Deltoid fibrosis etiology pathology signs and problems symptoms investigation and treatment explain in detail with appropriate illustrative diagrams and images
Reading File
Finding Sources
Finding Sources
Searching the Web
deltoid fibrosis etiology pathology signs symptoms treatment
Searching Images
deltoid fibrosis contracture shoulder
Finding Sources
Finding Sources
Searching PubMed
deltoid fibrosis contracture
Loading Image
Finding Sources
Searching PubMed
deltoid fibrosis intramuscular injection
Loading Image
Loading Image
Finding Sources
Finding Sources
Searching Images
deltoid muscle anatomy injection site intramuscular
Finding Sources
Finding Sources
Loading Image
Reading File
Searching the Web
deltoid fibrosis injection site contracture abduction deformity children management
Searching Images
deltoid muscle anatomy shoulder abduction posterior anterior middle fibers
I now have comprehensive information and images. Let me compile the full detailed response:
Deltoid Fibrosis — A Comprehensive Clinical Review
1. Introduction & Definition
Deltoid fibrosis (also called deltoid contracture or injection-induced deltoid fibrosis) is a condition in which the deltoid muscle — the triangular, multipennate muscle covering the shoulder joint — undergoes progressive replacement of normal muscle fibers with dense fibrous scar tissue, resulting in a fixed abduction contracture of the shoulder. The fibrotic band tethers the arm in a partially abducted position, preventing full adduction.
It is predominantly seen in children and young adults and represents a preventable iatrogenic complication in most cases.
2. Anatomy Relevant to the Condition
The deltoid muscle has three heads:
- Anterior (clavicular) — flexion, medial rotation
- Middle (acromial) — pure abduction (the most prominent part, most frequently injected)
- Posterior (spinous) — extension, lateral rotation
All converge onto the deltoid tuberosity of the humerus. The muscle is innervated by the axillary nerve (C5, C6), which runs through the quadrangular space and winds around the surgical neck of the humerus beneath the deltoid.
3. Etiology
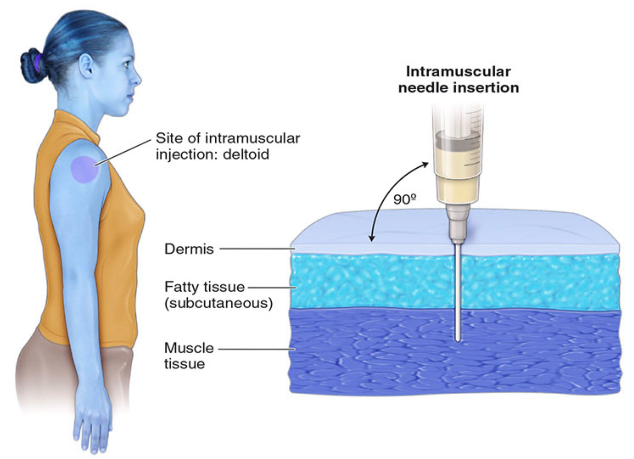
Primary Cause: Repeated Intramuscular (IM) Injections
The overwhelming majority of cases are caused by repeated IM injections into the deltoid, particularly in infancy and early childhood when the muscle bulk is small and repeated injections cause cumulative tissue damage.
Specific culprit drugs:
- Quinine — historically the most notorious offender; highly irritating to muscle tissue, causing intense local necrosis and subsequent fibrosis. As noted in Das' Manual on Clinical Surgery, "Irritating drugs such as quinine when injected intramuscularly in the deltoid may affect the axillary nerve."
- Penicillin (long-acting preparations) — benzathine penicillin, procaine penicillin
- Antimalarial agents (chloroquine, quinine)
- Vaccines administered too high (into the subdeltoid bursa rather than muscle)
- Oily/depot injections — iron dextran, vitamin preparations
- Antibiotics — streptomycin, tetracycline
Other Causes
| Category | Examples |
|---|---|
| Trauma | Penetrating injuries, crush injury to shoulder |
| Infection | Pyomyositis, abscess of deltoid |
| Post-surgical | After shoulder arthrotomy or deltoid-splitting approaches |
| Idiopathic | Rare; no identifiable cause |
| Genetic/hereditary | Very rare; associated with congenital fibromatosis |
4. Pathology
Macroscopic
- The deltoid muscle (particularly its middle head) is replaced by a dense white fibrous band
- The fibrotic band is firm to hard on palpation, running vertically from the acromion toward the deltoid tuberosity
- Overlying skin may show a characteristic skin dimple or furrow corresponding to the fibrous cord beneath (see clinical photo below)
- In chronic cases, the muscle belly is atrophied and pale
Microscopic
- Collagen deposition — dense type I and III collagen bundles replace muscle fibers
- Myofibroblasts — key cellular mediators of fibrosis; identical to those seen in Dupuytren's contracture (as noted in Miller's Review of Orthopaedics: "Frozen shoulder histologic evaluation demonstrates evidence of inflammation and fibrosis. There is a dense matrix of type III collagen–containing fibroblasts and myofibroblasts")
- Loss of muscle architecture — sarcomeres and cross-striations absent in fibrotic areas
- Chronic inflammatory infiltrate — lymphocytes, macrophages in early stages
- Fatty infiltration — in longstanding cases
- Calcification — dystrophic calcification may occur in old fibrotic bands
Pathogenesis Sequence
Repeated injection / chemical irritant
↓
Local myonecrosis (ischemic or direct toxic)
↓
Inflammatory response (macrophages, mast cells)
↓
Fibroblast/myofibroblast recruitment & activation
↓
Excessive ECM (collagen) deposition
↓
Fibrous band formation
↓
Progressive contracture & mechanical restriction
5. Clinical Features
Signs & Symptoms
Typical Presentation
The classic patient is a child 3–12 years old with a history of multiple IM injections in the deltoid region, presenting with:
Postural abnormality:
- The arm is held in fixed partial abduction (typically 30–50°)
- The child cannot fully adduct the arm to the side of the body
- The shoulder appears "sprung out" from the body
Visible signs:
- Skin dimple or vertical furrow over the lateral deltoid (pathognomonic) — corresponds to the fibrous band pulling skin inward
- Deltoid atrophy — particularly if the axillary nerve is also affected
- Shoulder asymmetry — on frontal view, the affected shoulder appears higher and projected laterally
- Winging of the scapula — secondary to altered shoulder mechanics
On movement:
- Restricted passive adduction — cannot bring arm close to trunk
- Abduction is often preserved or even excessive — because the fibrotic band acts as a passive abductor
- "Reverse shoulder rhythm" — the scapula elevates early on attempted adduction

Secondary Complications
- Glenohumeral joint subluxation/dislocation — in long-standing neglected cases; the humeral head may sublux anteriorly
- Shoulder joint dysplasia — disrupted development in children
- Scoliosis — compensatory spinal curvature
- Thoracic cage asymmetry
- Axillary nerve damage — may coexist if the injection caused direct nerve injury
6. Radiological Investigations
Plain X-Ray (AP & Axial Shoulder)
- Usually normal in early cases
- In advanced/neglected cases:
- Inferior subluxation or anterior dislocation of humeral head
- Drooping/elongation of acromion
- Tapering of distal clavicle
- Joint space narrowing
- Evidence of glenohumeral dysplasia

Ultrasound (USG)
- First-line imaging in children (no radiation, dynamic assessment)
- Demonstrates:
- Hyperechoic fibrous band within deltoid
- Muscle atrophy and echogenicity changes
- Axillary nerve assessment
- Dynamic assessment of band tightness during abduction/adduction
MRI
- Best for soft tissue characterization
- Shows:
- Low T1 and T2 signal fibrous band within deltoid (collagen is hypointense on both sequences)
- Muscle atrophy and fatty infiltration (high T1 signal)
- Associated joint changes
- Axillary nerve status
EMG/Nerve Conduction Studies
- Indicated when axillary nerve injury is suspected
- May show:
- Reduced CMAP amplitude from deltoid
- Denervation potentials (fibrillations, positive sharp waves) on EMG
- Normal conduction velocity (axonotmesis pattern)
7. Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Brachial plexus birth palsy | Present from birth, flaccid paresis, history of difficult delivery |
| Glenohumeral joint dislocation | X-ray confirms, no fibrous band |
| Sprengel's shoulder | Elevated scapula, bony abnormality, congenital |
| Obstetric paralysis (Erb's) | Waiter's tip posture, weakness, birth history |
| Frozen shoulder (adhesive capsulitis) | Adults, pain-predominant, restriction in all planes, no injection history |
| Calcific tendinitis | Painful, calcification on X-ray, normal adduction |
| Quadrangular space syndrome | Axillary nerve compression, no contracture, often in athletes |
8. Treatment
Conservative Treatment
Indicated in early/mild cases with incomplete fibrosis:
-
Physiotherapy
- Passive stretching of the deltoid into adduction
- Heat therapy (ultrasound/shortwave diathermy) to soften fibrotic tissue
- Massage of the fibrous band
- Active-assisted range of motion exercises
-
Corticosteroid injection
- Into the fibrous band
- May soften early fibrosis
- Limited long-term benefit in established contracture
-
Extracorporeal shockwave therapy (ESWT)
- Emerging modality for early fibrosis
Important: Conservative treatment alone is rarely curative for established deltoid fibrosis with significant contracture. Surgery is usually required.
Surgical Treatment
Surgery is the definitive treatment and should be performed before secondary joint changes develop (ideally before age 7–8 in children).
Principle
Division and excision of the fibrous band restoring full adduction.
Approaches
1. Open Surgical Release (Fibrotic Band Excision)
- Most commonly performed
- Incision over the lateral deltoid
- Identification and excision of the fibrous band
- Preservation of normal muscle fibers
- If the band is extensive, deltoid muscle Z-plasty or stepcut lengthening is performed
- The axillary nerve is identified and protected throughout
2. Arthroscopic/Minimally Invasive Release
- Emerging technique in specialized centers
- Endoscopic visualization and division of fibrotic tissue
- Lower morbidity, faster recovery
3. Management of Associated Joint Pathology
- Capsular release if secondary adhesive capsulitis
- Reduction of subluxed joint
- Rare cases may need shoulder arthroplasty in adults
Postoperative Care
- Immobilization in adduction for 2–3 weeks
- Early passive mobilization commenced
- Intensive physiotherapy for 3–6 months
- Progressive active strengthening of deltoid

9. Complications of Untreated Deltoid Fibrosis
- Progressive worsening of the abduction contracture
- Glenohumeral joint subluxation → dislocation
- Joint dysplasia and irreversible cartilage damage
- Scoliosis and thoracic asymmetry
- Cosmetic deformity and social/psychological impact
- Functional disability (difficulty with activities of daily living requiring adduction)
10. Prevention (Critical)
Since the vast majority of cases are iatrogenic, prevention is paramount:
- Correct injection technique — inject into the middle third of the deltoid, not too superiorly (avoids bursa, axillary nerve, and periosteum)
- Rotate injection sites — never repeatedly inject the same quadrant
- Appropriate needle length and gauge — ensure delivery into muscle, not subcutaneous fat
- Use the least irritating drug formulation available
- Avoid irritating drugs (quinine, depot preparations) via the deltoid whenever possible — use gluteal or thigh muscles instead
- Train healthcare workers in proper IM injection technique
- Vaccination programs should follow standardized injection protocols
Summary Table
| Feature | Detail |
|---|---|
| Most common cause | Repeated IM injections (quinine, penicillin) |
| Most common age | Children 3–12 years |
| Classic sign | Fixed shoulder abduction + skin dimple over deltoid |
| Pathology | Collagen-replacing fibrous band; myofibroblasts |
| Best imaging | MRI (characterization); USG (dynamic, no radiation) |
| Definitive treatment | Surgical excision/release of fibrotic band |
| Key prevention | Correct IM injection technique and site rotation |
Sources:
- S Das — A Manual on Clinical Surgery, 13th Edition (injection injury to deltoid and nerve)
- Miller's Review of Orthopaedics, 9th Edition (fibrosis histology, myofibroblasts)
- Gray's Anatomy for Students (deltoid and quadrangular space anatomy)
- Harrison's Principles of Internal Medicine, 21st Edition (IM injection technique)
- Clinical images from published PMC literature (deltoid contracture clinical series)
This is a shared conversation. Sign in to Orris to start your own chat.