what contributes to a tendinopathy pathophysiology of a tendinopathy how you would load- what exercises to get a tension patchy stronger achilles tendinopathy, patella tendinopathy tibialis posterior tendinopathy
what contributes to a tendinopathy pathophysiology of a tendinopathy how you would load- what exercises to get a tendinopathy stronger achilles tendinopathy, patella tendinopathy tibialis posterior tendinopathy
Tendinopathy — Complete Overview
What Contributes to Tendinopathy
- Increasing age (decreased tensile strength and blood supply)
- Male gender
- Obesity (especially for weight-bearing tendons)
- Muscle weakness and imbalance
- Insufficient flexibility
- Malalignment (e.g. flat foot driving tibialis posterior overload)
- Diabetes mellitus
- Chronic renal failure
- Rheumatoid arthritis / SLE
- Corticosteroid use
- Fluoroquinolone antibiotics (ciprofloxacin etc.) — strong independent risk
- Training errors (sudden increase in volume or intensity)
- Improper equipment or footwear
- Repetitive mechanical loading beyond the tendon's capacity
Pathophysiology
- Disorganisation and degeneration of collagen fibres — the ordered parallel collagen architecture breaks down
- Mucoid degeneration — ground substance accumulates between fibres
- Infiltration by macrophages, plasma cells, and lymphocytes (not neutrophils/leukocytes — minimal acute inflammation)
- Increased but dysfunctional vascularity (neovascularisation — new vessels grow in but are abnormal and associated with pain nerve ingrowth)
- Initiated by microscopic tearing of the tendon in response to repetitive load
Repetitive overload → microtears → failed healing response → abnormal collagen remodelling (type III replacing type I) → disorganised, weak tendon matrix → neovascularisation with nociceptive nerve ingrowth → chronic pain cycle
Loading Principles — How to Strengthen a Tendinopathy
Stage 1 — Isometric Loading (Pain Management Phase)
- Purpose: Reduce pain, maintain tendon stimulus without compression or dynamic stress
- Muscle contracts but no joint movement (e.g. wall sit, isometric calf raise against a step)
- High intensity, low repetition (e.g. 5 × 45 sec holds)
- Can be done daily — isometrics have an analgesic effect on tendon pain
Stage 2 — Heavy Slow Resistance (HSR)
- Purpose: Stimulate type I collagen production and reorganisation
- Slow, controlled concentric AND eccentric movements through full range
- e.g. 3–4 sets × 8–15 reps, 3× per week
- Progressively increase load over weeks
- This is where eccentric loading has historically shown the highest success rates for tendinopathy
Stage 3 — Energy Storage (Stretch-Shortening Cycle)
- Purpose: Restore spring-like tendon function
- Introduces speed — e.g. double-leg calf raises with a bounce, step-ups, low-level plyometrics
- Only introduced once pain is well-controlled at rest and with slow loading
Stage 4 — Return to Sport / High Load
- Running, jumping, sport-specific training
- Volume and intensity managed carefully to avoid recurrence
"Heavy-load eccentric strengthening has demonstrated the highest success rate" for noninsertional Achilles tendinopathy. — Miller's Review of Orthopaedics
Patellar and Achilles tendinopathy management: "physical therapy focused on eccentric exercises" is the mainstay. — ROSEN's Emergency Medicine
Achilles Tendinopathy
Noninsertional (mid-portion) — ~50% of cases
- Site: 2–6 cm proximal to calcaneal insertion (watershed zone)
- Fusiform thickening at this zone, pain with activity
- MRI: thickened tendon with intrasubstance intermediate signal
- Loading: Heavy-load eccentric strengthening (Alfredson protocol) — heel drops off a step, full range, with load; 3×15 twice daily
- Also: activity modification, heel lifts, physiotherapy (massage, US, iontophoresis), ESWT
- Responds conservatively in ~50–70% of cases
Insertional — ~25% of cases
- Site: at the calcaneal attachment
- May be associated with Haglund deformity (prominent superior calcaneal tuberosity)
- Radiograph: posterior calcaneal enthesophyte, intratendinous calcification
- Loading: Eccentric exercises are modified — heel drops done on flat ground (not off a step) to avoid compression at the insertion; heavy slow resistance preferred
- Heel lifts, silicone heel pads, shoe modification
- Avoid steroid injections — associated with rupture risk
- Responds conservatively in ~50–70% of cases
Patellar Tendinopathy ("Jumper's Knee")
- Mechanism: Repetitive tensile overload at the patellar tendon, especially with running and jumping sports
- Microscopic tears → inflammatory cascade → chronic cellular changes
- Presentation: Gradual onset anterior knee pain localised to the patellar tendon, typically at the inferior pole of the patella; tenderness on palpation
- Standard x-ray: rule out avulsion fractures, check for patella alta
- Red flags to exclude rupture: traumatic mechanism, palpable defect, inability to straight leg raise
- Isometrics first: Leg press at 60° knee flexion, wall sits — strong analgesic effect, critical for painful early phase
- HSR: Squats (bilateral → single leg), leg press, Spanish squat — slow and heavy (3–4 × 8 reps)
- Eccentric focus: Slow single-leg decline squat (25° decline board reduces patellar tendon load at the proximal insertion) — the decline squat is the gold-standard eccentric exercise for patellar tendinopathy
- Energy storage: Jump progressions when pain-free with slow loading
- No role for steroid injection in patellar tendinopathy
- Surgery (débridement) reserved for recalcitrant cases
Tibialis Posterior Tendinopathy
- The most commonly affected posteromedial ankle tendon, with ~2× the cross-sectional area of flexor digitorum longus
- Critical role: maintains the medial longitudinal arch and performs ankle plantar flexion and inversion; works with the spring ligament
- Repetitive overload with pronated/flat-foot mechanics (overpronation forces eccentric overload)
- Middle-aged women disproportionately affected
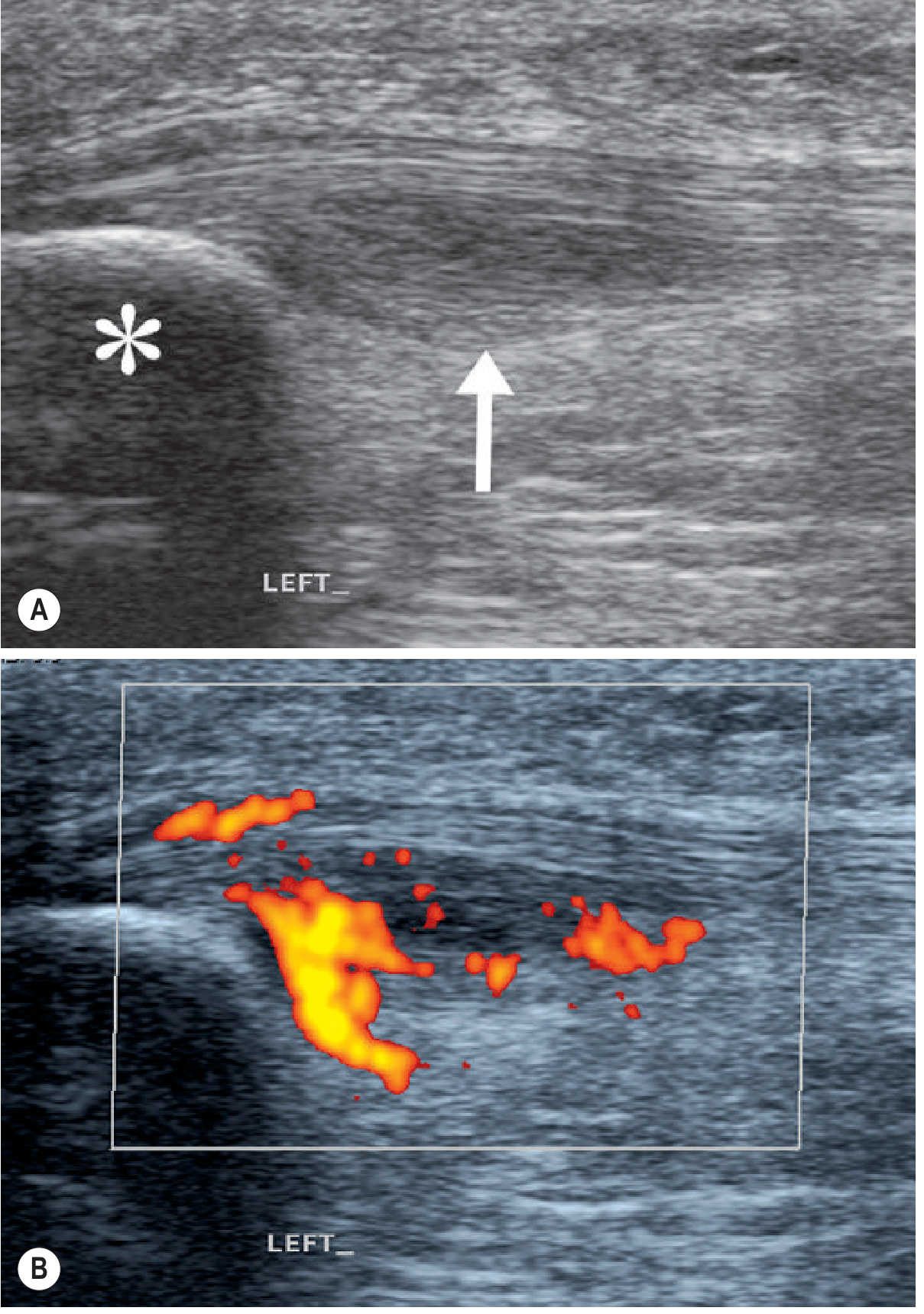
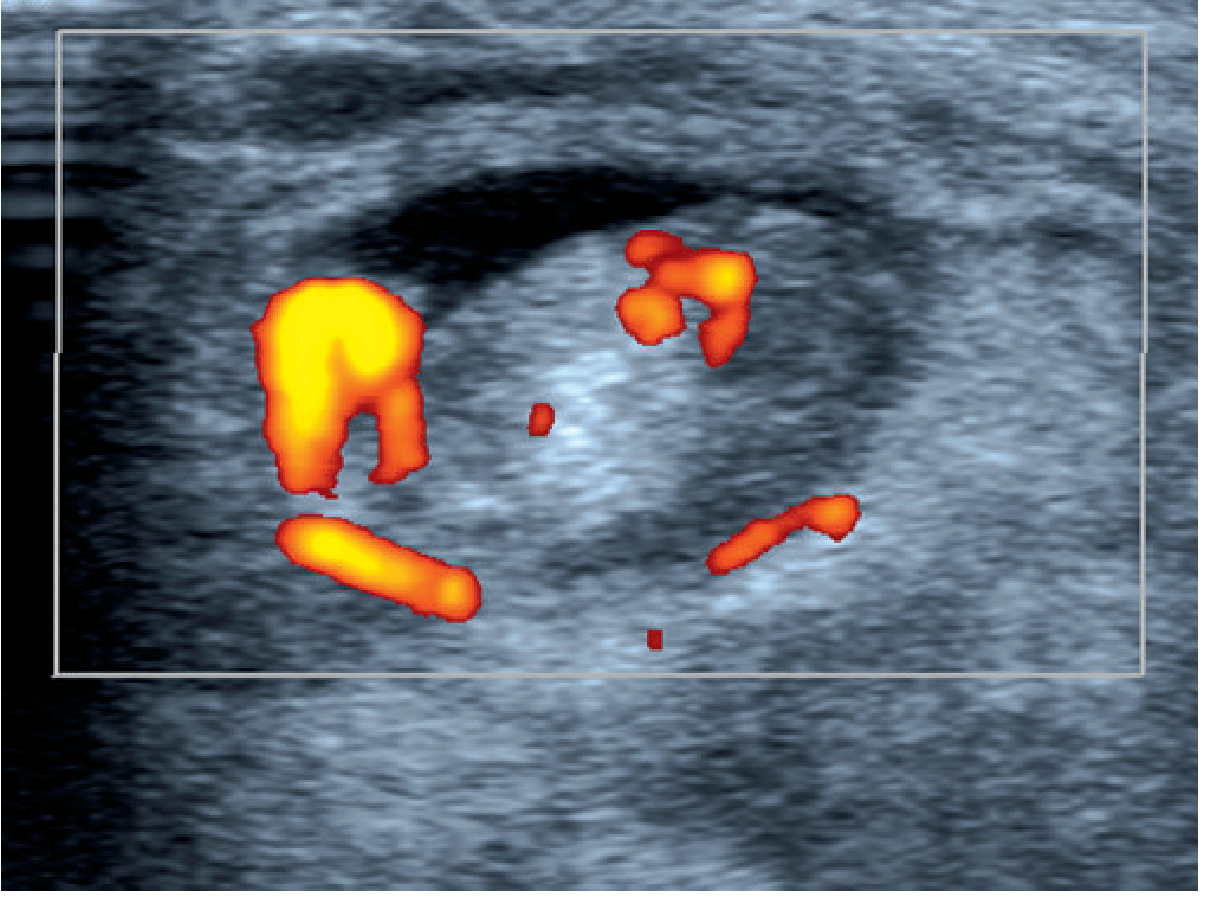
- Tenosynovitis is common — fluid in the tendon sheath with hypervascular changes on Doppler ultrasound
- Medial ankle pain (posterior to medial malleolus)
- Gradual flat foot deformity develops as the tendon fails
- Classic test: inability to perform single-leg heel raise (or painful/limited compared to the other side)
- Progressive: unopposed peroneus brevis causes exaggerated eversion → pes planus
- Isometrics: Resisted ankle inversion in neutral — towel or band, sustained holds
- HSR: Heel raise with inversion emphasis on calf raise machine or using a decline board; resisted inversion with theraband, progressing to single-leg calf raises
- Single-leg heel raise progressions — the key functional exercise; start bilateral, progress to unilateral with load
- Foot intrinsic strengthening and arch control work alongside tendon loading
- Medial arch support/orthoses to offload the tendon during rehabilitation
- PRICE in acute phase; physiotherapy for tendinopathy
- Orthopedic referral if tendon rupture suspected (loss of heel raise, progressive flatfoot)
Summary Table
| Tendon | Classic Site | Key Test | Primary Exercise |
|---|---|---|---|
| Achilles (noninsertional) | 2–6 cm above insertion | Pain with calf raise, fusiform swelling | Eccentric heel drop off step |
| Achilles (insertional) | At calcaneus | Posterior heel pain with direct pressure | Flat eccentric heel drop / HSR |
| Patellar | Inferior pole of patella | Palpation tenderness, pain with jumping | Decline single-leg squat (eccentric) |
| Tibialis posterior | Posteromedial ankle | Single-leg heel raise | Single-leg heel raise + resisted inversion |
what is achilles tendinopathy
Achilles Tendinopathy
What Is It?
Two Distinct Types
1. Noninsertional (Mid-portion) — ~50% of cases
- Location: 2–6 cm proximal to the calcaneal insertion (a relative watershed zone with poor blood supply)
- The most common type
2. Insertional — ~25% of cases
- Location: at the calcaneal attachment itself
- Often associated with a Haglund deformity (bony prominence on the back of the heel) and intratendinous calcification
Pathology
- Disorganised and degenerated collagen fibres (type III replaces type I)
- Mucoid degeneration of the matrix
- Minimal inflammatory cells (macrophages, plasma cells — not neutrophils)
- Neovascularisation — abnormal new vessels grow in, accompanied by nociceptive nerve fibres (this is a key driver of chronic pain)
- Initiated by microscopic tearing of tendon fibres in response to repetitive load beyond the tendon's capacity
Who Gets It?
- Overuse / sudden training load increase
- Mechanical imbalance (tight gastrocnemius-soleus complex, poor foot mechanics)
- Poor tissue vascularity
- Genetic predisposition
- Age (tissue quality declines)
- Fluoroquinolone antibiotic use (e.g. ciprofloxacin) — independent risk factor
- Systemic conditions: diabetes, rheumatoid arthritis, chronic renal failure
Presentation
- Posterior heel/lower leg pain, swelling, stiffness — typically worse first thing in the morning and at the start of activity, then may ease with warm-up before worsening again
- Pain worsened by push-off activities: running, stairs, hills, jumping
- On examination:
- Tenderness to palpation over the tendon
- Fusiform (spindle-shaped) swelling at the mid-portion (noninsertional), or thickening/tenderness at the heel insertion (insertional)
- "Wet crepitus" may be felt (fluid in the peritenon)
- Reduced strength on single-leg calf raise — can't perform repeated repetitions without pain
Investigations
- Radiographs not routinely needed early; used in chronic cases to identify calcific deposits, Haglund deformity, or enthesophyte at insertion
- Ultrasound / MRI — used to assess extent of degeneration, confirm diagnosis, or rule out partial/complete tear; note that imaging changes can persist even after clinical recovery
Management
Conservative (first line — effective in ~50–70% of cases)
| Approach | Detail |
|---|---|
| Relative rest + activity modification | Reduce provocative loading, maintain general fitness |
| Heel lifts | Offload the tendon, especially useful insertional |
| Eccentric strengthening (Alfredson protocol) | Heel drops off a step, slow and loaded, 3×15 twice daily — highest success rate for noninsertional disease |
| Heavy slow resistance (HSR) | Preferred for insertional — slow bilateral/single-leg calf raises on flat ground (avoids calcaneal compression) |
| ESWT (extracorporeal shockwave therapy) | Adjunct for recalcitrant cases |
| Physiotherapy modalities | Massage, therapeutic ultrasound, iontophoresis |
| Ice / NSAIDs | Short-term pain relief |
| Glyceryl trinitrate patches, prolotherapy | Evolving evidence |
Surgical (recalcitrant cases only)
- Noninsertional: Percutaneous longitudinal tenotomy, stripping of anterior tendon, isolated gastrocnemius recession (if contracture present), or open excision of degenerated tissue
- Insertional: Excision of retrocalcaneal bursa, resection of Haglund prominence, débridement of calcification; if >50% tendon detached → FHL tendon transfer; Zadek calcaneal osteotomy for bony mechanical issues
Key Points to Remember
- Degenerative, not primarily inflammatory — "tendinopathy" not "tendinitis"
- Two sites: mid-portion (2–6 cm up) vs insertional (at calcaneus) — different exercise approaches
- Eccentric loading is the cornerstone of rehab
- Avoid corticosteroid injection
- Thompson test rules out full rupture
what is patella tendinopathy
Patellar Tendinopathy ("Jumper's Knee")
What Is It?
Where Does It Occur?
Who Gets It?
- Athletes in jumping sports: basketball, volleyball, high jump, netball
- Runners
- Can occur in any repetitive loading occupation or activity
- Adolescents and young adults most commonly affected
- Skeletally immature patients presenting with pain at the distal pole of the patella may have Sinding-Larsen-Johansson disease (avulsion apophysitis at the distal patellar pole) rather than true tendinopathy
Pathology
- Repetitive tensile overload → microscopic tears in tendon fibres
- Failed healing → central degeneration of collagen (tendinosis)
- Disorganised type III collagen replaces type I
- Neovascularisation — new abnormal vessels grow into the tendon along with nociceptive nerve fibres → chronic pain
- Minimal true inflammation
- Ultrasound: Hypoechoic (dark) area in the deep central proximal tendon, tendon thickening, Doppler shows neovascularisation (orange signal)
- MRI: Focal increased fluid signal and thickening at the proximal attachment; increased vascularity
Note: Some asymptomatic jumping athletes have the same imaging findings — prognosis and outcomes are not predicted by imaging alone.
Presentation
- Gradual onset anterior knee pain localised to the patellar tendon (typically the inferior pole of the patella)
- Pain pattern: initially after activity → progresses to pain during activity → in severe cases, pain at rest
- Tenderness on direct palpation of the patellar tendon, most often at the inferior patellar pole
- Pain reproduced/worsened by activities loading the extensor mechanism: squatting, stairs, jumping, landing
- No joint effusion (distinguishes it from intra-articular pathology)
- Traumatic mechanism
- Palpable defect in the tendon
- Inability to perform a straight leg raise
Differential Diagnosis
| Condition | Key Feature |
|---|---|
| Patellofemoral syndrome | Pain "behind" or "around" patella, worse with stairs/prolonged sitting |
| Patellar tendon rupture | Traumatic, palpable defect, can't SLR |
| Osgood-Schlatter disease | Adolescent, pain/swelling at tibial tubercle |
| Sinding-Larsen-Johansson | Adolescent, pain at distal pole of patella |
| Chondromalacia patellae | Cartilage damage, pain with sustained flexion |
Investigations
- X-ray (standard knee views): rule out avulsion fractures, assess for patella alta (high-riding patella — a predisposing factor)
- Ultrasound / MRI: confirm tendon thickening, degeneration, neovascularisation — used as an adjunct, not standalone diagnostic tool
Management
Conservative (first line)
- Relative rest — reduce provocative activity (jumping, heavy squatting) but don't stop all exercise
- Identify and modify training errors
- Decline board single-leg squat (25° decline): the gold-standard eccentric exercise for patellar tendinopathy — the decline reduces patellar tendon load at the proximal attachment and isolates the tendon eccentrically
- Start with: 3 × 15 reps, slow and controlled, pain ≤ 3–4/10 acceptable
- Progress to loaded (weighted vest/backpack) as tolerated
- Isometric holds first if pain is high: wall sit or leg press at 60° knee flexion, 5 × 45 sec — reduces pain acutely
- Progress to heavy slow resistance squats (bilateral → single leg)
- Hamstring stretching — tight hamstrings increase compressive load on the patellar tendon
- Quadriceps strengthening — address underlying weakness
- Counterforce brace (infrapatellar strap / Cho-Pat strap) — can reduce symptoms by altering patellar tendon mechanics
- Deep friction massage, therapeutic ultrasound, prolotherapy, PRP — mixed evidence, no RCTs prove efficacy
- No corticosteroid injection — highly discouraged; predisposes to complete tendon rupture
- Avoid aggressive stretching into full knee flexion in acute phase
Surgical (recalcitrant cases only)
- Débridement of the degenerative tendinosis tissue
- Reserved for cases that fail 3–6+ months of structured conservative rehabilitation
Key Points
- Degenerative (tendinosis), not inflammatory — avoid steroid injections
- Most common site: deep central fibres at inferior patellar pole
- Hallmark exercise: decline single-leg squat (eccentric)
- Isometrics (wall sit/leg press) are useful for pain management early on
- Imaging confirms diagnosis but doesn't determine prognosis
- Rule out rupture if trauma + palpable defect + inability to SLR
what is tibialis posterior tendinopathy
Tibialis Posterior Tendinopathy
What Is It?
Anatomy — Why It Matters
- Originates from the proximal two-thirds of the tibia, fibula, and interosseous membrane
- Travels behind the medial malleolus (which acts as a pulley), held in place by the flexor retinaculum
- Primary insertion: navicular tuberosity; also sends slips to the cuneiforms, bases of 2nd–4th metatarsals, cuboid, and sustentaculum tali
- Is the largest and strongest of the three medial compartment tendons (~2× the cross-sectional area of flexor digitorum longus)
- Primary functions: plantar flexion and inversion of the foot
"The tibialis posterior tendon and the spring ligament are crucial structures supporting the medial arch of the foot." — Imaging Anatomy, Bones, Joints, Vessels and Nerves
Who Gets It?
- Middle-aged women are disproportionately affected
- Overweight/obese individuals (arch overload)
- Athletes with repetitive loading (running, dancing)
- Inflammatory arthropathies: rheumatoid arthritis particularly
- Accessory navicular bone — can alter tendon mechanics at the insertion
- Chronic overuse / training errors
- Hypovascularity at the zone 2–6 cm proximal to insertion
- Overload of the arch from activity or obesity
- Inflammatory disorders (RA)
- Gastrocnemius/soleus contracture (tight calf complex increases tensile demand on the tendon)
Pathology
- Repetitive loading → microtears → failed collagen remodelling → tendinosis (disorganised collagen, degeneration, minimal inflammation)
- Tenosynovitis: fluid accumulates in the tendon sheath with hypervascularity on Doppler
- Progressive tendon degeneration → functional incompetence → loss of arch support
- Unopposed peroneus brevis (the functional antagonist) causes progressive hindfoot valgus and forefoot abduction → flat foot (pes planus)
- The spring (calcaneonavicular) ligament — the primary static stabiliser of the talonavicular joint — also becomes stressed and can fail alongside the tendon, accelerating deformity
Staging (Johnson & Strom — important clinically)
| Stage | What's Happening | Deformity |
|---|---|---|
| Stage I | Tenosynovitis; tendon intact, normal strength | No deformity |
| Stage II | Tendon degenerated, functionally incompetent | Flexible flatfoot; hindfoot valgus correctable |
| Stage III | Tendon rupture; fixed deformity | Rigid flatfoot; cannot correct hindfoot |
| Stage IV | As III + valgus tilt of the talus in the ankle mortise | Ankle involved |
Presentation
- Medial ankle/foot pain — early and predominant symptom, posterior and inferior to the medial malleolus
- Progressive arch collapse (flat foot developing over months to years)
- Lateral ankle pain develops late — from subfibular impingement as the heel drifts into valgus and the calcaneus abuts the fibula
- Asymmetric hindfoot valgus on standing examination
- Depressed medial arch
- Abducted forefoot
- "Too-many-toes" sign — viewed from behind the patient, more toes are visible on the affected side due to forefoot abduction
- Single-leg heel raise test: inability to perform a single-leg heel raise, or pain/weakness compared to the other side — the most important functional test. The PTT must fire to invert and lock the hindfoot to allow heel rise; failure to do so indicates PTT incompetence
- Tenderness to palpation along the tendon (posterior to medial malleolus down to navicular)
Investigations
- X-ray (weight-bearing):
- Talo-first metatarsal angle >4° = pes planus
- Reduced calcaneal pitch angle
- Loss of medial cuneiform–floor height
- Lateral hindfoot: assess for subfibular impingement
- Ultrasound:
- Tenosynovitis: fluid in the sheath + neovascularisation on Doppler
- Tendon thickening, hypoechoic changes, tears
- MRI:
- Greater CSA of fluid than tendon = tenosynovitis
- Intrasubstance signal change = tendinosis
- Partial/complete tears
Management
Conservative (Stage I and II first line)
- Immobilisation (cast or walking boot) to offload the tendon acutely
- Orthotics (arch support + medial heel wedge) once acute pain settles
- PRICE: protect, relative rest, ice, compression, elevation
- AFO (ankle-foot orthosis) + physical therapy — has demonstrated the highest success rate for stage II
- Full-length orthotic with arch support, medial heel wedge, medial forefoot support
- Lace-up ankle brace as an alternative
- Isometrics first: Resisted ankle inversion in neutral (towel/theraband) — sustained holds
- Heavy slow resistance:
- Bilateral calf raises (heel raise with inversion emphasis) → progress to single-leg
- Resisted inversion with theraband progressing to heavier resistance
- Tibialis posterior isolation exercises on a bench or using resistance bands
- Single-leg heel raise — the functional gold-standard exercise; start bilateral, progress to unilateral, add load (backpack/weighted vest)
- Foot intrinsic strengthening — short foot exercises, toe gripping
- Gastrocnemius/soleus stretching — calf tightness is very commonly present and increases load on the PTT; address this concurrently
- Medial arch control — orthotics worn during all rehab and daily activity to protect the tendon while it recovers
Surgical (Stage II failing conservative, Stage III, Stage IV)
| Stage | Surgery |
|---|---|
| Stage I | Tenosynovectomy |
| Stage II | FDL (or FHL) tendon transfer to navicular + calcaneal osteotomy (medial slide for IIA; lateral column lengthening for IIB) ± spring ligament reconstruction ± gastrocnemius recession |
| Stage III | Double or triple hindfoot arthrodesis (subtalar ± talonavicular ± calcaneocuboid) |
| Stage IV | Triple arthrodesis + address ankle valgus |
Key Points
- PTTD is the most common cause of adult-acquired flatfoot
- Spectrum: tenosynovitis → tendinosis → rupture → fixed deformity
- Classic triad: medial ankle pain + flatfoot + inability to single-leg heel raise
- "Too-many-toes" sign viewed from behind
- Hypovascularity zone 2–6 cm proximal to navicular = most vulnerable area
- Stage II = flexible deformity (correctable) — most amenable to conservative rehab
- Stage III = rigid deformity — requires arthrodesis
- Single-leg heel raise is both the diagnostic test and the key rehab exercise
magnusson tendon collagen synthesis paper- summarise it
Magnusson et al. — Tendon Collagen Synthesis
Core Argument
Key Findings and Concepts
1. Tendon collagen turnover is slow but load-responsive
- The tendon core collagen has a half-life of approximately 100 years in adults — meaning the structural collagen laid down early in life is barely replaced
- However, a small metabolically active collagen pool does respond to mechanical loading
- Acute loading (exercise) triggers a transient increase in collagen synthesis lasting ~24–72 hours, followed by a return to baseline
2. Net collagen balance after loading
- After a single bout of mechanical loading, both synthesis AND degradation increase
- In young healthy tendons, synthesis outpaces degradation → net collagen gain
- The key finding: in tendinopathic tendons, this balance is disrupted — degradation may exceed or match synthesis, leading to net collagen loss and tissue deterioration
3. The "failed healing response" model
- Magnusson and Kjaer argue tendinopathy is best understood as a failed or dysregulated repair response, not chronic inflammation
- Repetitive microtrauma exceeds the tendon's capacity to synthesise new collagen → accumulation of damage
- Tenocytes (tendon cells) change their phenotype and begin producing type III collagen (weaker, disorganised) instead of type I
4. Regional heterogeneity within the tendon
- Peritendinous tissue (the outer envelope) has a much faster collagen turnover than the tendon core
- Most of the measurable acute collagen synthesis response occurs in the peritendinous tissue, not the core
- This distinction has implications: the core structural tendon is largely metabolically inert in adults, making true remodelling very slow and limited
5. Vascular and neurogenic contributions
- Tendinopathic tendons show neovascularisation with accompanying sympathetic nerve ingrowth
- These new vessels and nerves are associated with pain but do not effectively restore tissue nutrition or healing capacity
- Intratendinous vascularity remains poor despite neovascularisation
6. Implications for loading as treatment
- Because collagen synthesis is load-dependent, mechanical loading remains the most potent stimulus for driving adaptive collagen synthesis
- This provides the biological rationale for eccentric and heavy slow resistance loading in tendinopathy rehabilitation
- Load must be sufficient to stimulate synthesis but not so excessive as to outpace the tendon's repair capacity — this is the therapeutic window
Clinical Relevance
| Concept | Clinical implication |
|---|---|
| Slow core collagen turnover | Full tendon remodelling takes months–years; set realistic timelines |
| Load stimulates synthesis | Progressive loading is essential — rest alone is counterproductive |
| Net balance disrupted in tendinopathy | Need to tip balance back toward synthesis > degradation |
| Type III replaces Type I | Explains biomechanical weakness; why tendinopathic tendon is rupture-prone |
| Peritendinous turnover faster than core | Peritendinous healing is quicker; intratendinous damage is harder to reverse |
Limitations Acknowledged
- Most synthesis data came from microdialysis studies measuring peritendinous collagen markers (procollagen type I C-terminal propeptide, PICP) — may not fully reflect intratendinous changes
- Translating acute synthesis responses to long-term structural adaptation is not straightforward
- Individual variation in tenocyte response to loading is significant
Bottom Line
"The challenge is not to avoid loading the tendon, but to find the right amount of load to drive repair without perpetuating damage."
give me 5 exercises for post tib tendon dysfunction
1. Isometric Tibialis Posterior (Resisted Inversion Hold)
2. Seated Resisted Inversion with Theraband
3. Double-Leg Heel Raise (with inversion emphasis)
4. Single-Leg Heel Raise
5. Step-Down / Decline Single-Leg Squat with Inversion Control
Important Notes
| Point | Detail |
|---|---|
| Orthotics | Wear medial arch support + heel wedge during all exercises — reduces tendon strain while it's being loaded |
| Calf stretching | Do gastrocnemius and soleus stretches daily — tightness is almost universal and increases tensile demand on the PTT |
| Pain guide | Pain ≤ 3–4/10 during exercise is acceptable; pain that remains elevated the next morning = too much load, reduce |
| Progression | Only progress to the next exercise when the current one is pain-free and strong |
| Timeframe | Expect 3–6 months for meaningful tendon adaptation — set realistic expectations |
exercise with both feet on tiptoes and exercise with foot inverting
Exercise 1 — Bilateral Heel Raise (Both Feet on Tiptoes)
What It Is
How to Do It
- Stand with feet hip-width apart, toes pointing forward
- Light fingertip contact with a wall or chair for balance only — do not lean or push through hands
- Wear orthotics/arch support if prescribed
- Slowly rise up onto tiptoes — 2 seconds up
- At the top, squeeze slightly inward (gentle supination/inversion at the top of the raise) — this is the cue that actively engages tibialis posterior
- Hold at the top for 2 seconds
- Lower slowly back to the floor — 3 seconds down (this eccentric lowering phase is the most important part)
- Full foot contact with the floor before next rep — do not bounce
- 3 sets × 15 repetitions
- 3 times per week (allow a day's rest between sessions)
- Rest 60–90 seconds between sets
Progressions
| Stage | How to Progress |
|---|---|
| Too easy | Add a weighted backpack / hold dumbbells |
| Next step | Progress to single-leg heel raise (one foot at a time) |
| Further | Stand on a step edge so the heel drops below the step level — increases range |
What Tibialis Posterior Is Doing
Common Errors
- Rising too fast — the slow lowering is where the tendon loading occurs; do not rush the descent
- Allowing the ankles to roll outward or inward instead of straight up
- Gripping the wall/chair instead of using it only for balance
- Feet too wide or toes pointed out — changes the mechanics
Exercise 2 — Resisted Foot Inversion (Theraband)
What It Is
How to Do It
- Sit on a chair or bench with the foot off the floor, knee at about 90°
- Foot in slight plantar flexion (pointed slightly down) — this is the position where tibialis posterior is most active
- Loop a theraband around the forefoot (not just the toes)
- Anchor the other end to the opposite foot, a table leg, or a fixed point on the medial side so the band pulls the foot into eversion (outward) — your job is to resist this and move into inversion (inward)
- Start with foot in a neutral/slightly everted position
- Slowly turn the foot inward (inversion — sole turns to face the other foot)
- Hold for 2 seconds at end range
- Slowly return to start — 3 seconds back
- Do not let the band snap the foot back — control the return
- 3 sets × 15 repetitions
- 3 times per week
- Rest 60 seconds between sets
Progressions
| Stage | How to Progress |
|---|---|
| Too easy | Use a heavier resistance band (thicker/stiffer) |
| Next stage | Perform standing with band — adds body weight component |
| Further | Combine with single-leg standing — foot inversion control during balance |
What Tibialis Posterior Is Doing
Common Errors
- Moving from the knee rather than the ankle/foot — the lower leg should stay still, only the foot moves
- Going too fast — slow and controlled throughout
- Using too strong a band early — better to start light and nail the technique
- Anchoring the band in the wrong direction — it must pull the foot outward (into eversion) so you are working against it
How These Two Exercises Fit Together
| Bilateral Heel Raise | Resisted Inversion | |
|---|---|---|
| Load level | Higher — body weight | Lower — band resistance |
| Position | Standing, functional | Seated, isolated |
| When to use | When pain allows standing load | Early stage, or as warm-up before heel raise |
| What it trains | Functional arch locking, push-off | Direct tendon strength, isolated |
| Key phase | Slow eccentric lowering | Slow controlled return |
standing and inverting foot exercise
Standing Foot Inversion Exercise
What It Is
Setup
- Stand on the affected foot with a slight bend in the knee (10–15°) — do not lock the knee straight
- Loop a theraband around the forefoot of the standing foot
- Anchor the band to a fixed point on the lateral/outer side (e.g. a table leg, door frame, or heavy piece of furniture) — so the band is pulling your foot outward into eversion
- Light fingertip contact with a wall for balance if needed
- Wear your orthotics/arch support
The Movement
- Start with foot flat on the floor in a neutral position
- Lift the arch — press the big toe down and roll the foot slightly inward, inverting against the band's pull
- Hold for 2 seconds at end range
- Slowly return the foot to neutral — 3 seconds back
- Do not let the band pull the foot into eversion — you control the return
Prescription
- 3 sets × 12–15 repetitions
- 3 times per week
- Rest 60–90 seconds between sets
What Tibialis Posterior Is Doing
| Job | What's happening |
|---|---|
| Dynamic | Inverting the foot against the band |
| Stabilising | Maintaining the medial arch and controlling hindfoot valgus during single-leg stance |
What to Watch For
- Arch lifting/maintaining during the movement
- Smooth, controlled inversion and return
- Knee tracking over the 2nd toe — not collapsing inward
- Stable pelvis — not dropping to one side
- Arch collapsing downward instead of lifting — the whole foot pronating rather than the forefoot inverting
- Rotating the whole lower leg inward instead of isolating foot movement
- Rushing the return phase — the slow eccentric return is where most of the tendon loading benefit comes from
- Leaning heavily on the wall — only fingertip contact for balance
Progressions
| Stage | Modification |
|---|---|
| Too easy | Heavier resistance band |
| Next step | Perform on an unstable surface (balance board or folded towel) — increases demand on tendon stabilisation |
| Further | Combine with a mini squat — invert as you lower into a slight squat, return as you rise — integrates full chain |
| Advanced | Add a small hop or step and land with arch control — sport-specific preparation |
How It Fits in the Programme
Seated resisted inversion → Standing resisted inversion → Single-leg heel raise
(isolated, non-weight bearing) (functional, weight bearing) (full body weight load)
single heel raise
Single-Leg Heel Raise
What It Is
Why It Is So Important for PTTD
- Tibialis posterior fires to lock the subtalar joint into inversion — converting the foot from a mobile adaptor into a rigid lever
- The medial arch lifts and stiffens
- The calf (gastrocnemius/soleus) then generates the heel rise force through a now-rigid foot
- The heel stays in valgus (rolls outward) instead of inverting
- The arch collapses
- The heel rise is weak, painful, or impossible entirely
Setup
- Stand barefoot or in orthotics (orthotics recommended during rehab)
- Stand on the affected foot only
- Slight bend in the knee (10–15°) — never lock the knee straight
- Light fingertip contact with a wall for balance only — do not push through it
- Non-standing foot slightly lifted off the ground, held behind you
The Movement
- Slowly rise onto the ball of the foot/tiptoes — 2–3 seconds up
- At the top, check:
- Heel should be slightly inverted (tilted inward) — this is correct tibialis posterior activation
- Arch should be lifted, not collapsed
- If the heel stays in valgus (falls outward) at the top — tibialis posterior is not locking the joint
- Hold at the top — 2 seconds
- Slowly lower back to the floor — 3–4 seconds down
- This eccentric lowering phase is where the greatest tendon loading and collagen synthesis stimulus occurs — do not rush it
- Full foot contact before next rep — no bouncing
Prescription
| Variable | Detail |
|---|---|
| Sets | 3 sets |
| Reps | Start with 8–10; build to 15 |
| Tempo | 2 sec up / 2 sec hold / 3–4 sec down |
| Frequency | 3× per week (rest day between sessions) |
| Rest | 90 seconds between sets |
Pain Guide
| Pain level during exercise | Action |
|---|---|
| 0–3/10 | Continue — acceptable loading |
| 4–5/10 | Reduce reps or use lighter load |
| >5/10 | Stop — too much load; regress to bilateral heel raise |
| Elevated pain next morning | Too much — reduce volume next session |
What to Watch For
- Heel inverts slightly at the top of the rise
- Arch lifts — does not collapse inward
- Smooth, controlled descent — no sudden drop
- Knee tracks over 2nd toe throughout
- Heel staying in valgus at top — tibialis posterior not activating; cue "roll the heel slightly inward as you rise"
- Arch collapsing — foot pronating throughout the movement; cue "press your big toe into the floor"
- Pushing through the wall — makes the exercise easier and defeats the purpose; fingertips only
- Dropping too fast — the slow lowering is the key loading phase; count it out loud if needed
- Knee caving inward — cue "keep your knee over your second toe"
Progressions
| Stage | How |
|---|---|
| Too difficult | Regress to bilateral heel raise; use hands lightly on a surface |
| Baseline | Single-leg heel raise, bodyweight only |
| Progress 1 | Increase reps to 15, then 20 |
| Progress 2 | Add load — wear a weighted backpack or hold a dumbbell |
| Progress 3 | Perform off a step edge — heel drops below step level, increasing range of motion and loading demand |
| Progress 4 | Remove wall contact entirely — balance challenge increases tibialis posterior stabilisation demand |
| Return to sport benchmark | 25+ consecutive single-leg heel raises, pain-free, with good heel inversion at the top |
Step-Edge Variation (Advanced)
- Lower the heel below step level first (controlled dorsiflexion stretch)
- Then rise to tiptoe fully
- Slow controlled return below step level again
Where It Sits in the Programme
Isometric inversion holds
↓
Seated resisted inversion (band)
↓
Standing resisted inversion (band, weight-bearing)
↓
Bilateral heel raise (both feet)
↓
Single-leg heel raise ← YOU ARE HERE
↓
Single-leg heel raise off step edge
↓
Return to running / sport