Bulky uterus and grade 1 fatty liver relation in obs ang gyne
Reading File
Finding Sources
Finding Sources
Searching PubMed
fatty liver NAFLD uterine fibroids adenomyosis metabolic
Finding Sources
Finding Sources
Searching PubMed
NAFLD uterine fibroid insulin resistance metabolic syndrome women
Finding Sources
Finding Sources
Searching PubMed
adenomyosis metabolic syndrome obesity insulin
Finding Sources
Finding Sources
Searching the Web
bulky uterus grade 1 fatty liver relationship metabolic syndrome obstetrics gynecology
Reading File
Searching PubMed
PCOS NAFLD nonalcoholic fatty liver polycystic ovary syndrome
Excellent - I now have strong evidence. Let me compile a comprehensive answer.
Bulky Uterus and Grade 1 Fatty Liver: Relationship in Obs & Gynae
These two findings - a bulky uterus and Grade 1 fatty liver (hepatic steatosis) on ultrasound - are not directly causally linked, but they are frequently seen together because they share the same underlying metabolic and hormonal axis. Understanding this relationship is clinically important for holistic patient management.
1. What Causes a "Bulky Uterus"?
The term "bulky uterus" is an ultrasound description, not a diagnosis. Common causes include:
| Cause | Key features |
|---|---|
| Adenomyosis | Enlarged, globular uterus; endometrial glands within myometrium |
| Uterine fibroids (leiomyomata) | Most common benign gynecological tumor |
| PCOS | Multifollicular ovaries + metabolic features; uterus may appear bulky |
| Endometrial hyperplasia/cancer | Particularly in obese, anovulatory women |
| Pregnancy | Always exclude |
2. What is Grade 1 Fatty Liver?
Grade 1 (mild) hepatic steatosis = fat deposition in >5% of hepatocytes but <33%, seen as increased echogenicity on ultrasound. Most commonly due to Non-Alcoholic Fatty Liver Disease (NAFLD/MAFLD), strongly tied to insulin resistance and metabolic syndrome.
3. The Common Metabolic Link (Most Important)
A. Obesity and Insulin Resistance - The Central Connector
Obesity drives both conditions simultaneously:
-
Bulky uterus: Obesity increases risk of fibroids by 21% per 10 kg increase in body weight. It does this by:
- Increasing conversion of adrenal androgens to estrone in adipose tissue
- Decreasing sex hormone-binding globulin (SHBG)
- Net result: increased biologically available estrogen → promotes fibroid growth and uterine hypertrophy
- Berek & Novak's Gynecology, p. 502
-
Grade 1 fatty liver: Obesity drives hepatic lipid accumulation, insulin resistance, and visceral adiposity → NAFLD
B. PCOS - The Strongest Single Link in Reproductive-Age Women
PCOS is the most important gynecological condition connecting a bulky/multicystic uterus with fatty liver:
- PCOS patients have higher prevalence of insulin resistance, dyslipidemia, hypertension, and obesity - all components of metabolic syndrome (Dermatology 2-Volume Set, Harrison's Principles of Internal Medicine 22E)
- PCOS more than doubles the risk of fatty liver disease, even without obesity, diabetes, or other major risk factors
- A 2023 Meta-Analysis (Liu D et al., BMC Med; PMID 36800955) established genetic/causal evidence for a hepato-ovarian axis - NAFLD and PCOS are bidirectionally linked
- The uterus in PCOS can appear bulky due to anovulation, endometrial thickening, and associated adenomyosis
C. Estrogen Excess and Hepatic Metabolism
- Estrogen modulates hepatic lipid metabolism through estrogen receptors in the liver
- Hyperestrogenic states (anovulatory cycles in PCOS, obesity-related estrone excess) can impair hepatic lipid processing
- A 2022 Systematic Review (PMID 36419770) confirmed NAFLD interacts significantly with sex hormones across multiple endocrinopathies
4. Pathway Summary
OBESITY / INSULIN RESISTANCE
│
┌────┴────┐
▼ ▼
↑ Free estrogen ↑ Hepatic lipid deposition
↓ SHBG ↓ Beta-oxidation
│ │
▼ ▼
BULKY UTERUS GRADE 1 FATTY LIVER
(fibroids / adenomyosis) (NAFLD/MAFLD)
PCOS amplifies both arms of this pathway simultaneously.
5. Clinical Implications in Obs & Gynae Practice
| Issue | Relevance |
|---|---|
| Screen for metabolic syndrome | Any woman with bulky uterus + fatty liver should have: fasting glucose, HbA1c, lipid profile, BP |
| PCOS evaluation | Check for anovulation, hyperandrogenism, LH:FSH ratio, AMH |
| Endometrial cancer risk | Both obesity-driven hyperestrogenism (bulky uterus) and NAFLD are associated with uterine/endometrial malignancy |
| Preoperative workup | Fatty liver increases surgical and anesthetic risk (impaired coagulation factor synthesis, drug metabolism) in gynecological procedures (myomectomy, hysterectomy) |
| Fertility | Insulin resistance impairs ovulation; NAFLD-associated hormonal derangements worsen fertility outcomes |
| Lifestyle modification | Weight loss of 5-10% improves both uterine symptoms AND hepatic steatosis |
| Metformin | Used in PCOS - also reduces hepatic gluconeogenesis and has benefit in both PCOS-related uterine pathology and fatty liver |
6. Key Evidence
- Liu D et al. (2023) - "The hepato-ovarian axis" - Meta-analysis showing NAFLD and PCOS are causally linked (PMID 36800955)
- Arefhosseini et al. (2022) - NAFLD and sex hormones - Systematic review on NAFLD across endocrinopathies (PMID 36419770)
- Półkośnik et al. (2023) - NAFLD and PCOS in adolescents - Systematic review on pathogenesis and management (PMID 37455412)
- Berek & Novak's Gynecology - Obesity-fibroid link via estrogen/SHBG mechanism
Summary
A bulky uterus and Grade 1 fatty liver appearing together on ultrasound should prompt evaluation for the metabolic syndrome, PCOS, and insulin resistance - these are the unifying pathophysiological threads. The finding of both on a single scan is not coincidental; it is a red flag for underlying systemic metabolic dysfunction that requires coordinated gynecological and medical management.
Explain the role of metformin and lifestyle modification in both conditions
Finding Sources
Finding Sources
Searching PubMed
metformin NAFLD nonalcoholic fatty liver disease treatment
Reading File
Reading File
Searching PubMed
lifestyle modification weight loss NAFLD fatty liver exercise diet
Finding Sources
Finding Sources
Searching PubMed
lifestyle weight loss exercise PCOS polycystic ovary syndrome treatment
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
I now have everything needed for a thorough, well-cited answer. Here it is:
Metformin and Lifestyle Modification in Bulky Uterus + Grade 1 Fatty Liver
Both interventions work through the same metabolic axis - reducing insulin resistance, lowering free estrogen, and reversing hepatic steatosis. They are complementary and synergistic.
Part 1: Mechanism of Metformin (The Biochemical Core)
Metformin is a biguanide that acts via AMPK (AMP-activated protein kinase) activation:
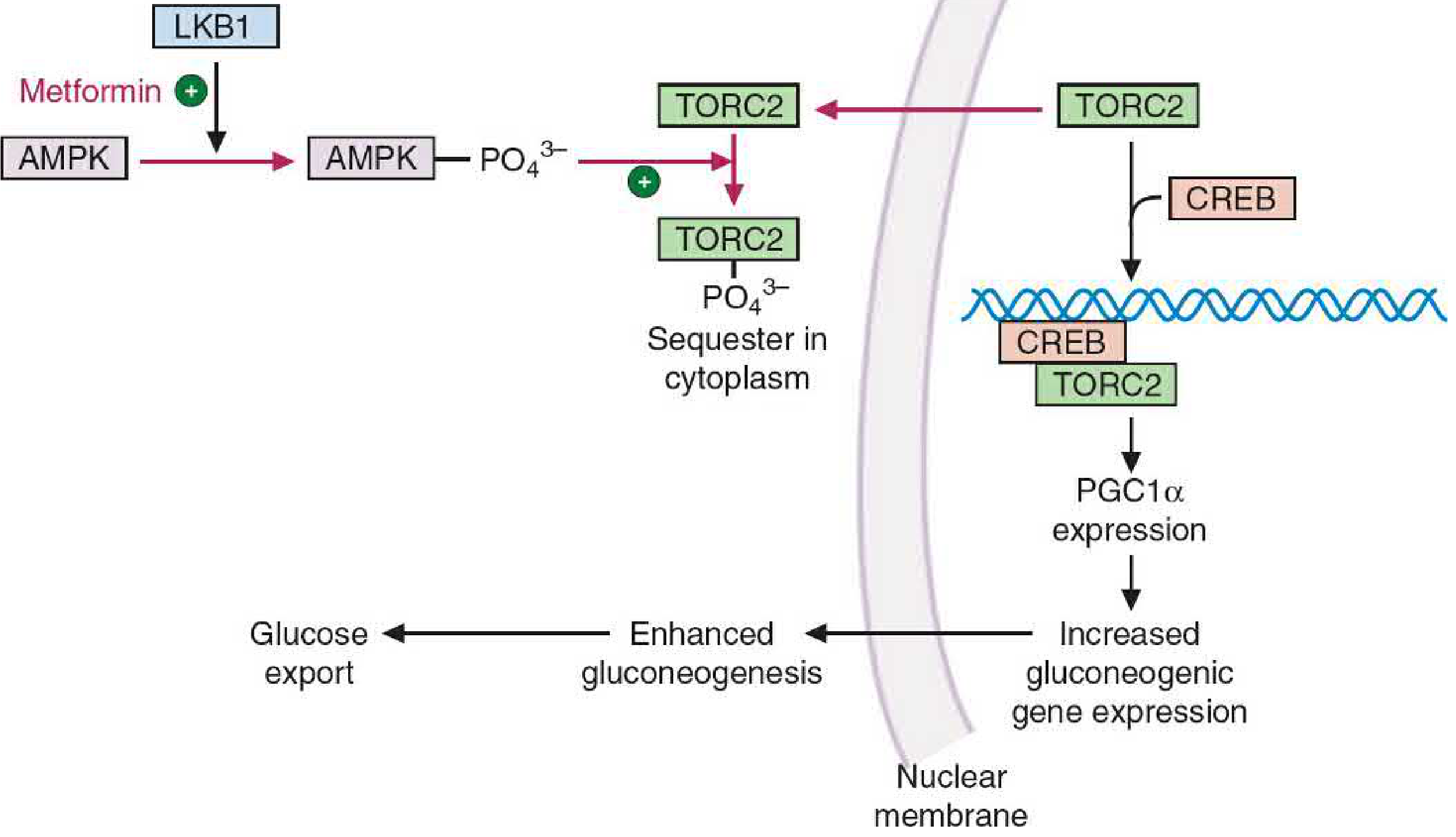
Metformin activates LKB1 → AMPK → phosphorylates TORC2 (sequesters it in cytoplasm) → blocks CREB-PGC1α transcription → reduces gluconeogenic enzyme (G6Pase, PEPCK) expression → less hepatic glucose output. Simultaneously, AMPK inhibits acetyl-CoA carboxylase → reduces fatty acid synthesis → reduces hepatic lipogenesis.
- Basic Medical Biochemistry - A Clinical Approach 6e, p.1226
The 4 key molecular effects of metformin:
| Action | Benefit in both conditions |
|---|---|
| ↓ Hepatic gluconeogenesis | Reduces blood glucose, directly addresses NAFLD |
| ↓ Hepatic lipogenesis (via AMPK → ↓ ACC, ↓ FAS) | Reduces hepatic fat content |
| ↑ Peripheral glucose uptake by muscle | Lowers insulin levels → less thecal androgen → better ovulation |
| ↓ Gut glucose absorption | Additonal glycemic benefit |
Part 2: Role in Bulky Uterus / PCOS / Uterine Pathology
How it helps:
1. Restores Ovulation
- Insulin resistance in PCOS drives hyperinsulinemia → excess LH → excess thecal androgen production → anovulation
- Metformin breaks this cycle by improving insulin sensitivity → lower LH → restored folliculogenesis
- Increases frequency of spontaneous ovulation in PCOS patients
- Berek & Novak's Gynecology, p.2053
2. Reduces Androgens and Hirsutism
- Lower insulin → less androgen from thecal cells → decreased total and bioavailable testosterone
- Clinically reduces acne, hirsutism, and menstrual irregularity
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry, p.7006
3. Reduces BMI and Waist-to-Hip Ratio
- Significant decrease in BMI observed with metformin treatment in PCOS
- This reduces aromatization of androgens to estrone in adipose tissue → reduces free estrogen → less stimulus for fibroid/uterine growth
- Berek & Novak's Gynecology: obesity increases fibroid risk 21% per 10 kg via ↑estrone and ↓SHBG
4. Protects Endometrium
- Anovulation in PCOS = unopposed estrogen = risk of endometrial hyperplasia
- By restoring ovulation, metformin restores cyclic progesterone exposure → protects endometrium
- Note: if metformin alone does not restore regular ovulation, cyclic progestogen (medroxyprogesterone acetate 10mg for 12-14 days/month) must be added to prevent hyperplasia
- Berek & Novak's Gynecology, p.1893
Dosing in PCOS:
- Start: 500 mg TDS or 850 mg BD (titrate slowly to reduce GI side effects)
- Extended release formulations have fewer GI side effects
- Maximum effective dose: 1500-2550 mg/day
Caution: Avoid in hepatic/renal dysfunction, pre-contrast imaging, perioperative period (risk of lactic acidosis).
Part 3: Role in Grade 1 Fatty Liver (NAFLD/MAFLD)
How it helps:
1. Direct Anti-steatotic Effect
- AMPK activation → ↓ ACC → ↓ malonyl CoA → ↓ fatty acid synthesis + ↑ fatty acid beta-oxidation
- AMPK also inhibits SREBP-1c transcription → less lipogenic enzyme (FAS, ACC) expression → net reduction in hepatic fat
- Basic Medical Biochemistry 6e, p.1226
2. Reduces Liver Glucose Output
- In insulin-resistant states, the liver produces excess glucose even in the fed state (CREB-PGC1α pathway remains active)
- Metformin blocks this → reduces hepatic glucose export → improves metabolic milieu driving NAFLD
3. Evidence from Meta-Analysis
- A 2022 Systematic Review & Meta-Analysis (Huang Y et al., Medicine; PMID 36316840) confirmed metformin significantly reduces liver enzymes (ALT, AST) and hepatic steatosis in NAFLD patients
- A pediatric meta-analysis (Gkiourtzis N et al., Eur J Pediatr 2023; PMID 37639015) also showed benefit in fatty liver outcomes
Practical limitation: Metformin is considered a secondary agent for NAFLD specifically - it is not formally approved for fatty liver, but in patients who have BOTH PCOS/insulin resistance AND fatty liver, it addresses both simultaneously. It is not recommended when advanced fibrosis or cirrhosis is present.
Part 4: Role of Lifestyle Modification
This is actually first-line for both conditions, and more powerful than any drug when adhered to.
A. Weight Loss - The Single Most Impactful Intervention
| Weight loss achieved | Effect on bulky uterus | Effect on fatty liver |
|---|---|---|
| 5% body weight | Improved menstrual regularity, lower androgens | Significant reduction in hepatic steatosis |
| 7-10% body weight | Restored ovulation, improved fertility, reduced fibroid stimulus | Near-complete resolution of Grade 1 steatosis; reduced inflammation |
| >10% body weight | Marked reduction in PCOS features | Can reverse NASH (steatohepatitis) |
- Weight reduction in obese PCOS women → improved pregnancy rates, decreased hirsutism, improved glucose and lipid levels
- Berek & Novak's Gynecology, p.1893
B. Diet
For both conditions:
- Caloric restriction (500-1000 kcal/day deficit) is the backbone
- Mediterranean diet - rich in olive oil, fish, vegetables, whole grains; reduces hepatic fat and insulin resistance
- Low glycaemic index diet - reduces postprandial insulin spikes, key for PCOS
- Reduce: refined carbohydrates, saturated fat, red meat, ultra-processed foods
- For fibroids specifically: diets rich in green vegetables reduce incidence; red meat and ham increase risk (Berek & Novak's Gynecology, p.502)
Dietary interventions confirmed by: Houttu V et al., Front Nutr 2021; PMID 34368214 and Hadefi A et al., United European Gastroenterol J 2023; PMID 37491835
C. Exercise
- Minimum: 150 minutes/week moderate-intensity aerobic exercise (e.g., brisk walking, cycling)
- Add resistance/strength training ≥2 days/week
- Exercise independently reduces hepatic fat even without significant weight loss (by increasing AMPK activity in muscle and liver - mimics metformin's mechanism!)
- In PCOS: reduces androgen levels, improves insulin sensitivity, and improves ovulation rates
- Women exercising >7 hours/week have significantly lower fibroid risk vs. <2 hours/week
- Berek & Novak's Gynecology
Evidence: Chen MJ et al., Front Nutr 2024; PMID 39834455 - comprehensive evidence summary of lifestyle interventions in MAFLD
Part 5: Comparison - Metformin vs. Lifestyle (Practical Summary)
| Parameter | Lifestyle Modification | Metformin |
|---|---|---|
| First-line status | YES - always first-line | Second-line / adjunct |
| Effect on hepatic fat | ✓✓✓ (strongest evidence) | ✓✓ |
| Effect on ovulation (PCOS) | ✓✓✓ (via weight loss) | ✓✓ |
| Effect on androgens | ✓✓ | ✓✓ |
| Endometrial protection | Indirect (via restored cycles) | Partial (via ovulation restoration) |
| BMI reduction | ✓✓✓ | ✓ (modest, ~2-3 kg) |
| Sustainability | Difficult without support | Easy to maintain |
| Side effects | None (if done safely) | GI upset, rare lactic acidosis |
| Best use | Obese/overweight patients | All PCOS + insulin resistance patients; adjunct in NAFLD |
The winning strategy is combining both: A 2025 Systematic Review (Gautam R et al., Nutrients; PMID 39861440) confirms lifestyle interventions are the cornerstone of PCOS management, with metformin amplifying the benefits especially in insulin-resistant and obese patients.
Clinical Takeaway
In a patient with bulky uterus + Grade 1 fatty liver, the management approach should be:
- Lifestyle first - caloric restriction, Mediterranean diet, 150+ min/week aerobic + resistance exercise
- Metformin (500-2000 mg/day titrated) - if PCOS or insulin resistance is confirmed; addresses both uterine and hepatic pathology simultaneously through AMPK
- Endometrial protection - if anovulation persists despite metformin, add cyclic progestogen
- Monitor: HbA1c, fasting insulin, lipid profile, LFTs, liver ultrasound at 6 months
- Target: 7-10% weight loss as the primary therapeutic goal - more impactful than any pharmacotherapy alone
This is a shared conversation. Sign in to Orris to start your own chat.