK BLUE section: "ADVERSE EFFECTS TO MONITOR • Genital mycotic infections (most common) — hygiene counseling • UTI / urosepsis / pyelonephritis — treat promptly • Necrotizing fasciitis (Fournier gangrene) — rare, urgent treatment • DKA (euglycemic) — educate on ketone monitoring; risk factors: T1D, fasting, alcohol, low-carb • Volume depletion / hypotension — adjust diuretics; monitor BP and renal function • Lower limb amputations — canagliflozin (monitor foot care) • Bone fractures — canagliflozin" RIGHT DARK GREEN section: "DURATION Long-term / indefinite — continue for CV and kidney benefit even as glucose-lowering effect diminishes at low eGFR. May continue until dialysis or transplantation (per individual agent)." Use: white background throughout, color-coded boxes exactly as described (green=start/go, red=stop/contraindication, yellow=caution/decision, orange=warning/hold, blue=dosing/action, purple=monitoring, teal=indications, dark navy=headers), clear directional arrows, bold section titles, clean professional medical poster layout. Make all text clearly readable. The image should be very tall to accommodate both complete flowcharts.
- Contraindication screening → eGFR pathway → IR/ER dosing → Monitoring → Hold situations → Continue when... → New 2026 recommendations
- Absolute contraindications → eGFR decision pathway → All 4 individual agents with doses → Indications → Hold situations → Adverse effects → Duration
DPP-4 inhibitors Intermediate (oral) No Neutral Neutral Neutral (potential risk: saxagliptin) Neutral Pioglitazone (oral) Dose adjustment required based on kidney function Unknown gastroparesis consider slower dose titra-tion for those experiencing Gl challenges; not recom-mended for individuals with Pancreatitis has been reported but causality has not been established; discontinue if High No Gain Potential benefit Neutral Increased risk Neutral Neutral Neutral (sitagliptin, saxagliptin, alogliptin) No dose adjustment required for linagliptin No dose adjustment Potential benefit required impairment due to potential for fluid retention Generally not recom-mended in kidney Glyburide: generally not recommended in Unknown CKD Glipizide and glimepiride: initiate conservatively to avoid hypoglycemia Sulfonylureas (2nd generation) (oral) High Yes Gain Use with caution in individ-uals at risk for hypoglyce-mia, particularly if in combi-nation with insulin once full], decreasing intake of high-fat or spicy food); pancreatitis is suspected Postmarketing concerns about joint pain (consider discontinuing if debilitating and other treatment options are feasible) and bullous pemphigoid (discontinue if suspected) reversible upon discontinuation Increased risk of HF and fluid retention; do not use in setting of HF Risk of bone fractures Bladder cancer: do not use in individuals with active bladder cancer, and use caution in those with prior history of bladder cancer; association observed with higher cumulative exposure (e.g., longer duration, higher doses) FDA Special Warning on in-creased risk of CV mortality based on studies of an older sulfonylurea (tolbutamide); glimepiride shown to be CV
ADA 2026 DPP-4 inhibitors sitagliptin saxagliptin linagliptin alogliptin dosage titration maximum dose indication contraindication table 9.2
ADA 2026 pioglitazone sulfonylureas glipizide glimepiride glyburide dosage titration maximum dose contraindication table 9.2
https://pmc.ncbi.nlm.nih.gov/articles/PMC12690185
sitagliptin saxagliptin linagliptin alogliptin dose renal adjustment eGFR pioglitazone dose maximum glipizide glimepiride dosing 2025 2026
A very large, tall professional medical reference poster on white background combining TWO complete clinical flowcharts stacked vertically with a thick dividing line between them. Clean, readable fonts, color-coded boxes, clear directional arrows. Professional medical style. ======================================== TOP HALF — CHART 1: DPP-4 INHIBITORS ======================================== TITLE (large dark blue bold text, centered): "DPP-4 INHIBITORS — ADA 2026 Clinical Flowchart" LEFT FLOWCHART PATH: GREEN START BOX: "START — Patient with T2DM — Consider DPP-4 Inhibitor" Arrow down to YELLOW DIAMOND: "Any Contraindication?" YES arrow → RED BOX: "DO NOT USE / CAUTION: • History of pancreatitis (do not initiate) • Serious hypersensitivity to agent • Saxagliptin: avoid in heart failure (potential risk) • Avoid DPP-4i + GLP-1 RA combination (no added benefit) • Heart failure: saxagliptin associated with increased HF hospitalizations • Severe hepatic impairment (alogliptin)" NO arrow → YELLOW DIAMOND: "Check eGFR" eGFR paths: "eGFR ≥45" → GREEN box: "Full dose — no adjustment needed for any agent" "eGFR 30-44" → YELLOW box: "Reduce sitagliptin to 50 mg/day | Reduce saxagliptin to 2.5 mg/day | Reduce alogliptin to 12.5 mg/day | Linagliptin: NO adjustment" "eGFR <30 or dialysis" → ORANGE box: "Reduce sitagliptin to 25 mg/day | Saxagliptin: 2.5 mg/day (not recommended in HD) | Reduce alogliptin to 6.25 mg/day | Linagliptin: NO adjustment — preferred agent in CKD" All paths merge → BLUE DOSING BOX: "INDIVIDUAL AGENT DOSING (Once Daily, With or Without Food) SITAGLIPTIN (Januvia): 100 mg once daily | Renal: 50 mg (eGFR 30-44); 25 mg (eGFR <30/dialysis) | MAX: 100 mg/day SAXAGLIPTIN (Onglyza): 2.5 mg or 5 mg once daily | Renal: 2.5 mg if eGFR <45 | MAX: 5 mg/day | Avoid in HF LINAGLIPTIN (Tradjenta): 5 mg once daily | NO renal adjustment needed | MAX: 5 mg/day — PREFERRED in CKD ALOGLIPTIN (Nesina): 25 mg once daily | Renal: 12.5 mg (eGFR 30-59); 6.25 mg (eGFR <30/dialysis) | MAX: 25 mg/day" TEAL INDICATIONS BOX: "INDICATIONS (ADA 2026) • T2DM glycemic management (add-on therapy) — A1C lowering ~0.7-1.0% • Patients at risk for hypoglycemia (no hypoglycemia risk as monotherapy) • Weight-neutral option when weight gain undesirable • Post-transplant: DPP-4i for mild hyperglycemia (Rec 9.37 — NEW ADA 2026) • Preferred in frailty and older adults (NICE/ADA) • Note: Do NOT combine with GLP-1 RA — no added benefit" PURPLE MONITORING BOX: "ADVERSE EFFECTS & MONITORING • Pancreatitis: reported but causality unestablished; discontinue if suspected • Joint pain (arthralgia): consider discontinuing if debilitating • Bullous pemphigoid: discontinue if suspected — reversible • Saxagliptin: increased HF hospitalization risk — avoid in HF patients • Renal function: monitor periodically for dose adjustments" THICK DIVIDING LINE ======================================== BOTTOM HALF — CHART 2: PIOGLITAZONE & SULFONYLUREAS ======================================== TITLE (large dark maroon bold, centered): "PIOGLITAZONE & SULFONYLUREAS — ADA 2026 Clinical Flowchart" TWO SIDE-BY-SIDE COLUMNS: LEFT COLUMN — PIOGLITAZONE (Actos) — Header in DARK TEAL: GREEN START: "Patient with T2DM — Consider Pioglitazone" YELLOW DIAMOND: "Any Contraindication?" YES → RED BOX: "DO NOT USE: • Active Heart Failure (NYHA Class III-IV) — increased HF risk and fluid retention • Active bladder cancer • Caution: prior history of bladder cancer • Severe hepatic impairment • Osteoporosis / high fracture risk • Pregnancy" NO → BLUE DOSING BOX: "PIOGLITAZONE DOSING (Once Daily, With or Without Food): Start: 15 mg or 30 mg once daily Titrate: Increase by 15 mg every 4-8 weeks as tolerated MAX: 45 mg/day Renal: Generally not recommended in kidney impairment due to potential for fluid retention Frequency: ONCE DAILY" ORANGE INDICATIONS BOX: "INDICATIONS (ADA 2026) • T2DM glycemic management — HIGH efficacy (A1C reduction similar to metformin) • MASH/biopsy-proven MASH — potential benefit (Rec 9.13a — ADA 2026) • Insulin-sparing: adjunctive to insulin (reduces insulin dose needed) • Cardiovascular: potential benefit (PROactive trial data)" PURPLE ADVERSE EFFECTS: "MONITOR: • Fluid retention / edema — dose-related; avoid in HF • Weight gain — significant (3-4 kg average) • Heart failure risk — increased; do not use in HF • Bone fractures — increased risk (especially women) • Bladder cancer — do not use if active; caution if prior history • Hepatotoxicity — monitor LFTs" RIGHT COLUMN — SULFONYLUREAS (2nd Generation) — Header in DARK RED: GREEN START: "Patient with T2DM — Consider Sulfonylurea" YELLOW DIAMOND: "Any Contraindication?" YES → RED BOX: "DO NOT USE / CAUTION: • Glyburide: generally NOT recommended in CKD • Sulfa allergy (all agents) • Type 1 Diabetes / DKA • Pregnancy (insulin preferred) • Severe hepatic or renal impairment • High hypoglycemia risk (elderly, frail, irregular meals)" NO → BLUE DOSING BOX: "INDIVIDUAL SULFONYLUREA DOSING (With Meals) GLIPIZIDE (Glucotrol): Start: 5 mg once daily before breakfast | Titrate: +2.5-5 mg/week | MAX: 40 mg/day IR (20 mg/day XL) | Frequency: 1-2x daily (XL once daily) GLIMEPIRIDE (Amaryl): Start: 1-2 mg once daily with first meal | Titrate: +1-2 mg every 1-2 weeks | MAX: 8 mg/day | Frequency: ONCE DAILY GLYBURIDE (DiaBeta): Start: 2.5-5 mg once daily with breakfast | Titrate: +2.5 mg/week | MAX: 20 mg/day | Frequency: 1-2x daily | AVOID in CKD" TEAL INDICATIONS BOX: "INDICATIONS (ADA 2026) • T2DM glycemic management — HIGH efficacy (A1C reduction 1-2%) • Cost-effective option when affordability is a priority • Glimepiride: CV-safe (shown non-inferior in CAROLINA trial) • Note ADA 2026: Limit/discontinue SU when GLP-1 RA or SGLT2-i initiated — no added CV/kidney/weight benefit" ORANGE RENAL DOSING BOX: "RENAL CONSIDERATIONS (ADA 2026): • Glyburide: GENERALLY NOT RECOMMENDED in CKD (active metabolite accumulates — hypoglycemia risk) • Glipizide: PREFERRED sulfonylurea in CKD — initiate conservatively • Glimepiride: Use conservatively in CKD — initiate at 1 mg/day; monitor closely • All: Initiate at lowest dose to avoid hypoglycemia in renal impairment" PURPLE ADVERSE EFFECTS: "MONITOR: • Hypoglycemia — YES (significant risk, especially with insulin combination) • Weight gain — significant • FDA warning: increased CV mortality (older sulfonylurea tolbutamide); glimepiride shown CV-safe • Avoid in combination with insulin without careful dose reduction" BOTTOM FOOTER BOX (spans full width, dark navy): "ADA 2026 KEY POSITION: DPP-4 inhibitors, sulfonylureas, and pioglitazone are considered second-line or adjunctive agents. When GLP-1 RAs or SGLT2 inhibitors are initiated, ADA 2026 recommends limiting or discontinuing DPP-4i and sulfonylureas as they provide no additional CV, kidney, weight, or liver benefit. Pioglitazone may be continued adjunctively for MASH or insulin-sparing benefit." White background, professional medical poster, color-coded sections, bold headers, readable text, clear arrows. Very tall image to fit all content.
DPP-4 inhibitors Intermediate (oral) No Neutral Neutral Neutral (potential risk: saxagliptin) Neutral Pioglitazone (oral) Dose adjustment required based on kidney function Unknown gastroparesis consider slower dose titra-tion for those experiencing Gl challenges; not recom-mended for individuals with Pancreatitis has been reported but causality has not been established; discontinue if High No Gain Potential benefit Neutral Increased risk Neutral Neutral Neutral (sitagliptin, saxagliptin, alogliptin) No dose adjustment required for linagliptin No dose adjustment Potential benefit required impairment due to potential for fluid retention Generally not recom-mended in kidney Glyburide: generally not recommended in Unknown CKD Glipizide and glimepiride: initiate conservatively to avoid hypoglycemia Sulfonylureas (2nd generation) (oral) High Yes Gain Use with caution in individ-uals at risk for hypoglyce-mia, particularly if in combi-nation with insulin once full], decreasing intake of high-fat or spicy food); pancreatitis is suspected Postmarketing concerns about joint pain (consider discontinuing if debilitating and other treatment options are feasible) and bullous pemphigoid (discontinue if suspected) reversible upon discontinuation Increased risk of HF and fluid retention; do not use in setting of HF Risk of bone fractures Bladder cancer: do not use in individuals with active bladder cancer, and use caution in those with prior history of bladder cancer; association observed with higher cumulative exposure (e.g., longer duration, higher doses) FDA Special Warning on in-creased risk of CV mortality based on studies of an older sulfonylurea (tolbutamide); glimepiride shown to be CV. Give me dosage, how many times a day , titration, maximum dosages, how long and indication and contraindications from Ada 2026 guidelines for DPP-4 inhibitors ,Pioglitazone (oral)AND Sulfonylureas (2nd generation) (oral) make me a flowchart image like before if possible both in same image
DPP-4 inhibitors sitagliptin saxagliptin linagliptin alogliptin dosage titration renal adjustment ADA 2026
pioglitazone sulfonylureas glipizide glimepiride glyburide dosage titration maximum dose contraindication ADA 2026 CKD
A very large professional medical reference poster on white background with THREE complete clinical flowcharts arranged as follows: TOP section = DPP-4 Inhibitors, MIDDLE section = Pioglitazone, BOTTOM section = Sulfonylureas 2nd Generation. Separated by thick colored divider lines. Color-coded boxes, clear arrows, bold headings, clean readable fonts. Professional medical style. ======================================== TOP SECTION — DPP-4 INHIBITORS ======================================== LARGE DARK BLUE TITLE: "DPP-4 INHIBITORS (Oral) — ADA 2026 Clinical Flowchart" GREEN START BOX: "START — Patient with T2DM — Consider DPP-4 Inhibitor" Arrow down → YELLOW DIAMOND: "Any Contraindication?" YES → RED BOX (right): "DO NOT USE / CAUTION: • Hypersensitivity to specific agent • Personal or family history of pancreatitis (avoid / high caution) • Saxagliptin: avoid in Heart Failure — associated with increased HF hospitalization risk • DO NOT combine with GLP-1 RA — no added glycemic benefit • Severe hepatic impairment (alogliptin: use caution)" NO → down → YELLOW DIAMOND: "Check eGFR" Three arrows from eGFR diamond: "eGFR ≥45" → GREEN box: "Full dose — no adjustment for any agent" "eGFR 30-44" → YELLOW/ORANGE box: "Sitagliptin → 50 mg once daily Saxagliptin → 2.5 mg once daily Alogliptin → 12.5 mg once daily Linagliptin → 5 mg once daily (NO change)" "eGFR <30 / Dialysis" → ORANGE box: "Sitagliptin → 25 mg once daily Saxagliptin → 2.5 mg once daily (not ideal in HD) Alogliptin → 6.25 mg once daily Linagliptin → 5 mg once daily (PREFERRED in CKD — NO adjustment)" All paths merge → BLUE DOSING BOX: "INDIVIDUAL AGENT DOSING — Once Daily, With or Without Food SITAGLIPTIN (Januvia): Start & Maintenance: 100 mg once daily | MAX: 100 mg/day | Renal: 50 mg (eGFR 30-44); 25 mg (eGFR <30/dialysis) SAXAGLIPTIN (Onglyza): Start: 2.5-5 mg once daily | MAX: 5 mg/day | Renal: 2.5 mg if eGFR <45 | AVOID in heart failure LINAGLIPTIN (Tradjenta): 5 mg once daily | MAX: 5 mg/day | NO renal adjustment — PREFERRED in CKD ALOGLIPTIN (Nesina): 25 mg once daily | MAX: 25 mg/day | Renal: 12.5 mg (eGFR 30-59); 6.25 mg (eGFR <30/dialysis) No titration needed for any DPP-4 inhibitor — fixed doses" TEAL INDICATIONS BOX: "INDICATIONS (ADA 2026) • T2DM glycemic management as add-on therapy (A1C lowering ~0.7-1.0%) • Weight-neutral option — no hypoglycemia risk as monotherapy • Preferred in frailty and older adults (minimal side effects, once-daily dosing) • Post-transplant: DPP-4i recommended for mild hyperglycemia (NEW ADA 2026 Rec 9.37) • Useful when GLP-1 RA not tolerated or affordable • ADA 2026: Limit/discontinue DPP-4i when GLP-1 RA started (no added CV/kidney/weight benefit)" PURPLE ADVERSE EFFECTS BOX: "ADVERSE EFFECTS TO MONITOR • Pancreatitis: reported; causality not established — discontinue if suspected • Joint pain (arthralgia): consider discontinuing if debilitating • Bullous pemphigoid: discontinue if suspected — reversible on discontinuation • Saxagliptin: increased HF hospitalization risk — avoid in HF patients • Nasopharyngitis and upper respiratory tract infections: common class effect • Duration: Long-term / indefinite as needed for glycemic control" THICK RED DIVIDER LINE ======================================== MIDDLE SECTION — PIOGLITAZONE ======================================== LARGE DARK TEAL TITLE: "PIOGLITAZONE (Oral — Thiazolidinedione) — ADA 2026 Clinical Flowchart" GREEN START BOX: "START — Patient with T2DM — Consider Pioglitazone" Arrow → YELLOW DIAMOND: "Any Contraindication?" YES → RED BOX: "DO NOT USE: • Active Heart Failure (any class) — increased HF risk and fluid retention • Active bladder cancer — absolute contraindication • Prior bladder cancer — use with caution (higher cumulative dose/duration = higher risk) • Severe hepatic impairment (ALT >2.5x ULN) • Pregnancy • Osteoporosis / high fracture risk — increased bone fracture risk • Edema / fluid overload states" NO → BLUE DOSING BOX: "PIOGLITAZONE DOSING — Once Daily, With or Without Food Start: 15 mg or 30 mg once daily Titrate: Increase by 15 mg every 8-12 weeks as tolerated and based on glycemic response Maintenance: 30-45 mg once daily MAX: 45 mg/day Frequency: ONCE DAILY Renal: Generally NOT recommended in kidney impairment — risk of fluid retention and edema Duration: Long-term as tolerated; benefits accumulate over months" TEAL INDICATIONS BOX: "INDICATIONS (ADA 2026) • T2DM glycemic management — HIGH efficacy (A1C reduction 1-1.5%) • MASH / Biopsy-proven MASH or high risk for liver fibrosis — potential benefit (ADA 2026 Rec 9.13a) • Adjunct to insulin — reduces insulin dose requirement • Cardiovascular: potential benefit (PROactive trial) • Alternative when GLP-1 RA/SGLT2-i not available or not tolerated" ORANGE ADVERSE EFFECTS BOX: "ADVERSE EFFECTS TO MONITOR • Fluid retention / peripheral edema — dose-related; avoid in HF • Weight gain — significant (2-4 kg) • Heart failure risk — increased; do NOT use in active HF • Bone fractures — increased risk, especially postmenopausal women • Bladder cancer — do not use if active; caution with longer use / higher doses • Monitor LFTs before initiating and periodically" THICK DARK RED DIVIDER LINE ======================================== BOTTOM SECTION — SULFONYLUREAS (2nd GENERATION) ======================================== LARGE DARK MAROON TITLE: "SULFONYLUREAS — 2nd Generation (Oral) — ADA 2026 Clinical Flowchart" GREEN START BOX: "START — Patient with T2DM — Consider Sulfonylurea" Arrow → YELLOW DIAMOND: "Any Contraindication?" YES → RED BOX: "DO NOT USE / CAUTION: • Type 1 Diabetes / DKA • Sulfa drug allergy (cross-reactivity possible) • Glyburide: generally NOT recommended in CKD — active metabolite accumulates → hypoglycemia • Pregnancy — insulin preferred • Severe hepatic impairment • Elderly / frail patients with irregular meals — high hypoglycemia risk • Combination with insulin — extreme hypoglycemia risk (reduce both doses) • ADA 2026: Fracture risk — avoid in patients with elevated fracture likelihood (TZDs and SUs)" NO → BLUE DOSING BOX (3 columns): "GLIPIZIDE (Glucotrol / Glucotrol XL) — With meals: IR: Start: 5 mg once daily (2.5 mg in elderly/liver disease) Titrate: +2.5-5 mg every several days MAX: 40 mg/day IR (doses >15 mg divide into 2 doses before meals) XL: Start: 5 mg once daily | MAX: 20 mg/day Frequency: IR 1-2x daily; XL once daily (with breakfast) CKD: PREFERRED sulfonylurea in CKD — initiate conservatively GLIMEPIRIDE (Amaryl) — With first meal of day: Start: 1-2 mg once daily Titrate: +1-2 mg every 1-2 weeks Maintenance: 1-4 mg once daily MAX: 8 mg/day Frequency: ONCE DAILY (with first meal) CKD: Start 1 mg/day; initiate conservatively; monitor closely CV: Shown CV-safe (CAROLINA trial vs linagliptin) GLYBURIDE (DiaBeta / Micronase) — With breakfast or first meal: Start: 2.5-5 mg once daily Titrate: +2.5 mg/week MAX: 20 mg/day (micronized: 12 mg/day) Frequency: 1-2x daily with meals CKD: GENERALLY NOT RECOMMENDED — active metabolite accumulates" TEAL INDICATIONS BOX: "INDICATIONS (ADA 2026) • T2DM glycemic management — HIGH efficacy (A1C reduction 1-2%) • Cost-effective option when affordability is a concern (lowest drug cost) • Glimepiride: CV-safe option (CAROLINA trial showed non-inferiority vs linagliptin) • Short-term glycemic coverage during illness/transitions • ADA 2026 NOTE: Limit/discontinue sulfonylureas when GLP-1 RA or SGLT2-i started — SUs provide no additional CV, kidney, weight, or liver benefit and increase hypoglycemia and weight gain risk" ORANGE ADVERSE EFFECTS BOX: "ADVERSE EFFECTS TO MONITOR • Hypoglycemia — YES (significant; most common serious adverse effect) • Weight gain — significant (1-4 kg) • FDA Special Warning: Increased CV mortality based on tolbutamide studies (older generation) • Glimepiride: shown CV-safe in CAROLINA trial • Avoid/reduce dose when combining with insulin • ADA 2026: Avoid in patients with elevated fracture risk (TZDs and SUs — increased fracture risk recommendation)" BOTTOM WIDE NAVY FOOTER BOX: "ADA 2026 KEY POSITION: DPP-4 inhibitors, sulfonylureas, and pioglitazone are second-line or adjunctive agents. When GLP-1 RA or SGLT2-i are initiated (preferred for CV/kidney/weight benefit), ADA 2026 recommends limiting or discontinuing DPP-4 inhibitors and sulfonylureas. Pioglitazone may be retained for MASH or insulin-sparing benefit. Glipizide or glimepiride are preferred over glyburide in CKD." White background, color-coded boxes (green=start, red=contraindication, yellow=decision/caution, orange=hold/adverse, blue=dosing, teal=indications, purple=monitoring, navy=footer), clear arrows, bold readable text, professional clinical layout. Very tall image to fit all three sections.
Do it again
A very large tall professional medical reference poster on white background with THREE stacked clinical flowcharts separated by thick colored divider lines. Color-coded boxes, clear arrows, bold headings, readable fonts throughout. Professional clinical style. ═══════════════════════════════════════ SECTION 1 — DPP-4 INHIBITORS ═══════════════════════════════════════ TITLE (large, dark blue bold, centered): "DPP-4 INHIBITORS (Oral) — ADA 2026" GREEN BOX: "START: Patient with T2DM — Consider DPP-4 Inhibitor" ↓ YELLOW DIAMOND: "Any Contraindication?" YES → RED BOX: "DO NOT USE: • Hypersensitivity to agent • Saxagliptin: avoid in Heart Failure (increased HF hospitalization risk) • Do NOT combine with GLP-1 RA (no added benefit) • Pancreatitis history: high caution • Severe hepatic impairment (alogliptin)" NO → YELLOW DIAMOND: "Check eGFR" → eGFR ≥45: GREEN box "Full dose all agents" → eGFR 30–44: YELLOW box "Sitagliptin 50 mg | Saxagliptin 2.5 mg | Alogliptin 12.5 mg | Linagliptin 5 mg (unchanged)" → eGFR <30 / Dialysis: ORANGE box "Sitagliptin 25 mg | Saxagliptin 2.5 mg (avoid HD) | Alogliptin 6.25 mg | Linagliptin 5 mg (PREFERRED — no adjustment)" All paths → BLUE BOX: "DOSING — Once Daily, With or Without Food (No Titration Required) • SITAGLIPTIN (Januvia): 100 mg once daily | MAX: 100 mg/day • SAXAGLIPTIN (Onglyza): 2.5–5 mg once daily | MAX: 5 mg/day | Avoid HF • LINAGLIPTIN (Tradjenta): 5 mg once daily | MAX: 5 mg/day | NO renal adjustment — preferred in CKD • ALOGLIPTIN (Nesina): 25 mg once daily | MAX: 25 mg/day" TEAL BOX: "INDICATIONS (ADA 2026) • T2DM add-on glycemic management (A1C ↓ ~0.7–1.0%) • No hypoglycemia risk as monotherapy — weight neutral • Preferred in frailty / older adults • Post-transplant mild hyperglycemia (NEW Rec 9.37, ADA 2026) • ADA 2026: Limit/discontinue when GLP-1 RA started — no added CV/kidney/weight benefit" PURPLE BOX: "ADVERSE EFFECTS • Pancreatitis: reported; discontinue if suspected • Joint pain (arthralgia): discontinue if debilitating • Bullous pemphigoid: discontinue if suspected — reversible • Saxagliptin: ↑ HF hospitalization — avoid in HF • Duration: Long-term as needed" THICK RED HORIZONTAL DIVIDER LINE ═══════════════════════════════════════ SECTION 2 — PIOGLITAZONE ═══════════════════════════════════════ TITLE (large dark teal bold, centered): "PIOGLITAZONE — Thiazolidinedione (Oral) — ADA 2026" GREEN BOX: "START: Patient with T2DM — Consider Pioglitazone" ↓ YELLOW DIAMOND: "Any Contraindication?" YES → RED BOX: "DO NOT USE: • Active Heart Failure (any class) — ↑ HF risk and fluid retention • Active bladder cancer — absolute contraindication • Prior bladder cancer — caution (higher cumulative dose/duration = higher risk) • Osteoporosis / high fracture risk — increased bone fracture risk • Severe hepatic impairment • Pregnancy • Significant edema / fluid overload • Kidney impairment — generally NOT recommended (fluid retention)" NO → BLUE BOX: "PIOGLITAZONE DOSING — Once Daily, With or Without Food • Start: 15–30 mg once daily • Titrate: Increase by 15 mg every 8–12 weeks based on response • Maintenance: 30–45 mg once daily • MAX: 45 mg/day • Frequency: ONCE DAILY • Renal: Generally NOT recommended in CKD — fluid retention risk • Duration: Long-term as tolerated; months needed to see full glycemic effect" TEAL BOX: "INDICATIONS (ADA 2026) • T2DM glycemic management — HIGH efficacy (A1C ↓ ~1–1.5%) • MASH / Biopsy-proven MASH or high liver fibrosis risk — Rec 9.13a (ADA 2026) • Adjunct to insulin — reduces insulin dose requirement • Cardiovascular: potential benefit (PROactive trial data) • Alternative when GLP-1 RA / SGLT2-i not available or not tolerated" ORANGE BOX: "ADVERSE EFFECTS TO MONITOR • Fluid retention / peripheral edema — dose-related • Weight gain — significant (2–4 kg) • Heart failure — increased risk; do NOT use in active HF • Bone fractures — increased risk (especially postmenopausal women) • Bladder cancer — avoid if active; caution with long-term high-dose use • Monitor LFTs before starting and periodically • ADA 2026: Avoid in elevated fracture risk patients (TZDs and SUs both flagged)" THICK DARK MAROON HORIZONTAL DIVIDER LINE ═══════════════════════════════════════ SECTION 3 — SULFONYLUREAS (2nd GENERATION) ═══════════════════════════════════════ TITLE (large dark maroon bold, centered): "SULFONYLUREAS — 2nd Generation (Oral) — ADA 2026" GREEN BOX: "START: Patient with T2DM — Consider Sulfonylurea" ↓ YELLOW DIAMOND: "Any Contraindication?" YES → RED BOX: "DO NOT USE / CAUTION: • Type 1 Diabetes or DKA • Sulfa drug allergy • Glyburide: GENERALLY NOT RECOMMENDED in CKD (active metabolite accumulates → hypoglycemia) • Pregnancy — use insulin instead • Severe hepatic impairment • Elderly / frail / irregular meals — high hypoglycemia risk • Combination with insulin: extreme hypoglycemia caution • ADA 2026: Avoid in patients with elevated fracture risk" NO → THREE-COLUMN BLUE BOX: "INDIVIDUAL AGENT DOSING (With Meals) GLIPIZIDE (Glucotrol): IR: Start 5 mg once daily before breakfast (2.5 mg elderly/liver) Titrate: +2.5–5 mg every few days MAX IR: 40 mg/day (divide doses >15 mg) XL: Start 5 mg once daily | MAX: 20 mg/day Frequency: IR 1–2x daily | XL once daily CKD: PREFERRED — initiate conservatively GLIMEPIRIDE (Amaryl): Start: 1–2 mg once daily with first meal Titrate: +1–2 mg every 1–2 weeks Maintenance: 1–4 mg once daily MAX: 8 mg/day Frequency: ONCE DAILY with first meal CKD: Start 1 mg; initiate conservatively CV: CAROLINA trial — proven CV safety vs linagliptin GLYBURIDE (DiaBeta): Start: 2.5–5 mg once daily with breakfast Titrate: +2.5 mg/week MAX: 20 mg/day (micronized: 12 mg/day) Frequency: 1–2x daily with meals CKD: GENERALLY NOT RECOMMENDED" TEAL BOX: "INDICATIONS (ADA 2026) • T2DM glycemic management — HIGH efficacy (A1C ↓ 1–2%) • Most cost-effective oral agent • Glimepiride: CV-safe (CAROLINA trial) • Short-term glycemic coverage during transitions or illness • ADA 2026: Limit/discontinue when GLP-1 RA or SGLT2-i started — no added CV/kidney/weight/liver benefit; increase hypoglycemia and weight gain risk" ORANGE BOX: "ADVERSE EFFECTS TO MONITOR • Hypoglycemia — YES (most significant risk; especially in elderly, renal impairment, combination with insulin) • Weight gain — significant (1–4 kg) • FDA Warning: Increased CV mortality with tolbutamide (older agent); glimepiride shown CV-safe • Bone fractures: ADA 2026 flags SUs and TZDs — avoid in elevated fracture risk • Reduce dose when adding insulin or GLP-1 RA (hypoglycemia risk)" FULL-WIDTH DARK NAVY FOOTER: "ADA 2026 POSITION: DPP-4 inhibitors, sulfonylureas, and pioglitazone are second-line / adjunctive agents. When GLP-1 RA or SGLT2-i are started, ADA 2026 recommends limiting or discontinuing DPP-4i and sulfonylureas (no additional CV/kidney/weight/liver benefit). Pioglitazone may be retained for MASH benefit or insulin-sparing. In CKD: linagliptin (no dose adjustment), glipizide or glimepiride preferred over glyburide." White background, color-coded (green=start, red=contraindication, yellow=caution/decision, orange=adverse/hold, blue=dosing, teal=indications, purple=monitoring, navy=footer). All text clearly readable. Very tall poster accommodating all three complete flowchart sections.
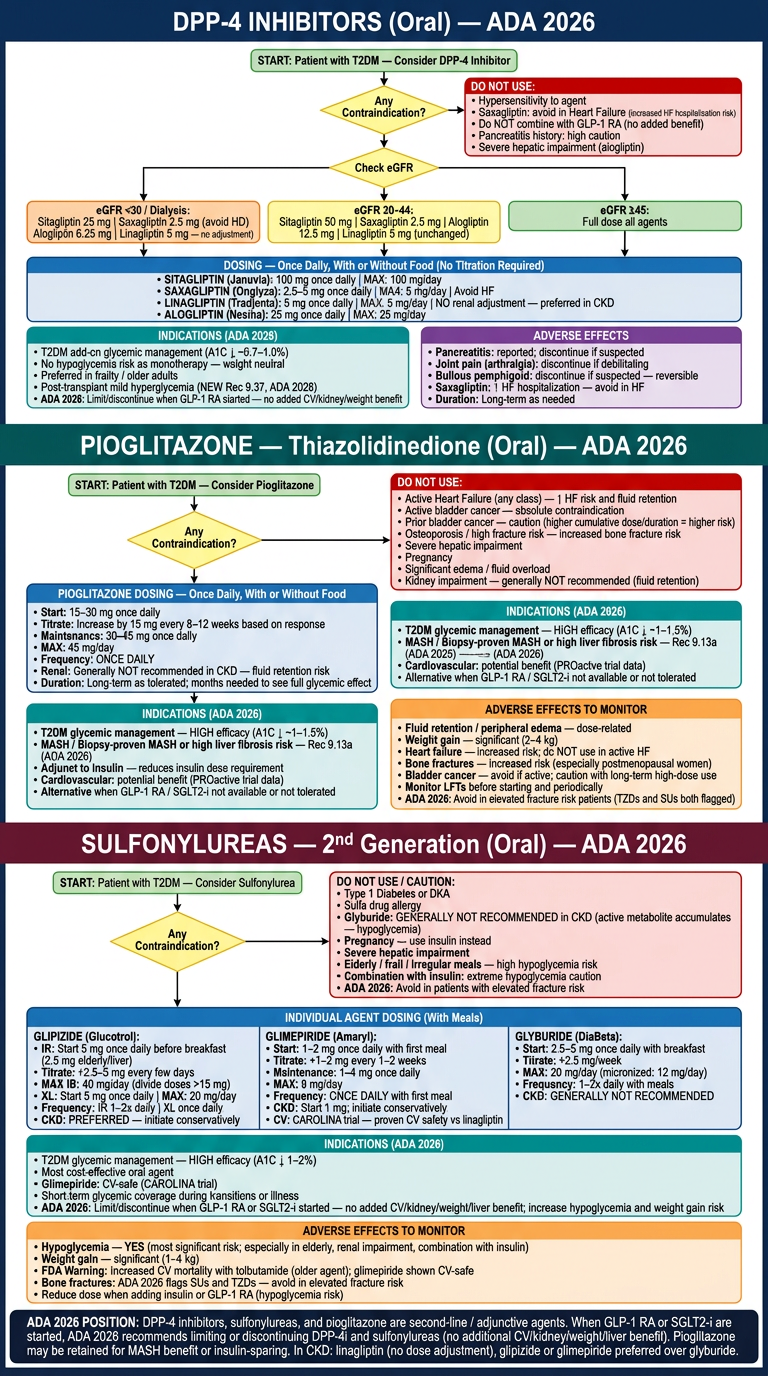
DPP-4 Inhibitors — Key Points
- No titration - all agents are fixed once-daily doses
- Linagliptin is the safest in CKD - no renal dose adjustment ever needed
- Sitagliptin, saxagliptin, alogliptin all require dose reductions as eGFR falls
- Saxagliptin: avoid in Heart Failure (increased HF hospitalization)
- A1C reduction ~0.7-1.0%; weight neutral; no hypoglycemia alone
Pioglitazone — Key Points
- Start 15-30 mg → titrate up → MAX 45 mg/day once daily
- ADA 2026 Rec 9.13a: option for biopsy-proven MASH
- Absolute contraindication: active bladder cancer, active HF
- Generally avoid in CKD - fluid retention risk
- Significant weight gain and edema; fracture risk in women
Sulfonylureas — Key Points
- Glipizide: preferred in CKD; MAX 40 mg/day IR
- Glimepiride: CV-safe (CAROLINA trial); MAX 8 mg/day; once daily
- Glyburide: avoid in CKD - metabolite accumulates
- Major risks: hypoglycemia + weight gain
- ADA 2026: discontinue when GLP-1 RA or SGLT2-i started
administration) Insulin (human) Glucose-lowering Hypoglycemia Progression of Kidney effects (SQ; regular efficacy' risk insulin also High to very high Yes Weight effects? Gain Effect on MACE Neutral Effect on HF Neutral Neutral CKD Dosing/use considerations* Lower insulin doses Clinical considerations and adverse available as required with a MASH effects effects inhaled decrease in eGFR; Unknown • Injection site reactions formulation) titrate per clinical Higher risk of hypoglycemia Insulin (analogs) response with human insulin (NPH or premixed formulations) vs. analogs (SQ) Risk of hypoglycemia and duration of activity increases with severity of impaired kidney function Refer to device-specific instructions for insulins compatible with different delivery systems (i.e., pumps, connected insulin pens, insulin patches). Give me dosage, how many times a day , titration, maximum dosages, how long and indication and contraindications from Ada 2026 guidelines for insulin make me a flowchart image like before
ADA 2026 insulin therapy dosage titration basal bolus types indication contraindication table 9.2 section 9
ADA 2026 insulin initiation basal insulin starting dose titration algorithm T2DM eGFR renal adjustment
http://saigaiin.sakura.ne.jp/sblo_files/saigaiin/image/DM20E…
A very large tall professional medical reference poster on white background titled "INSULIN THERAPY — ADA 2026 Clinical Flowchart". Multiple clearly color-coded sections with bold headings, clear arrows, readable text. Professional clinical style. TITLE (very large, dark blue bold, centered at top): "INSULIN THERAPY — ADA 2026 Clinical Flowchart" Subtitle: "(Human Insulin & Analogs — SQ; Regular also available inhaled)" ═══ TOP: INSULIN TYPES REFERENCE TABLE ═══ DARK NAVY HEADER BOX: "INSULIN TYPES & PHARMACOKINETICS" Four columns side by side: COLUMN 1 — BASAL INSULINS (Long/Intermediate-Acting) — DARK BLUE header: "LONG-ACTING ANALOGS (Preferred): • Insulin Glargine U-100 (Lantus): Onset 2-4h | Peak: Peakless | Duration: ~24h • Insulin Glargine U-300 (Toujeo): Onset 6h | Peak: Peakless | Duration: >24h • Insulin Detemir (Levemir): Onset 1-2h | Peak: Minimal | Duration: 16-24h • Insulin Degludec U-100/U-200 (Tresiba): Onset 1h | Peak: Peakless | Duration: >42h INTERMEDIATE-ACTING (Human): • NPH (Humulin N / Novolin N): Onset 2-4h | Peak: 4-10h | Duration: 10-18h" COLUMN 2 — PRANDIAL / BOLUS INSULINS (Short/Rapid-Acting) — TEAL header: "RAPID-ACTING ANALOGS (Preferred): • Insulin Lispro (Humalog): Onset 15-30min | Peak: 30-90min | Duration: 3-5h • Insulin Aspart (NovoLog): Onset 10-20min | Peak: 40-50min | Duration: 3-5h • Insulin Glulisine (Apidra): Onset 10-15min | Peak: 30-90min | Duration: 3-5h • Ultra-Rapid: Faster Aspart (Fiasp), Lispro-aabc (Lyumjev): Onset <5min SHORT-ACTING (Human): • Regular insulin (Humulin R / Novolin R): Onset 30-60min | Peak: 2-4h | Duration: 5-8h Also available as INHALED (Afrezza): Onset 12-15min | Peak: 30min | Duration: 2-3h" COLUMN 3 — PREMIXED INSULINS — PURPLE header: "PREMIXED (Human & Analog): • NPH/Regular 70/30: 70% NPH + 30% Regular • Lispro 75/25 (Humalog Mix): 75% protamine + 25% lispro • Aspart 70/30 (NovoLog Mix): 70% protamine + 30% aspart • Use: Twice daily with meals (fixed ratio) • Limitation: Less flexibility; Higher hypoglycemia risk vs analogs" COLUMN 4 — CONCENTRATED INSULINS — ORANGE header: "CONCENTRATED: • Regular U-500 (Humulin R U-500): Severe insulin resistance; 5x concentration • Glargine U-300 (Toujeo): 3x concentration; longer duration • Degludec U-200 (Tresiba): 2x concentration Refer to device-specific instructions for pumps, connected pens, insulin patches (ADA 2026)" ═══ SECTION 2: INITIATION FLOWCHART ═══ GREEN BOX: "INDICATION TO START INSULIN" Split into two paths: LEFT PATH — TYPE 1 DIABETES: "T1DM — Insulin is MANDATORY (not optional) • Newly diagnosed T1DM: 0.2–0.6 units/kg/day total daily dose (TDD) • Divide: ~50% as BASAL + ~50% as PRANDIAL (at meals) • Honeymoon phase: lower doses may suffice • AID (Automated Insulin Delivery) systems: offer to ALL adults with T1DM (ADA 2026)" RIGHT PATH — TYPE 2 DIABETES: "T2DM — Consider insulin when: • A1C >10% OR blood glucose ≥300 mg/dL with symptoms • Failure of 2-3 oral/injectable agents • Symptomatic hyperglycemia • Pregnancy with inadequate glycemic control • Cancer treatment, surgery, critical illness, steroids" Both paths merge → YELLOW DIAMOND: "Which Insulin Regimen?" Four regimen paths: PATH A — GREEN: "BASAL INSULIN ALONE (Start here for most T2DM) Start: 10 units/day OR 0.1–0.2 units/kg/day SC at bedtime or same time each day Titrate: Increase by 2 units every 3 days until fasting glucose reaches target (80–130 mg/dL) OR increase 10–15% every 3 days Preferred agents: Glargine U-100, Detemir, Degludec (analogs preferred over NPH) Continue oral agents (especially metformin, SGLT2-i, GLP-1 RA) Stop: Sulfonylureas, meglitinides, DPP-4i when adding insulin" PATH B — TEAL: "BASAL + PRANDIAL (Basal-Bolus) — For T1DM or T2DM needing intensification Prandial initiation: Add 4 units/day OR 10% of basal dose with largest meal Titrate: Increase by 1–2 units or 10–15% every 3 days to reach PPG target (<180 mg/dL) Reduce basal by 4 units/day or 10% when adding prandial Stepwise: Add 1 prandial dose → 2 → 3 (full basal-bolus) T1DM TDD: 0.4–0.7 units/kg/day (higher in insulin resistance)" PATH C — PURPLE: "PREMIXED TWICE DAILY — Alternative for some T2DM Start: Unit-for-unit conversion from basal at same TDD 2/3 dose before breakfast | 1/3 dose before dinner Titrate: Adjust each component based on fasting and PPG Limitation: Less flexible; higher hypoglycemia risk" PATH D — ORANGE: "SELF-MIXED / SPLIT (NPH + Short/Rapid) 2/3 before breakfast | 1/3 before dinner Add 4 units or 10% of NPH dose as short/rapid with each injection Titrate each component individually" ═══ SECTION 3: TITRATION & MONITORING ═══ BLUE BOX: "TITRATION PRINCIPLES (ADA 2026) • Uptitrate or downtitrate at EVERY VISIT based on: A1C, CGM data, SMBG (fasting & postprandial) • Assess insulin dose adequacy and insulin-taking behaviors at every visit • Hypoglycemia: Determine cause; if no clear reason → lower dose by 10–20% • Overbasalization warning signs: bedtime-to-morning glucose differential ≥50 mg/dL, hypoglycemia (aware or unaware), high glucose variability • If overbasalized: consider adding prandial insulin rather than increasing basal further • CGM: Recommended for ALL patients on insulin (ADA 2026) — offer at diabetes onset and at any time • AID systems: Offer to ALL adults with T2DM on insulin (NEW ADA 2026)" ═══ SECTION 4: RENAL CONSIDERATIONS ═══ YELLOW/ORANGE BOX: "RENAL / KIDNEY DOSING (ADA 2026) • Lower insulin doses required as eGFR decreases • Titrate per clinical response — no fixed dose reduction formula • Risk of hypoglycemia INCREASES with severity of CKD (reduced insulin clearance) • Analogs preferred over human insulin (NPH/premixed) — lower hypoglycemia risk • Monitor glucose more frequently in CKD • Prefer analogs: glargine, detemir, degludec over NPH in renal impairment" ═══ SECTION 5: CONTRAINDICATIONS & CAUTIONS ═══ RED BOX: "CONTRAINDICATIONS / CAUTIONS • Hypoglycemia unawareness — use CGM/AID; reduce dose; use analogs • Insulin allergy (rare) — may require desensitization or switch formulation • Severe lipohypertrophy at injection sites — rotate sites • Do NOT use U-500 concentrated insulin in standard insulin syringes (dosing error risk) • Inhaled insulin (Afrezza): contraindicated in asthma, COPD, active lung disease • Premixed insulins: avoid in patients requiring flexible dosing (illness, variable meals)" ═══ SECTION 6: INDICATIONS SUMMARY ═══ TEAL BOX: "INDICATIONS (ADA 2026) TYPE 1 DIABETES: Absolute requirement — all patients TYPE 2 DIABETES: • Failure to meet glycemic targets on oral/injectable agents • A1C >10% or BG ≥300 mg/dL with symptoms • Gestational diabetes / pregnancy with inadequate control • Hospitalization, surgery, critical illness • Cancer therapy-induced severe hyperglycemia (Rec 9.33–9.36) • Immunotherapy-associated diabetes (assess for insulin need — NEW ADA 2026 Rec 9.33) • Continue metformin + SGLT2-i + GLP-1 RA when starting insulin (ADA 2026 Rec 9.23)" ═══ SECTION 7: ADVERSE EFFECTS ═══ PURPLE BOX: "ADVERSE EFFECTS TO MONITOR • Hypoglycemia — most significant; higher with human insulin (NPH/premixed) vs analogs; higher in CKD • Weight gain — significant; mitigate with GLP-1 RA combination • Injection site reactions — lipohypertrophy, lipoatrophy; rotate sites • Edema — early insulin therapy • Vision changes — transient with rapid glucose correction • Duration: Lifelong in T1DM; long-term / indefinite in T2DM as needed" DARK NAVY FOOTER: "ADA 2026 KEY POINTS: (1) Analogs preferred over human insulin — less hypoglycemia risk. (2) Continue metformin, SGLT2-i, GLP-1 RA when initiating insulin. (3) Stop sulfonylureas, meglitinides, DPP-4i. (4) Offer AID systems to ALL adults with T1DM and T2DM on insulin. (5) CGM recommended at diabetes onset for all on insulin. (6) Reassess insulin doses when adding/escalating GLP-1 RA or dual GIP/GLP-1 RA." White background, professional medical poster, color-coded sections clearly separated, bold headers, all text clearly readable, large enough to show all detail. Very tall image.
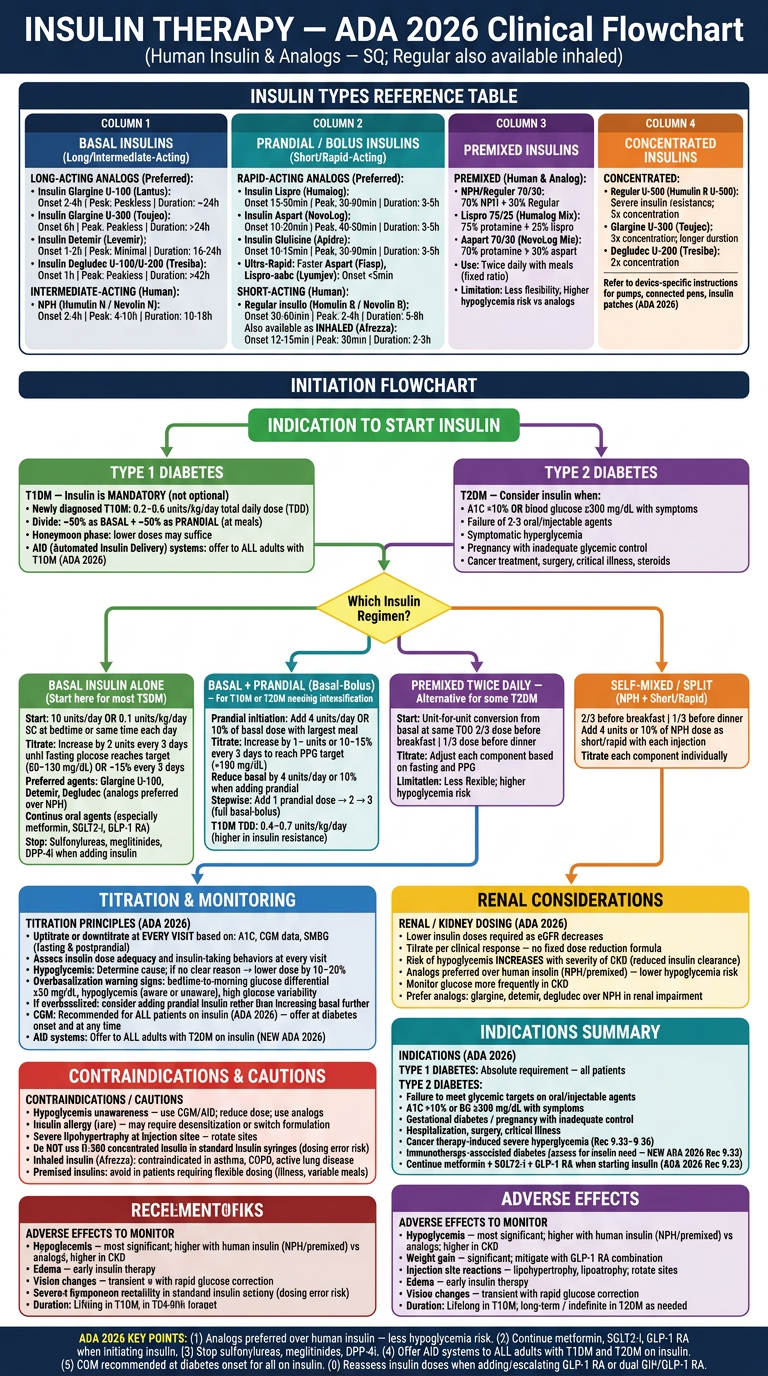
Insulin Therapy — ADA 2026 Complete Reference
Insulin Types
| Class | Agent | Onset | Peak | Duration | Frequency |
|---|---|---|---|---|---|
| Long-acting analog | Glargine U-100 (Lantus) | 2-4h | Peakless | ~24h | Once daily |
| Glargine U-300 (Toujeo) | 6h | Peakless | >24h | Once daily | |
| Detemir (Levemir) | 1-2h | Minimal | 16-24h | Once or twice daily | |
| Degludec U-100/200 (Tresiba) | 1h | Peakless | >42h | Once daily | |
| Intermediate (human) | NPH (Humulin N) | 2-4h | 4-10h | 10-18h | 1-2x daily |
| Rapid-acting analog | Lispro (Humalog) | 15-30 min | 30-90 min | 3-5h | Before each meal |
| Aspart (NovoLog) | 10-20 min | 40-50 min | 3-5h | Before each meal | |
| Glulisine (Apidra) | 10-15 min | 30-90 min | 3-5h | Before each meal | |
| Ultra-rapid | Faster Aspart (Fiasp) | <5 min | ~1h | 3-5h | With each meal |
| Short-acting (human) | Regular (Humulin R) | 30-60 min | 2-4h | 5-8h | 30 min before meals |
| Inhaled | Afrezza | 12-15 min | ~30 min | 2-3h | Before each meal |
| Premixed | NPH/Regular 70/30 | Combined | Combined | Combined | Twice daily |
| Concentrated | Regular U-500 | 30-60 min | 2-5h | Up to 24h | 2-3x daily |
Indications (ADA 2026)
| Indication | Notes |
|---|---|
| Type 1 Diabetes | Absolute requirement - all patients, lifelong |
| T2DM: A1C >10% or BG ≥300 mg/dL with symptoms | Start insulin regardless of background therapy |
| T2DM: failure of oral/injectable agents | After 2-3 agent failure to meet glycemic targets |
| Pregnancy / GDM inadequately controlled | Insulin preferred first-line |
| Hospitalization, surgery, critical illness | Insulin is primary agent |
| Immunotherapy-associated diabetes (NEW Rec 9.33) | Assess insulin need to prevent DKA |
| Cancer therapy severe hyperglycemia (Rec 9.33-9.36) | Insulin for severe hyperglycemia / crises |
| Steroid-induced hyperglycemia | Insulin if severe or uncontrolled |
Dosing & Titration
T1DM — Starting Dose
- Total Daily Dose (TDD): 0.2-0.6 units/kg/day at initiation (lower in honeymoon phase)
- Split: ~50% basal + ~50% prandial (divided among meals)
- Typical maintenance: 0.4-0.7 units/kg/day
T2DM — Basal Insulin (Start Here)
| Phase | Dose |
|---|---|
| Start | 10 units/day OR 0.1-0.2 units/kg/day SC |
| Timing | Bedtime or same time daily |
| Titrate | Increase by 2 units every 3 days until FPG 80-130 mg/dL |
| Alternative titration | Increase 10-15% every 3 days |
| Preferred agents | Glargine, Detemir, Degludec (analogs > NPH) |
| Maximum | No fixed maximum - titrate to glycemic target |
Adding Prandial Insulin (when basal insufficient)
| Phase | Dose |
|---|---|
| Start | 4 units/day OR 10% of basal dose with the largest meal |
| Reduce basal | Lower basal by 4 units or 10% when adding prandial |
| Titrate prandial | Increase 1-2 units or 10-15% every 3 days to PPG target <180 mg/dL |
| Stepwise | Add 1 meal dose → 2 meals → full basal-bolus (3 meals) |
| For hypoglycemia | Lower offending dose by 10-20%; determine cause |
| Frequency | Before each meal (rapid-acting); 30 min before (regular) |
Renal Dosing (ADA 2026)
- Lower insulin doses required as eGFR decreases - reduced renal clearance prolongs insulin action
- Titrate per clinical response - no fixed formula
- Hypoglycemia risk increases with CKD severity
- Analogs preferred over human insulin (NPH/premixed) in renal impairment - lower hypoglycemia risk
- Monitor glucose more frequently in CKD
Overbasalization — ADA 2026 Warning Signs
- Bedtime-to-morning glucose differential ≥50 mg/dL
- Hypoglycemia (aware or unaware)
- High glucose variability
- Action: Add prandial insulin rather than continuing to increase basal
Contraindications / Cautions
| Issue | Action |
|---|---|
| Hypoglycemia unawareness | Use CGM/AID; reduce dose; switch to analogs |
| Insulin allergy | Rare; switch formulation; desensitize if needed |
| Lipohypertrophy | Rotate injection sites systematically |
| Inhaled insulin (Afrezza) | Contraindicated in asthma, COPD, active lung disease |
| U-500 concentrated | Do not use standard syringes - dedicated pen/syringe only |
| Premixed insulin | Avoid when flexible dosing needed (illness, variable meals) |
ADA 2026 Key Insulin Rules
- Continue metformin, SGLT2-i, GLP-1 RA when starting insulin (Rec 9.23)
- Stop sulfonylureas, meglitinides, DPP-4 inhibitors when starting insulin
- Offer AID systems to ALL adults with T1DM and T2DM on insulin (NEW 2026)
- CGM recommended at diabetes onset for all on insulin (Rec 9.25)
- Reassess insulin doses when adding or escalating GLP-1 RA or tirzepatide
- Analogs preferred over human insulin - lower hypoglycemia risk, especially in CKD
- Duration: Lifelong in T1DM; long-term/indefinite in T2DM as clinically required
Can you make it in horizontal
A very wide horizontal landscape medical reference flowchart poster on white background titled "INSULIN THERAPY — ADA 2026 Clinical Flowchart". Flow goes LEFT to RIGHT across the full width. Color-coded boxes, clear horizontal arrows, bold readable text, professional clinical style. TITLE (large dark blue bold, top center): "INSULIN THERAPY — ADA 2026 Clinical Flowchart" Subtitle (smaller): "Human Insulin & Analogs — SQ | Regular also available Inhaled (Afrezza)" ══════════════════════════════════════════════════════════ TOP ROW — INSULIN TYPES REFERENCE BAR (spans full width) ══════════════════════════════════════════════════════════ Five side-by-side colored boxes across the top: BOX 1 — DARK BLUE: "BASAL — Long-Acting Analogs (PREFERRED) • Glargine U-100 (Lantus): ~24h, peakless, once daily • Glargine U-300 (Toujeo): >24h, peakless, once daily • Detemir (Levemir): 16-24h, once or twice daily • Degludec (Tresiba): >42h, peakless, once daily" BOX 2 — STEEL BLUE: "BASAL — Intermediate (Human) • NPH (Humulin N): Onset 2-4h | Peak 4-10h | Duration 10-18h • 1-2x daily • Higher hypoglycemia risk vs analogs" BOX 3 — TEAL: "PRANDIAL — Rapid-Acting Analogs (PREFERRED) • Lispro (Humalog): onset 15-30 min • Aspart (NovoLog): onset 10-20 min • Glulisine (Apidra): onset 10-15 min • Faster Aspart (Fiasp) / Lispro-aabc (Lyumjev): <5 min • Duration 3-5h | Given before each meal" BOX 4 — GREEN: "PRANDIAL — Short-Acting (Human) • Regular (Humulin R / Novolin R) • Onset 30-60 min | Peak 2-4h | Duration 5-8h • Give 30 min BEFORE meals • Also available INHALED (Afrezza): onset 12-15 min" BOX 5 — PURPLE: "PREMIXED & CONCENTRATED • NPH/Regular 70/30 — twice daily with meals • Lispro 75/25, Aspart 70/30 — twice daily • U-500 Regular: severe insulin resistance only • Glargine U-300, Degludec U-200: concentrated basal • Use device-specific instructions (pumps, pens, patches)" ══════════════════════════════════════════════════════════ MAIN FLOWCHART — LEFT TO RIGHT HORIZONTAL FLOW ══════════════════════════════════════════════════════════ STEP 1 — GREEN START BOX (far left): "INDICATION FOR INSULIN T1DM: Mandatory — all patients T2DM: Consider when: • A1C >10% or BG ≥300 mg/dL + symptoms • Failure of oral/injectable agents • Pregnancy / GDM uncontrolled • Surgery, critical illness, hospitalization • Immunotherapy diabetes (NEW Rec 9.33) • Cancer drug hyperglycemia (Rec 9.33-9.36)" → RIGHT ARROW → STEP 2 — YELLOW DIAMOND: "T1DM or T2DM?" → T1DM arrow UP-RIGHT → BLUE BOX: "T1DM DOSING TDD: 0.2–0.6 units/kg/day 50% BASAL + 50% PRANDIAL Maintenance: 0.4–0.7 units/kg/day AID systems: Offer to ALL T1DM adults (ADA 2026) CGM: Recommended at diagnosis" → T2DM arrow DOWN-RIGHT → ORANGE BOX: "T2DM — START BASAL INSULIN Start: 10 units/day OR 0.1–0.2 units/kg/day SC Timing: Bedtime or same time daily Preferred: Glargine, Detemir, Degludec (analogs) Continue: Metformin + SGLT2-i + GLP-1 RA STOP: Sulfonylureas, Meglitinides, DPP-4i" → RIGHT ARROW (from both paths) → STEP 3 — BLUE BOX: "BASAL TITRATION ALGORITHM Increase by 2 units every 3 days OR 10–15% every 3 days Target FPG: 80–130 mg/dL Assess at EVERY visit: • CGM data / SMBG readings • Hypoglycemia episodes • Insulin-taking behaviors ↓ Hypoglycemia: Reduce 10–20%" → RIGHT ARROW → STEP 4 — YELLOW DIAMOND: "Basal Adequate? FPG at target but A1C still high / PPG elevated?" → YES (still above target) → TEAL BOX: "ADD PRANDIAL INSULIN Start: 4 units/day OR 10% of basal dose Give with LARGEST meal first Reduce basal by 4 units or 10% simultaneously Titrate: +1–2 units or 10–15% every 3 days PPG target: <180 mg/dL Step up: 1 meal → 2 meals → Full Basal-Bolus (3 meals) Preferred: Rapid-acting analogs over Regular" → RIGHT ARROW → STEP 5 — DARK BLUE BOX: "FULL BASAL-BOLUS or AID T1DM: Full MDI (Multiple Daily Injections) or AID T2DM: Basal-bolus if targets not met AID (Automated Insulin Delivery): Offer to ALL T1DM adults Offer to ALL T2DM adults on insulin (NEW ADA 2026) Reassess doses when adding/escalating GLP-1 RA or tirzepatide" → RIGHT ARROW → STEP 6 — PURPLE BOX: "ONGOING MONITORING & TITRATION Uptitrate OR downtitrate at every visit OVERBASALIZATION — Check if: • Bedtime-to-morning glucose ≥50 mg/dL • Hypoglycemia (aware or unaware) • High glucose variability Action: Add prandial rather than ↑ basal further CGM: All patients on insulin (Rec 9.25) Assess need for AID, pump, connected pen" ══════════════════════════════════════════════════════════ BOTTOM ROW — Three boxes spanning full width ══════════════════════════════════════════════════════════ BOTTOM LEFT — RED BOX: "CONTRAINDICATIONS / CAUTIONS • Inhaled insulin (Afrezza): contraindicated in asthma, COPD, active lung disease • U-500: do NOT use standard syringes — dedicated device only • Premixed: avoid when flexible dosing needed (illness, variable meals) • Allergy to insulin: rare — switch formulation • Lipohypertrophy: rotate injection sites — impairs absorption" BOTTOM MIDDLE — ORANGE BOX: "RENAL CONSIDERATIONS (ADA 2026) • Lower insulin doses required as eGFR decreases • Titrate per clinical response — no fixed formula • Hypoglycemia risk INCREASES with CKD severity • Analogs preferred over NPH/premixed in CKD • Monitor glucose more frequently in CKD • Insulin remains safe at any eGFR level (unlike other agents)" BOTTOM RIGHT — DARK NAVY BOX: "ADA 2026 KEY RULES 1. Continue metformin + SGLT2-i + GLP-1 RA when starting insulin (Rec 9.23) 2. STOP sulfonylureas, meglitinides, DPP-4i with insulin 3. Analogs PREFERRED over human insulin (less hypoglycemia) 4. Offer AID to ALL adults with T1DM and T2DM on insulin (NEW 2026) 5. CGM at diagnosis for all on insulin (Rec 9.25) 6. Reassess insulin doses when GLP-1 RA added/escalated 7. Duration: Lifelong T1DM | Long-term T2DM as needed ADVERSE EFFECTS: Hypoglycemia • Weight gain • Injection site reactions • Edema (early)" Wide landscape orientation, white background, left-to-right flow with clear horizontal arrows between steps, color-coded boxes, bold section titles, all text readable. Make it very wide to accommodate the horizontal layout.
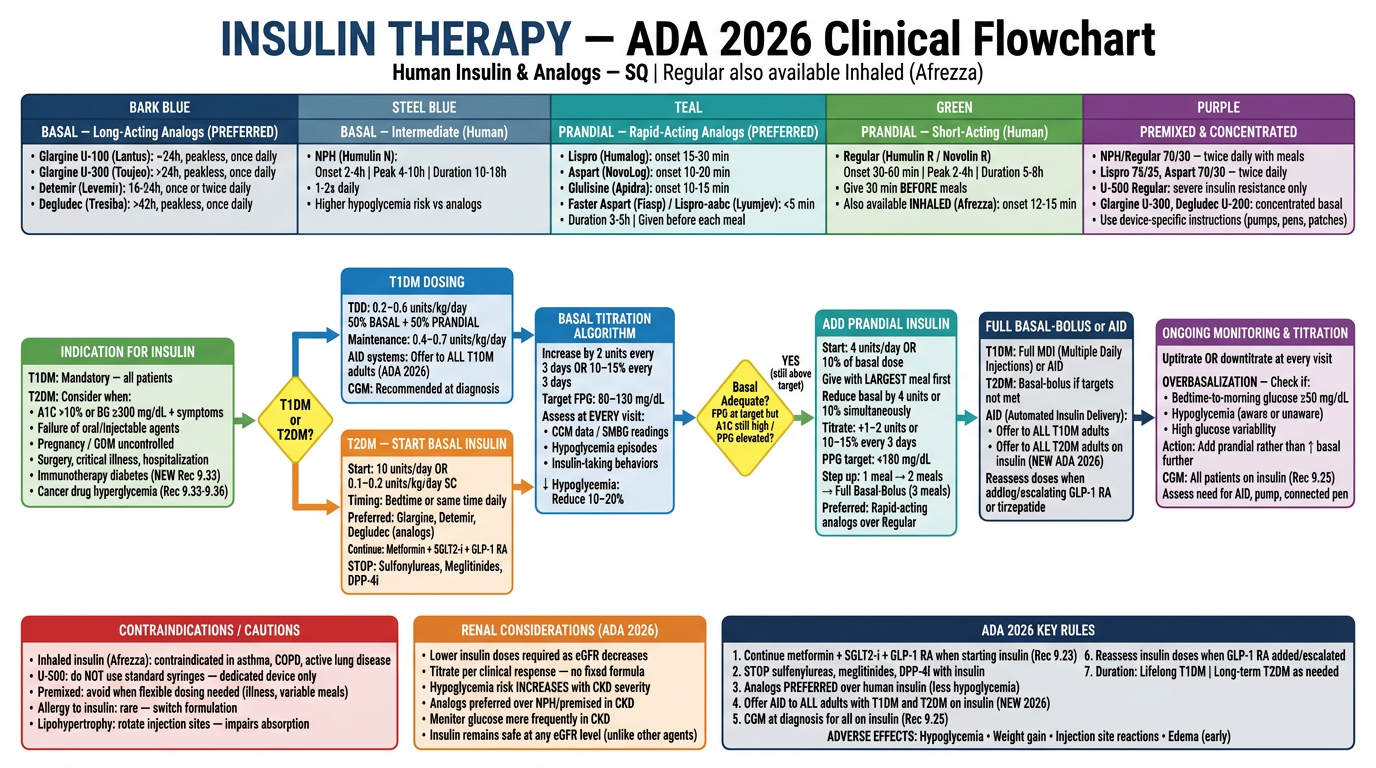
-
Insulin Types bar across the top - all 5 categories at a glance (long-acting analogs, NPH, rapid-acting analogs, regular/inhaled, premixed/concentrated)
-
Main flow: Indication → T1DM vs T2DM split → Basal initiation → Titration algorithm → Adding prandial → Full basal-bolus / AID → Ongoing monitoring
-
Bottom row: Contraindications | Renal considerations | ADA 2026 key rules

Explain this
📋 Explanation: DPP-4 Inhibitors, Pioglitazone & Sulfonylureas — ADA 2026
SECTION 1: DPP-4 INHIBITORS (Oral)
What are they?
How to use the flowchart:
- Hypersensitivity to the specific agent
- Saxagliptin in heart failure - this agent specifically was shown to increase HF hospitalization in the SAVOR-TIMI trial, so avoid it in HF patients
- Never combine a DPP-4 inhibitor with a GLP-1 RA - they work on the same pathway so there is no added benefit, only added cost and side effects
- Pancreatitis history - use high caution
- Severe hepatic impairment (especially alogliptin)
| eGFR | Action |
|---|---|
| ≥45 | Full dose for all agents |
| 20-44 | Sitagliptin 50 mg, Saxagliptin 2.5 mg, Alogliptin 12.5 mg, Linagliptin unchanged |
| <30 / Dialysis | Sitagliptin 25 mg, Saxagliptin 2.5 mg (avoid in hemodialysis), Alogliptin 6.25 mg, Linagliptin unchanged |
Key clinical pearl: Linagliptin is the only DPP-4 inhibitor that does NOT need any dose adjustment in kidney disease - it is excreted via bile, not the kidneys. This makes it the preferred DPP-4 inhibitor in CKD patients.
- Sitagliptin (Januvia): 100 mg once daily
- Saxagliptin (Onglyza): 2.5-5 mg once daily
- Linagliptin (Tradjenta): 5 mg once daily
- Alogliptin (Nesina): 25 mg once daily
- Add-on therapy for T2DM (reduces A1C by ~0.7-1.0%)
- Weight neutral with no hypoglycemia - useful in elderly and frail patients
- Post-transplant mild hyperglycemia (new ADA 2026 Rec 9.37)
- ADA 2026 says: limit or discontinue DPP-4i when you start a GLP-1 RA - no added CV, kidney, or weight benefit
- Pancreatitis (rare but reported - stop if suspected)
- Joint pain (arthralgia) - stop if debilitating
- Bullous pemphigoid (skin blistering) - stop, reverses on discontinuation
- Saxagliptin: increased HF hospitalization - avoid in heart failure patients
SECTION 2: PIOGLITAZONE — Thiazolidinedione (TZD)
What is it?
How to use the flowchart:
- Active Heart Failure (any NYHA class) - pioglitazone causes fluid retention and can precipitate or worsen HF
- Active bladder cancer - absolute contraindication
- Prior bladder cancer - use with caution; risk increases with longer use and higher cumulative doses
- Osteoporosis / high fracture risk - pioglitazone increases bone fracture risk, especially in postmenopausal women
- Severe hepatic impairment, pregnancy, significant edema
- Kidney impairment - generally not recommended due to fluid retention risk
- Start: 15-30 mg once daily (any time, with or without food)
- Titrate: increase by 15 mg every 8-12 weeks
- Maintenance: 30-45 mg once daily
- Maximum: 45 mg/day
- Takes weeks to months to reach full glycemic effect - this is a slow-acting drug
- T2DM glycemic management - HIGH efficacy (A1C reduction ~1-1.5%)
- MASH/biopsy-proven MASH (metabolic liver disease with steatohepatitis) - ADA 2026 Rec 9.13a: pioglitazone is one of the options for patients with T2DM and biopsy-proven MASH or high risk for liver fibrosis
- Adjunct to insulin - reduces how much insulin is needed
- Some cardiovascular benefit from the PROactive trial
- Fluid retention and edema - most significant clinical concern
- Weight gain (2-4 kg)
- Heart failure risk - do NOT use in active HF
- Bone fractures - especially women
- Bladder cancer - monitor for symptoms with long-term use
- Monitor liver function tests (LFTs) before starting and periodically
SECTION 3: SULFONYLUREAS — 2nd Generation
What are they?
How to use the flowchart:
- Type 1 Diabetes or DKA - never use (pancreatic beta cells are destroyed in T1DM)
- Sulfa drug allergy - possible cross-reactivity
- Glyburide in CKD: generally NOT recommended - its active metabolite accumulates in renal impairment causing prolonged, dangerous hypoglycemia
- Pregnancy (use insulin instead)
- Elderly/frail patients with irregular meals - very high hypoglycemia risk
- Combination with insulin - extreme hypoglycemia caution; reduce both doses
- ADA 2026 specifically flags: avoid in patients with elevated fracture risk (both TZDs and sulfonylureas increase fracture risk)
- IR: Start 5 mg once daily before breakfast (2.5 mg in elderly)
- Titrate: +2.5-5 mg every few days
- MAX IR: 40 mg/day (divide doses >15 mg into twice daily)
- XL formulation: Start 5 mg once daily, MAX 20 mg/day
- Frequency: IR 1-2x daily; XL once daily
- Start: 1-2 mg once daily with first meal of the day
- Titrate: +1-2 mg every 1-2 weeks
- Maintenance: 1-4 mg once daily
- MAX: 8 mg/day
- In CKD: start at 1 mg, titrate conservatively
- CAROLINA trial showed CV safety (non-inferior to linagliptin) - the most CV-evidence-backed sulfonylurea
- Start: 2.5-5 mg once daily with breakfast
- Titrate: +2.5 mg/week
- MAX: 20 mg/day (micronized form: 12 mg/day)
- Frequency: 1-2x daily
- Generally NOT recommended in CKD - active metabolite accumulates
- T2DM glycemic management - HIGH efficacy (A1C reduction 1-2%)
- Most cost-effective oral diabetes agent - important for affordability
- Glimepiride: CV-safe per CAROLINA trial
- Short-term glycemic coverage during illness or transitions
- ADA 2026 key message: limit or discontinue sulfonylureas when starting GLP-1 RA or SGLT2-i - sulfonylureas provide no CV, kidney, weight, or liver benefit, and they add hypoglycemia and weight gain risks
- Hypoglycemia - most significant risk, especially in elderly, CKD, and with insulin combination
- Weight gain (1-4 kg)
- FDA Warning: Increased CV mortality with tolbutamide (older, 1st-generation agent); glimepiride shown safe
- Bone fractures - ADA 2026 flags both TZDs and sulfonylureas: avoid in patients at elevated fracture risk
- Always reduce dose when adding insulin or a GLP-1 RA (hypoglycemia risk increases)
BOTTOM FOOTER — ADA 2026 Overall Position
DPP-4 inhibitors, sulfonylureas, and pioglitazone are second-line or adjunctive agents.
- Limit or stop DPP-4 inhibitors (no added CV/kidney/weight benefit)
- Limit or stop sulfonylureas (increase hypoglycemia and weight gain without organ-protective benefit)
- Pioglitazone may be kept if the patient has MASH or needs insulin-sparing
- Linagliptin = preferred DPP-4i (no dose adjustment)
- Glipizide or glimepiride = preferred sulfonylureas (glipizide most preferred)
- Glyburide = avoid