A 60 yr old woman a k ken case of SLE, not on treatmenf for past 6yrs came with early morning stiffness and pain, swelling hand small joints for 2 weeks,
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Searching PubMed
SLE arthritis flare management hydroxychloroquine
Loading Image
Here is a structured clinical approach to this case:
60-Year-Old Woman with Known SLE - Off Treatment 6 Years - Presenting with Polyarthritis
Clinical Problem Summary
A woman with established SLE, off all treatment for 6 years, presents with 2 weeks of early morning stiffness (EMS), pain, and swelling of the small joints of both hands. This is a SLE flare until proven otherwise, but several important differentials must be considered.
Step 1: Differential Diagnosis
Most Likely: SLE Arthritis Flare
- SLE arthritis is typically a symmetric polyarthritis involving the wrists, MCPs, and PIPs - exactly the pattern described here.
- EMS is a classic feature of inflammatory arthritis.
- Being off treatment for 6 years significantly increases flare risk.
- Key feature: SLE arthritis is classically non-erosive and non-deforming, though in some patients periarticular ligament damage may lead to Jaccoud-like deformity (reducible subluxations, distinct from RA).
- Harrison's (2025): "Lupus arthritis is characterized by a polyarthritis most commonly involving the wrists, the MCP and PIP joints of the hands, and the knees."
Important Differential: Rhupus (SLE + RA Overlap)
- RA and SLE can occur simultaneously - this overlap is termed "Rhupus".
- Features that would favor Rhupus over pure SLE arthritis: erosive changes on X-ray/MRI, RF/anti-CCP positivity, more deforming arthritis, nodules.
- Emerging MRI/ultrasound studies suggest SLE can occasionally show erosive changes, but less severe than RA.
Other Differentials to Exclude
| Condition | Distinguishing Features |
|---|---|
| Infectious arthritis | Fever, monoarthritis more common, culture positivity |
| Viral arthritis (Parvovirus B19, Chikungunya) | Recent viral illness, self-limiting |
| Drug-induced lupus | History of offending drug (not relevant here - off meds) |
| Osteoarthritis (OA) | DIP involvement, bony swelling, less EMS |
| Psoriatic arthritis | Skin/nail changes, DIP involvement, asymmetric |
| Crystal arthropathy (Gout/CPPD) | Asymmetric, acute episodic, crystal on aspiration |
| Sjögren's syndrome overlap | Dry eyes/mouth, anti-Ro/La antibodies |
| Avascular necrosis (AVN) | Single large joint (hip, shoulder, knee), pain out of proportion - if prior steroid use |
Step 2: Key History to Take
- Duration and pattern of joint involvement (additive vs. migratory)
- Any other SLE features currently: rash, photosensitivity, oral ulcers, hair loss, chest pain/breathlessness (serositis), hematuria, frothy urine (nephritis), neurological symptoms
- Why treatment was stopped 6 years ago (side effects? remission? non-compliance?)
- Prior medications (especially steroids - raises AVN risk)
- Family history of RA
- Signs of infection (fever, recent illness)
- Menstrual/hormonal history (menopause - post-menopausal women can flare)
Step 3: Investigations
Immediate / Baseline
| Investigation | Rationale |
|---|---|
| CBC with differential | Cytopenias (leukopenia, thrombocytopenia, hemolytic anemia) - markers of SLE activity |
| ESR and CRP | Elevated in inflammation; CRP is usually disproportionately low in SLE flare (unless infection or serositis) |
| Serum creatinine and eGFR | Screen for lupus nephritis |
| Urine routine + microscopy | Proteinuria, hematuria, casts = nephritis (screen every 3 months per EULAR) |
| Spot urine protein:creatinine ratio (UPCr) | If UPCr >0.5 suggests nephritis, consider biopsy |
| LFT, blood glucose | Baseline before starting therapy |
Serological (Disease Activity Markers)
| Investigation | Rationale |
|---|---|
| ANA (if not previously done) | Confirming baseline |
| Anti-dsDNA | Rises with SLE flare, correlates with nephritis activity |
| Complement C3 and C4 | Fall with active SLE (immune complex consumption); low C3/C4 + high anti-dsDNA = classic active lupus |
| Anti-Sm | Specific for SLE |
| Anti-Ro/La | Associated with SCLE, photosensitivity, neonatal lupus, secondary Sjögren's |
| Anti-phospholipid antibodies (aCL, anti-B2GPI, LA) | Antiphospholipid syndrome risk - important before treatment |
To Differentiate from RA / Rhupus
| Investigation | Rationale |
|---|---|
| Rheumatoid Factor (RF) | Can be positive in ~25% of SLE; but high titer + erosions suggests Rhupus |
| Anti-CCP antibodies | More specific for RA; if positive with erosive arthritis = Rhupus |
| X-rays of hands and wrists | Non-erosive in SLE; periarticular osteopenia ± erosions in RA |
| Ultrasound of joints (if available) | Synovitis, erosions, tendon involvement; emerging tool in SLE arthritis assessment |
Additional
- Blood cultures (if fever present, to exclude septic arthritis/infection)
- Parvovirus B19 IgM/IgG (if viral illness history)
- Calculate SLEDAI score to quantify disease activity
Clinical tip: In SLE flares, CRP is characteristically normal or only mildly elevated despite significant synovitis. A markedly elevated CRP should raise suspicion for concurrent infection or serositis, rather than SLE activity alone.
Step 4: Management
Overall Goal
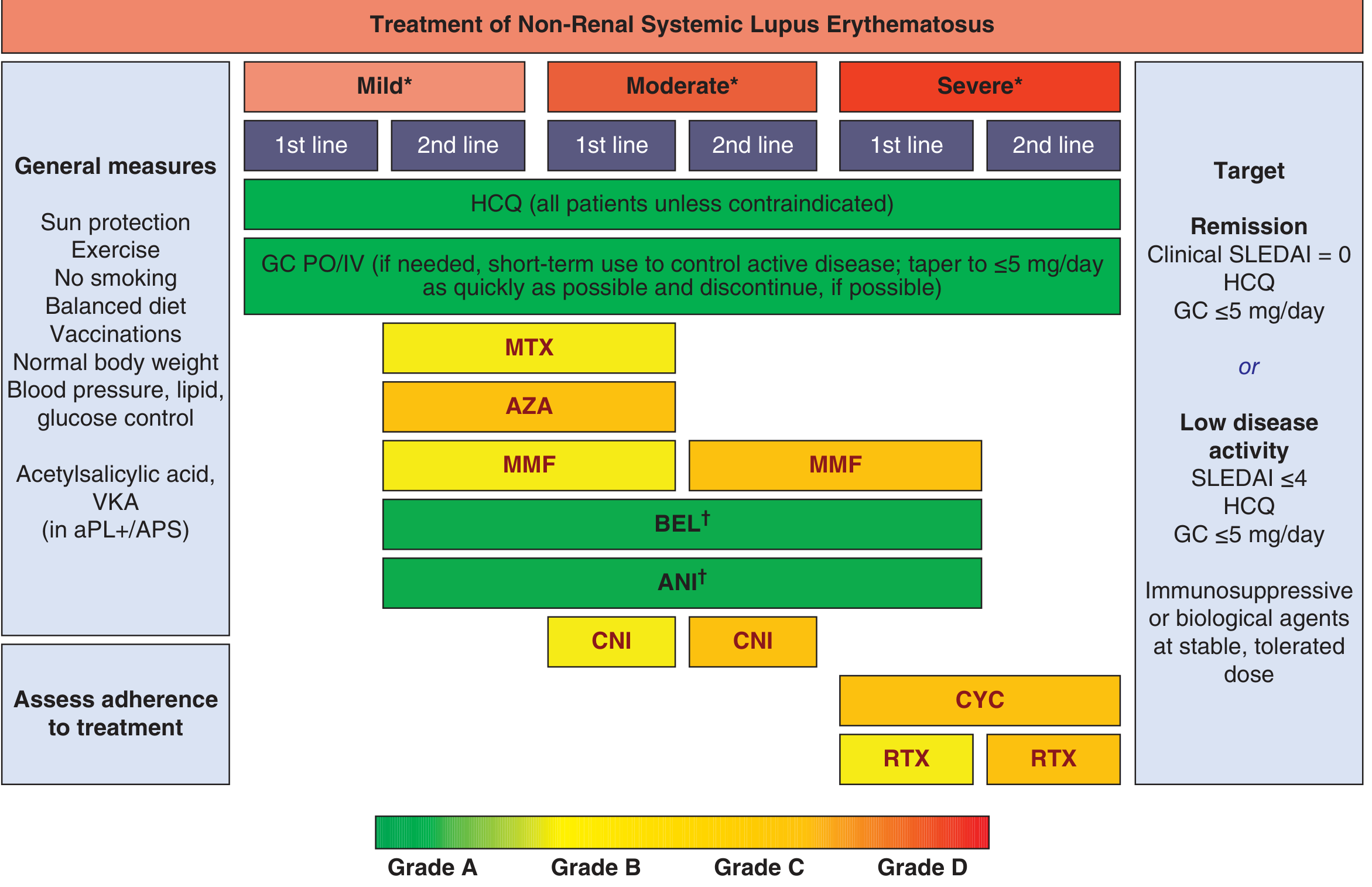
Per EULAR recommendations, the treatment target is remission (SLEDAI = 0) or low disease activity (SLEDAI ≤4), with minimal glucocorticoids (≤5 mg/day prednisone equivalent).
A. Restart Disease-Modifying Therapy
Hydroxychloroquine (HCQ) - First-line for ALL SLE patients
- Dose: up to 5 mg/kg/day (actual body weight)
- Indicated for arthritis, skin, fatigue, serositis, and to prevent flares
- Benefits: reduces flare frequency, improves survival, reduces thrombosis risk (especially if antiphospholipid antibodies present), safe in pregnancy
- Monitoring: Baseline retinal exam, then annual ophthalmology review (retinal toxicity risk with prolonged high-dose use)
- Side effects: GI symptoms (nausea, diarrhea), rash, skin dyspigmentation, rare cardiomyopathy
Important: Tobacco use reduces HCQ efficacy - advise smoking cessation.
B. For Active Joint Inflammation (Short-Term)
- NSAIDs (e.g., naproxen, celecoxib): for mild joint pain/stiffness while HCQ takes effect (4-8 weeks onset), but caution with renal function and CV risk
- Low-dose glucocorticoids (e.g., prednisone 5-15 mg/day): if more severe arthritis or if NSAIDs insufficient; taper to ≤5 mg/day as quickly as possible
C. If Inadequate Response to HCQ (Moderate Disease)
- Methotrexate (MTX): particularly useful for arthritis-dominant lupus (also used in Rhupus)
- Azathioprine (AZA): good steroid-sparing agent
- Mycophenolate mofetil (MMF): especially if renal involvement
- Belimumab (BEL): biologic (anti-BLyS), approved for active SLE, reduces flares
- Anifrolumab (ANI): anti-IFN-alpha receptor biologic, newer option for moderate-severe non-renal SLE
D. General Measures (ALL patients)
- Daily sunscreen on sun-exposed areas
- Regular exercise, healthy diet, normal BMI
- No smoking
- Blood pressure, lipid, glucose monitoring and control
- Vaccination compliance (avoid live vaccines if on immunosuppressives)
- Osteoporosis prophylaxis if on long-term steroids (calcium + vitamin D, consider bisphosphonate)
SLE Arthritis vs. RA - Key Distinguishing Features
| Feature | SLE Arthritis | RA |
|---|---|---|
| Erosions on X-ray | Rare (non-erosive) | Present |
| Deformity | Jaccoud's (reducible) | Fixed/deforming |
| RF | Low-titer (~25% positive) | High-titer (>80%) |
| Anti-CCP | Usually negative | Positive (~70%) |
| Synovitis | Mild-moderate | Severe, persistent |
| Extra-articular | Multi-organ SLE features | Nodules, vasculitis |
| Complement | Low C3/C4 | Normal |
| Anti-dsDNA | Elevated | Negative |
Treatment Algorithm (EULAR 2023, Harrison's 2025)
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 368
- Goldman-Cecil Medicine, Hydroxychloroquine section
Bottom Line for This Patient
- This presentation is most consistent with a SLE flare with polyarthritis after 6 years off treatment.
- Rule out Rhupus (send RF, anti-CCP, hand X-rays), concurrent RA, and infection.
- Assess for other organ involvement - especially lupus nephritis (urine PR:CR, renal function) and cytopenias.
- Send disease activity markers: anti-dsDNA, C3/C4, CBC.
- Restart HCQ immediately (first-line, all SLE patients) + short-course low-dose glucocorticoids/NSAIDs for acute relief.
- Calculate SLEDAI score and set target of remission or low disease activity.
- Educate on importance of not stopping treatment once started.
60 yr old pt with no symptoms, madsive spleenomegaly on usg abdomen, normocytic normochromic rbc, eosinophilia in ph smear, pancytopenia in cbc, why not its ITP
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have all the information needed for a thorough, structured answer. Let me compose it.
Why This is NOT ITP - Clinical Reasoning
This is an excellent reasoning question. The clues in this case actively argue against ITP one by one, and together point strongly toward a different diagnosis. Here is a systematic breakdown:
The 4 Clues That Exclude ITP
1. MASSIVE SPLENOMEGALY - The Strongest Argument Against ITP
This is the single most important clue.
"Splenomegaly is uncommon with ITP in both adults and children, and its occurrence should prompt a search for a separate cause of thrombocytopenia."
- Schwartz's Principles of Surgery, 11th Ed.
In ITP, the spleen is a site of platelet destruction and anti-platelet antibody production - it does not enlarge massively because there is no infiltration, congestion, or extramedullary hematopoiesis. A massive spleen on USG in a 60-year-old is a red flag for:
- Myeloproliferative neoplasm (myelofibrosis, CML, PV)
- Lymphoma (especially hairy cell leukemia, splenic marginal zone lymphoma)
- Visceral leishmaniasis (kala-azar)
- Chronic malaria
- Gaucher disease
- Portal hypertension / congestive splenomegaly
2. PANCYTOPENIA - Not the Pattern of ITP
| Feature | ITP | This Patient |
|---|---|---|
| Platelets | Low (isolated) | Low |
| Hemoglobin | Normal | Low (pancytopenia) |
| WBC | Normal | Low (pancytopenia) |
ITP causes isolated thrombocytopenia. It is an antibody-mediated destruction of platelets only. There is no mechanism in ITP that destroys RBCs and WBCs simultaneously.
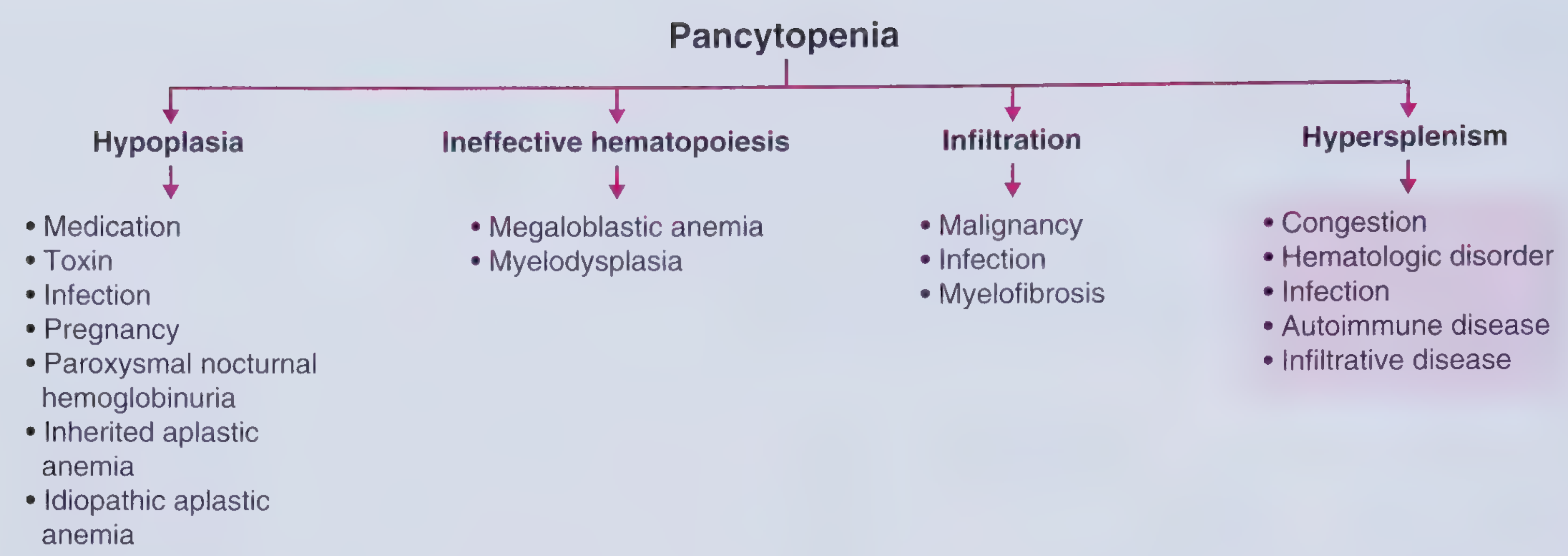
The presence of pancytopenia (all three cell lines low) means the problem is either:
- Hypersplenism - the massive spleen is sequestering all cell lines (can sequester up to 90% of platelets, 65% of granulocytes, 30% of RBCs)
- Bone marrow failure / infiltration / replacement
- A systemic disease hitting the marrow
3. NORMOCYTIC NORMOCHROMIC ANEMIA - Argues Against ITP
In ITP, if there is any anemia, it is either:
- Microangiopathic/hemolytic (Evans syndrome = ITP + AIHA, with spherocytes on smear)
- Due to blood loss (iron deficiency = microcytic, hypochromic)
Normocytic normochromic anemia in this context suggests:
- Anemia of chronic disease
- Hemolytic anemia with compensated picture (but the smear shows eosinophilia, not spherocytes)
- Splenic sequestration effect
- Early bone marrow infiltration/replacement
4. EOSINOPHILIA ON PERIPHERAL SMEAR - Completely Unexplained by ITP
ITP has no mechanism to cause eosinophilia. This single finding effectively eliminates ITP as the diagnosis. Eosinophilia in this context, combined with massive splenomegaly, strongly points toward:
- Parasitic infection - visceral leishmaniasis (kala-azar), schistosomiasis, hyperreactive malarial splenomegaly, toxocariasis
- Myeloproliferative neoplasm with eosinophilia - chronic eosinophilic leukemia, CML
- Lymphoma - Hodgkin lymphoma (classic cause of eosinophilia + splenomegaly)
- Hypereosinophilic syndrome
Why ITP Does NOT Explain This Case - Summary Table
| Feature Present | Expected in ITP? | Explains ITP Exclusion |
|---|---|---|
| Massive splenomegaly | ✗ No - spleen rarely enlarged | ITP doesn't cause massive splenomegaly |
| Pancytopenia (all 3 lines) | ✗ No - only platelets fall | ITP is isolated thrombocytopenia |
| Normocytic normochromic RBC | Partial - only if Evans or blood loss | Doesn't fit typical ITP pattern |
| Eosinophilia on smear | ✗ Never | ITP has zero mechanism for eosinophilia |
| 60 yrs old, asymptomatic | Partial - adult ITP exists | But adult ITP usually has bleeding symptoms |
| No symptoms | Unusual | Symptomatic thrombocytopenia expected |
What IS the Likely Diagnosis?
The combination of massive splenomegaly + pancytopenia + eosinophilia + normocytic normochromic anemia + asymptomatic 60-year-old fits best with:
Top Differentials:
-
Visceral Leishmaniasis (Kala-azar)
- Classic: months of fever, fatigue, weight loss, massive splenomegaly, pancytopenia
- Eosinophilia can be present (though more commonly eosinopenia)
- Endemic areas relevant
- Diagnosis: rK39 antigen test, bone marrow aspirate (Leishman-Donovan bodies)
-
Myelofibrosis (Primary Myelofibrosis)
- Massive splenomegaly from extramedullary hematopoiesis
- Pancytopenia from marrow fibrosis + hypersplenism
- Leukoerythroblastic smear ± eosinophilia, teardrop RBCs
- Diagnosis: bone marrow biopsy (dry tap), JAK2/CALR/MPL mutations
-
Lymphoma (Splenic Marginal Zone / Hodgkin / NHL)
- Massive splenomegaly, pancytopenia from hypersplenism
- Eosinophilia (especially Hodgkin lymphoma)
- Diagnosis: LDH, CT scan, FNAC/biopsy
-
Hyperreactive Malarial Splenomegaly (Tropical Splenomegaly)
- Massive splenomegaly, anemia, pancytopenia
- High malarial antibody titers, eosinophilia
- Responds to antimalarials
-
Chronic Myeloid Leukemia (CML)
- Massive splenomegaly, high WBC (or paradoxically low with hypersplenism)
- Eosinophilia/basophilia on smear
- BCR-ABL positive
Mechanism: Why Pancytopenia with Massive Spleen
This is hypersplenism:
"Massive spleens are capable of sequestering up to 90% of peripheral platelets, 65% of granulocytes, and 30% of RBCs."
- Frameworks for Internal Medicine
Hypersplenism is defined as: splenomegaly + one or more peripheral cytopenias + normo/hypercellular bone marrow. It is the underlying mechanism for pancytopenia here, driven by whatever disease is causing the massive spleen.
Investigations to Order
| Test | Purpose |
|---|---|
| Peripheral blood smear review | Teardrop cells (myelofibrosis), LE cells, blasts, Reed-Sternberg precursors, malarial parasites |
| Bone marrow aspirate + biopsy | Leishmaniasis (LD bodies), fibrosis, lymphoma infiltration |
| LDH, uric acid | Lymphoma/myeloproliferative activity |
| rK39 antigen test / Leishmania serology | Kala-azar |
| Malaria antigen / thick smear | Malaria |
| JAK2 V617F mutation | Myelofibrosis, PV |
| BCR-ABL (FISH/PCR) | CML |
| CT abdomen + chest | Lymphadenopathy, liver involvement |
| LFT, PT/INR | Portal hypertension from hepatic disease |
Bottom Line
ITP is excluded by 4 simultaneous arguments:
- ITP does not cause massive splenomegaly
- ITP causes only thrombocytopenia, not pancytopenia
- ITP has no mechanism for eosinophilia
- ITP in adults causes bleeding symptoms - this patient is asymptomatic
The true diagnosis in this 60-year-old is most likely hypersplenism from an underlying systemic disease - with visceral leishmaniasis, myelofibrosis, and lymphoma at the top of the list. A bone marrow biopsy is the single most important next step.
This is a shared conversation. Sign in to Orris to start your own chat.