Give an essay answer type response for cernea classification in thyroid for Ent post graduation exam by referring standard textbooks and online articles , it’s significance
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative surgical textbooks. Let me compose a detailed essay-type answer.
Cernea Classification of the External Branch of the Superior Laryngeal Nerve (EBSLN) in Thyroid Surgery
Introduction
The superior laryngeal nerve (SLN) arises from the vagus nerve at the base of the skull and descends along the internal carotid artery before dividing at the level of the hyoid bone into two branches:
- Internal branch — sensory to the supraglottic larynx and laryngeal mucosa above the vocal cords
- External branch (EBSLN) — motor to the cricothyroid muscle and inferior pharyngeal constrictor
The EBSLN is the "nerve of the singing voice." It is the sole motor supply to the cricothyroid muscle — the tensor of the vocal cord — which controls pitch, voice projection, and the ability to sustain high-frequency phonation. Its surgical relevance in thyroid operations cannot be overstated, as it travels in intimate proximity to the superior thyroid pole vessels before reaching its target muscle.
The anatomical variability in the course of this nerve and its relationship to the superior thyroid artery was systematically described by Cernea and colleagues in 1992, leading to the eponymous classification that is now the standard reference for thyroid surgeons worldwide.
Anatomy of the EBSLN Relevant to Thyroid Surgery
The EBSLN descends from the common SLN trunk and runs along the lateral surface of the inferior pharyngeal constrictor muscle, traveling cephalad to caudad lateral to the superior thyroid vascular pedicle. It then crosses the superior thyroid artery in a medial direction to enter and innervate the cricothyroid muscle. This oblique medial crossing — and specifically the point at which it occurs relative to the superior pole of the thyroid — defines the surgical risk zone.
The superior thyroid artery, the first branch of the external carotid artery, divides into anterior and posterior branches at the apex of the thyroid lobe. The EBSLN crosses this artery (or its branches) at a variable level. In large, ptotic, or multi-nodular goitres, the nerve may descend even lower, bringing it into greater jeopardy during superior pole ligation.
The Cernea Classification
Cernea et al. studied 33 cadaveric necks and 28 surgical patients, establishing a practical anatomical classification based on the relationship of the EBSLN to the superior thyroid pole and the superior thyroid vessels (measured at a 1 cm reference above the upper border of the thyroid pole).
Type 1
The EBSLN crosses the superior thyroid vessels ≥ 1 cm above the superior border of the thyroid lobe.
- The nerve is well away from the superior pole dissection zone
- Lowest risk of inadvertent injury during superior pole mobilisation
- Incidence: approximately 50–75% of individuals
Type 2A
The EBSLN crosses the superior thyroid vessels within 1 cm above the superior border of the thyroid superior pole (i.e., < 1 cm above the upper edge of the pole, but still above it).
- The nerve is close to the vascular pedicle and lies within the surgical field during standard superior pole dissection
- Significantly higher risk of injury
- Incidence: approximately 18–20% of individuals
Type 2B
The EBSLN crosses the superior thyroid vessels at or below the superior border of the thyroid lobe — i.e., it descends behind the thyroid capsule itself.
- The nerve is completely buried within the dissection field, often not visible unless specifically sought
- Highest risk of injury — the nerve may be ligated en masse with the superior thyroid vessels if these are not divided individually close to the thyroid surface
- Incidence: approximately 6–7% of individuals; more common in patients with large or ptotic glands
Visual Reference
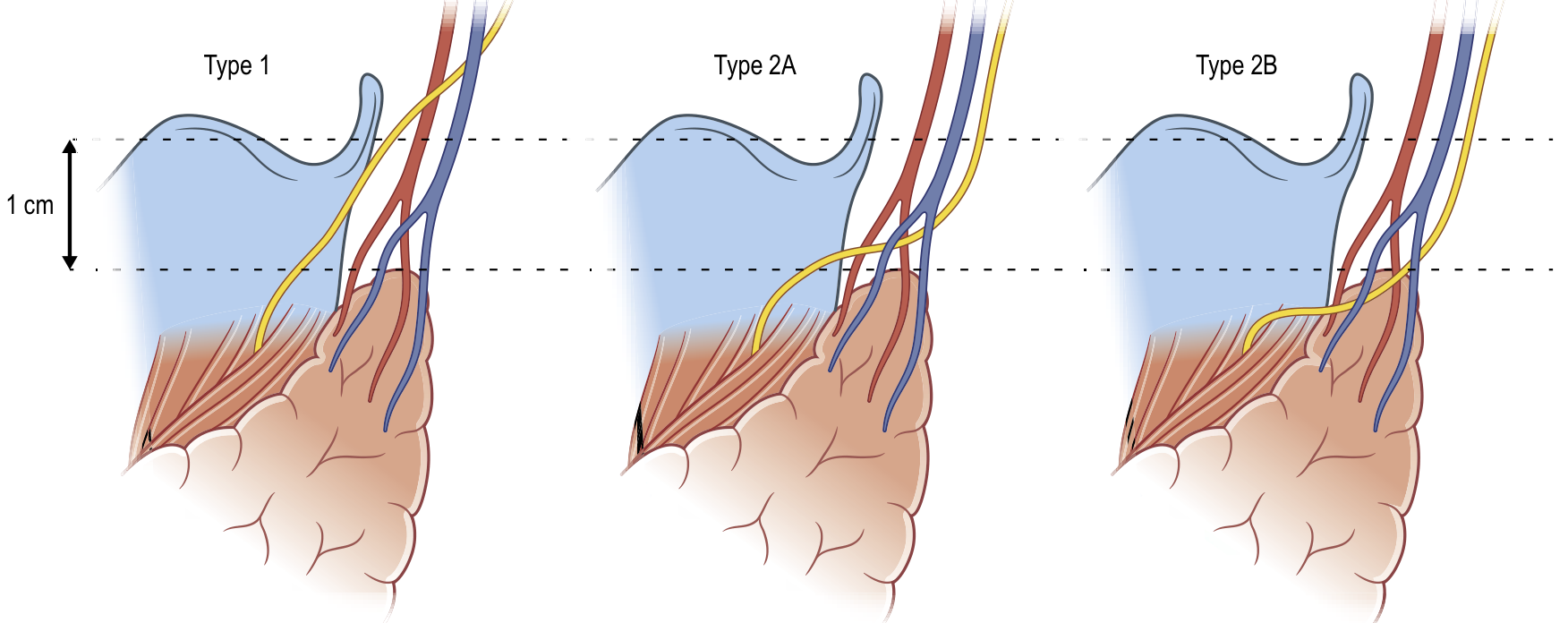
Cernea classification of the EBSLN. Type 1: nerve crosses > 1 cm above the superior pole. Type 2A: nerve crosses within 1 cm above the pole. Type 2B: nerve crosses below the border of the superior pole. Types 2A and 2B are most vulnerable during thyroidectomy. (From Gray's Surgical Anatomy, as reproduced in Current Surgical Therapy, 14e)
Some authors describe a modified or extended classification
The Kierner modification and subsequent refinements by other groups have proposed subdividing Type 2 further, but the original three-category Cernea system remains the most widely adopted in clinical practice and surgical exams.
Friedman's modification further delineates:
- Type 1 — crosses STA ≥ 1 cm above superior pole
- Type 2 — crosses within 1 cm above the pole or below it (unifying Cernea's 2A and 2B)
However, for purposes of surgical planning and examination, the Cernea three-type classification is standard.
Clinical Significance
1. Incidence of Injury
Injury to the EBSLN during thyroidectomy is the most common nerve injury in thyroid surgery and is often underreported because it does not cause the dramatic vocal cord palsy associated with RLN injury. Reported rates range from 0% (in meticulous dissections) to 58% (when the nerve is not specifically sought). With the Type 2B variant, routine en masse ligation of the superior pole is virtually guaranteed to injure the nerve.
2. Consequences of Injury
Injury to the EBSLN leads to cricothyroid muscle denervation, resulting in:
- Loss of ability to tense the ipsilateral vocal cord
- Inability to produce high-pitched sounds — difficulty "hitting high notes"
- Voice fatigue during prolonged speech
- Reduced voice projection and volume
- In professional voice users (singers, teachers, lawyers, clergy), the functional impairment can be career-ending
The classic test is the high-pitched "e" phonation — the affected patient cannot sustain a high-pitched note on the same side. Laryngoscopy may show subtle posterior glottic asymmetry and a low-lying arytenoid on the affected side.
3. Surgical Implications
The Cernea classification directly guides surgical technique:
a) Individual vessel ligation at the thyroid capsule: Rather than placing a mass ligature across the entire superior thyroid pedicle, each branch of the superior thyroid artery should be ligated individually, as close as possible to the thyroid capsule. This reduces the risk regardless of nerve type.
b) Space of Reeves: An avascular space exists between the medial superior pole and the cricothyroid muscle. Dissecting within this space (medially) allows the surgeon to skeletonise the superior pole vessels while the EBSLN remains safely lateral, hugging the constrictor muscle.
c) Avoid mass ligation: En masse ligation of the superior pole is particularly dangerous in Type 2B anatomy. The nerve, lying behind the thyroid capsule, may be caught in the ligature.
d) Intraoperative neuromonitoring (IONM): EMG-based IONM can help identify and preserve the EBSLN in real time, especially for Type 2A and 2B variants. EMG recordings from the cricothyroid muscle during stimulation help confirm nerve integrity before and after superior pole dissection.
e) Influence of pathology: A large or ptotic thyroid gland may drag the nerve inferiorly — effectively converting a Type 1 to a Type 2B-equivalent anatomy. Surgeons must be especially vigilant in goitre surgery, re-operations, and Graves' disease where the superior pole vasculature is engorged and the anatomy distorted.
4. Importance in Professional Voice Users
Preoperative identification of Cernea type (Type 2A/2B) through careful surgical planning and discussion of the risk with patients — especially professional voice users — is considered mandatory. Baseline voice assessment (perceptual analysis, laryngoscopy, voice range profile) is recommended pre- and post-thyroidectomy in high-risk cases.
Practical Points for ENT PG Examination
| Feature | Type 1 | Type 2A | Type 2B |
|---|---|---|---|
| Nerve level | ≥ 1 cm above superior pole | < 1 cm above superior pole | Below superior pole border |
| Surgical risk | Low | High | Highest |
| Frequency | ~50–75% | ~18–20% | ~6–7% |
| Key danger | — | En masse ligation | Buried behind capsule |
Key facts to remember:
- EBSLN innervates cricothyroid (only intrinsic laryngeal muscle supplied by SLN)
- All other intrinsic laryngeal muscles → RLN
- Injury → loss of high-pitched phonation, not hoarseness in the traditional sense
- Type 2B is the highest risk and most clinically relevant variant
- Prevention: individual vessel ligation, close to thyroid surface; use of the space of Reeves; intraoperative neuromonitoring
Summary
The Cernea classification is a practical, anatomy-based system that quantifies the risk of EBSLN injury during thyroid surgery. It divides the nerve's relationship to the superior thyroid pole into three types of progressively increasing risk (Type 1 → 2A → 2B). Its significance lies in directing surgical technique — specifically the mandate for individual superior pole vessel ligation and awareness of high-risk variants — to preserve cricothyroid function and protect the patient's voice quality. In an era of evidence-based surgical practice and medico-legal accountability, awareness of this classification is essential for every surgeon who operates on the thyroid.
Sources:
- Schwartz's Principles of Surgery, 11th Ed., Chapter 38 — Nerves (EBSLN and Cernea classification)
- Current Surgical Therapy, 14th Ed. — Anatomy section (Cernea classification with Figure 1)
- Mulholland and Greenfield's Surgery, 7th Ed. — Chapter 75, Nerves of the thyroid
- Sabiston Textbook of Surgery — Chapter 73, Dissection and Release of the Superior Pole
Create a pdf of this
Reading File
Reading File
Running Command
ls -la /home/daytona/workspace/ 2>/dev/null || echo "workspace not found"
Running Command
mkdir -p /home/daytona/workspace/cernea-classification && echo "done"
Writing File
~/cernea-classification/create_pdf.py
import json
import subprocess
import base64
import os
from reportlab.lib.pagesizes import A4
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.units import cm
from reportlab.lib import colors
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Image, Table, TableStyle,
HRFlowable, KeepTogether
)
from reportlab.lib.enums import TA_CENTER, TA_JUSTIFY, TA_LEFT
from io import BytesIO
OUTPUT_PATH = "/home/daytona/workspace/cernea-classification/Cernea_Classification_Thyroid.pdf"
IMAGE_URL = "https://cdn.orris.care/cdss_images/bbbf46fc1d820f22c446753fbb498feef17c25cce444f230f1a52e31680bb02a.png"
# ── Download image ──────────────────────────────────────────────────────────
print("Downloading diagram image...")
result = json.loads(subprocess.check_output([
"node", "/home/daytona/skills/shared/scripts/fetch_images.js", IMAGE_URL
]))
img_path = None
if result and result[0].get("base64"):
raw = base64.b64decode(result[0]["base64"].split(",")[1])
img_path = "/home/daytona/workspace/cernea-classification/cernea_diagram.png"
with open(img_path, "wb") as f:
f.write(raw)
print(f"Image saved to {img_path}")
else:
print("Image download failed, continuing without image.")
# ── Styles ───────────────────────────────────────────────────────────────────
doc = SimpleDocTemplate(
OUTPUT_PATH,
pagesize=A4,
leftMargin=2.5*cm, rightMargin=2.5*cm,
topMargin=2.5*cm, bottomMargin=2.5*cm,
title="Cernea Classification – ENT PG Essay",
author="Orris Medical"
)
styles = getSampleStyleSheet()
W = A4[0] - 5*cm # usable width
style_title = ParagraphStyle("MyTitle",
fontName="Helvetica-Bold", fontSize=16, leading=22,
alignment=TA_CENTER, spaceAfter=6, textColor=colors.HexColor("#1a3a5c"))
style_subtitle = ParagraphStyle("MySubtitle",
fontName="Helvetica-Oblique", fontSize=10, leading=14,
alignment=TA_CENTER, spaceAfter=4, textColor=colors.HexColor("#555555"))
style_h1 = ParagraphStyle("H1",
fontName="Helvetica-Bold", fontSize=13, leading=18,
spaceBefore=14, spaceAfter=4, textColor=colors.HexColor("#1a3a5c"))
style_h2 = ParagraphStyle("H2",
fontName="Helvetica-Bold", fontSize=11, leading=16,
spaceBefore=10, spaceAfter=3, textColor=colors.HexColor("#2c6e9e"))
style_body = ParagraphStyle("Body",
fontName="Helvetica", fontSize=10, leading=15,
alignment=TA_JUSTIFY, spaceBefore=4, spaceAfter=4)
style_body_small = ParagraphStyle("BodySmall",
fontName="Helvetica", fontSize=9, leading=13,
alignment=TA_JUSTIFY, spaceBefore=2, spaceAfter=2)
style_bullet = ParagraphStyle("Bullet",
fontName="Helvetica", fontSize=10, leading=15,
leftIndent=16, firstLineIndent=-8,
spaceBefore=2, spaceAfter=2)
style_caption = ParagraphStyle("Caption",
fontName="Helvetica-Oblique", fontSize=8.5, leading=12,
alignment=TA_CENTER, spaceAfter=8, textColor=colors.HexColor("#555555"))
style_source = ParagraphStyle("Source",
fontName="Helvetica-Oblique", fontSize=8, leading=11,
textColor=colors.HexColor("#777777"))
def h1(text): return Paragraph(text, style_h1)
def h2(text): return Paragraph(text, style_h2)
def body(text): return Paragraph(text, style_body)
def bullet(text): return Paragraph(f"\u2022 {text}", style_bullet)
def space(n=8): return Spacer(1, n)
def hr(): return HRFlowable(width="100%", thickness=0.8, color=colors.HexColor("#cccccc"), spaceAfter=6)
# ── Build story ──────────────────────────────────────────────────────────────
story = []
# Title block
story.append(space(10))
story.append(Paragraph("Cernea Classification of the External Branch of the", style_title))
story.append(Paragraph("Superior Laryngeal Nerve in Thyroid Surgery", style_title))
story.append(space(4))
story.append(Paragraph("Essay Answer — ENT Post-Graduation Examination", style_subtitle))
story.append(Paragraph("Sources: Schwartz's Surgery 11e · Current Surgical Therapy 14e · Mulholland & Greenfield's Surgery 7e · Sabiston Textbook of Surgery", style_subtitle))
story.append(space(6))
story.append(HRFlowable(width="100%", thickness=2, color=colors.HexColor("#1a3a5c"), spaceAfter=10))
# 1. Introduction
story.append(h1("1. Introduction"))
story.append(body(
"The superior laryngeal nerve (SLN) arises from the vagus nerve at the base of the skull and "
"descends along the internal carotid artery before dividing at the level of the hyoid bone into two branches: "
"(1) the <b>internal branch</b>, which is sensory to the supraglottic larynx and laryngeal mucosa above the vocal cords, and "
"(2) the <b>external branch (EBSLN)</b>, which is the sole motor supply to the cricothyroid muscle and the inferior "
"pharyngeal constrictor."
))
story.append(body(
"The EBSLN is often called the 'nerve of the singing voice' because the cricothyroid muscle — its only target — "
"acts as the vocal cord tensor, controlling pitch, voice projection, and the ability to sustain high-frequency "
"phonation. Its surgical relevance in thyroid operations is profound: it travels in intimate proximity to the "
"superior thyroid pole vessels before reaching the cricothyroid muscle."
))
story.append(body(
"The anatomical variability in the course of this nerve and its relationship to the superior thyroid artery was "
"systematically described by <b>Cernea and colleagues in 1992</b>, leading to the eponymous classification that "
"is now the standard reference for thyroid surgeons worldwide."
))
# 2. Anatomy
story.append(h1("2. Relevant Surgical Anatomy of the EBSLN"))
story.append(body(
"The EBSLN descends from the common SLN trunk and runs along the lateral surface of the inferior pharyngeal "
"constrictor muscle, traveling cephalad-to-caudad lateral to the superior thyroid vascular pedicle. It then "
"crosses the superior thyroid artery in a <i>medial direction</i> to enter and innervate the cricothyroid muscle. "
"This oblique medial crossing — and specifically the level at which it occurs relative to the superior pole of "
"the thyroid — defines the surgical risk zone."
))
story.append(body(
"The superior thyroid artery, the first branch of the external carotid artery, divides into anterior and "
"posterior branches at the apex of the thyroid lobe. In large, ptotic, or multi-nodular goitres, the nerve "
"may descend even lower, increasing jeopardy during superior pole ligation."
))
# 3. Classification
story.append(h1("3. The Cernea Classification"))
story.append(body(
"Cernea et al. studied 33 cadaveric necks and 28 surgical patients, establishing a practical anatomical "
"classification based on the relationship of the EBSLN to the <b>superior thyroid pole</b> and the "
"<b>superior thyroid vessels</b>, measured using a 1 cm reference above the upper border of the thyroid pole."
))
story.append(h2("Type 1"))
story.append(body(
"The EBSLN crosses the superior thyroid vessels <b>≥ 1 cm above</b> the superior border of the thyroid lobe. "
"The nerve is well away from the superior pole dissection zone. This represents the <b>lowest surgical risk</b> "
"and is the most common variant, occurring in approximately <b>50–75%</b> of individuals."
))
story.append(h2("Type 2A"))
story.append(body(
"The EBSLN crosses the superior thyroid vessels <b>within 1 cm above</b> the superior border of the thyroid "
"superior pole — i.e., less than 1 cm above the upper edge, but still above it. The nerve lies close to the "
"vascular pedicle and within the surgical field during standard superior pole dissection, carrying a "
"<b>significantly higher risk</b> of injury. Incidence: approximately <b>18–20%</b>."
))
story.append(h2("Type 2B"))
story.append(body(
"The EBSLN crosses the superior thyroid vessels <b>at or below</b> the superior border of the thyroid lobe, "
"meaning the nerve descends behind the thyroid capsule itself. This variant carries the <b>highest risk</b> of "
"injury — the nerve may be ligated en masse with the superior thyroid vessels if these are not divided "
"individually close to the thyroid surface. Incidence: approximately <b>6–7%</b>; more common in patients with "
"large or ptotic glands."
))
# Image
story.append(space(8))
if img_path and os.path.exists(img_path):
img = Image(img_path, width=14*cm, height=5.5*cm)
img.hAlign = "CENTER"
story.append(KeepTogether([
img,
Paragraph(
"Figure: Cernea classification of the EBSLN. Type 1: nerve crosses > 1 cm above the superior pole. "
"Type 2A: nerve crosses within 1 cm above the pole. Type 2B: nerve crosses below the border of the superior "
"pole. Types 2A and 2B are most vulnerable during thyroidectomy.<br/>"
"<i>(From Gray's Surgical Anatomy, as reproduced in Current Surgical Therapy 14e)</i>",
style_caption
)
]))
story.append(space(6))
# 4. Modified classifications
story.append(h1("4. Modified Classifications"))
story.append(body(
"The <b>Kierner modification</b> and subsequent refinements have been proposed, but the original three-category "
"Cernea system remains the most widely adopted. <b>Friedman's modification</b> simplifies the system into two "
"types: Type 1 (crossing ≥ 1 cm above) and Type 2 (unifying Cernea 2A and 2B). For purposes of surgical "
"planning and examinations, the original Cernea three-type classification is standard."
))
# 5. Significance
story.append(h1("5. Clinical Significance"))
story.append(h2("5.1 Incidence of Injury"))
story.append(body(
"Injury to the EBSLN during thyroidectomy is the <b>most common nerve injury</b> in thyroid surgery and is "
"often underreported because it does not cause the dramatic vocal cord palsy associated with RLN injury. "
"Reported rates range from 0% (meticulous dissections) to 58% (when the nerve is not specifically sought). "
"With the Type 2B variant, routine en masse ligation of the superior pole virtually guarantees nerve injury."
))
story.append(h2("5.2 Consequences of Injury"))
story.append(body("Injury to the EBSLN leads to cricothyroid muscle denervation, resulting in:"))
for b in [
"Loss of ability to tense the ipsilateral vocal cord",
"Inability to produce high-pitched sounds — difficulty 'hitting high notes'",
"Voice fatigue during prolonged speech",
"Reduced voice projection and volume",
"In professional voice users (singers, teachers, lawyers, clergy), the impairment can be career-ending",
]:
story.append(bullet(b))
story.append(body(
"The classic bedside test is <b>high-pitched 'e' phonation</b> — the affected patient cannot sustain a "
"high-pitched note. Laryngoscopy may reveal subtle posterior glottic asymmetry and a low-lying arytenoid "
"on the affected side."
))
story.append(h2("5.3 Surgical Implications"))
story.append(body("The Cernea classification directly guides surgical technique:"))
for b in [
"<b>Individual vessel ligation at the thyroid capsule:</b> Each branch of the superior thyroid artery should be ligated individually, as close as possible to the thyroid capsule, regardless of nerve type.",
"<b>Space of Reeves:</b> An avascular space exists between the medial superior pole and the cricothyroid muscle. Dissecting within this space allows the surgeon to skeletonise superior pole vessels while the EBSLN remains safely lateral.",
"<b>Avoid mass ligation:</b> En masse ligation is particularly dangerous in Type 2B anatomy where the nerve lies behind the thyroid capsule.",
"<b>Intraoperative neuromonitoring (IONM):</b> EMG-based IONM from the cricothyroid muscle helps confirm EBSLN integrity in real time, especially for Type 2A and 2B variants.",
"<b>Effect of pathology:</b> A large or ptotic thyroid gland may drag the nerve inferiorly — effectively converting a Type 1 into a Type 2B-equivalent anatomy. Extra vigilance is required in goitre surgery, re-operations, and Graves' disease.",
]:
story.append(bullet(b))
story.append(h2("5.4 Importance in Professional Voice Users"))
story.append(body(
"Preoperative identification of Cernea type, informed consent discussion, and baseline voice assessment "
"(perceptual analysis, laryngoscopy, voice range profile) are recommended before thyroidectomy in all patients, "
"and are mandatory for professional voice users."
))
# 6. Summary Table
story.append(h1("6. Summary Table"))
table_data = [
["Feature", "Type 1", "Type 2A", "Type 2B"],
["Nerve level relative\nto superior pole", "≥ 1 cm above", "< 1 cm above\n(but above border)", "At or below\nthe superior border"],
["Surgical risk", "Low", "High", "Highest"],
["Approximate frequency", "50–75%", "18–20%", "6–7%"],
["Key surgical danger", "—", "En masse ligation\nnear pole", "Nerve buried\nbehind capsule"],
]
col_widths = [4.5*cm, 3.5*cm, 3.5*cm, 3.5*cm]
t = Table(table_data, colWidths=col_widths, repeatRows=1)
t.setStyle(TableStyle([
# Header row
("BACKGROUND", (0,0), (-1,0), colors.HexColor("#1a3a5c")),
("TEXTCOLOR", (0,0), (-1,0), colors.white),
("FONTNAME", (0,0), (-1,0), "Helvetica-Bold"),
("FONTSIZE", (0,0), (-1,0), 9),
("ALIGN", (0,0), (-1,0), "CENTER"),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
# Body rows
("FONTNAME", (0,1), (-1,-1), "Helvetica"),
("FONTSIZE", (0,1), (-1,-1), 9),
("ALIGN", (1,1), (-1,-1), "CENTER"),
("ALIGN", (0,1), (0,-1), "LEFT"),
("ROWBACKGROUNDS", (0,1), (-1,-1), [colors.HexColor("#f0f5fb"), colors.white]),
("GRID", (0,0), (-1,-1), 0.5, colors.HexColor("#aaaaaa")),
("TOPPADDING", (0,0), (-1,-1), 6),
("BOTTOMPADDING", (0,0), (-1,-1), 6),
("LEFTPADDING", (0,0), (-1,-1), 6),
("RIGHTPADDING", (0,0), (-1,-1), 6),
]))
story.append(t)
story.append(space(8))
# 7. Key facts
story.append(h1("7. Key Facts for ENT PG Examination"))
for b in [
"EBSLN innervates the <b>cricothyroid muscle</b> — the only intrinsic laryngeal muscle supplied by the SLN",
"All other intrinsic laryngeal muscles are supplied by the <b>RLN</b>",
"EBSLN injury causes <b>loss of high-pitched phonation</b> — not hoarseness in the traditional sense",
"<b>Type 2B</b> carries the highest surgical risk; the nerve is buried behind the thyroid capsule",
"Prevention: <b>individual vessel ligation close to the thyroid surface</b>; use of the <b>Space of Reeves</b>; intraoperative neuromonitoring",
"Large/ptotic goitre can convert a Type 1 anatomy to a functionally Type 2B-equivalent situation",
"The internal branch of the SLN, if injured, causes <b>aspiration</b> (loss of supraglottic sensation) — a distinct and rarer injury",
]:
story.append(bullet(b))
# 8. Conclusion
story.append(h1("8. Summary"))
story.append(body(
"The Cernea classification is a practical, anatomy-based system that quantifies the risk of EBSLN injury "
"during thyroid surgery. It divides the nerve's relationship to the superior thyroid pole into three types of "
"progressively increasing risk (Type 1 → 2A → 2B). Its significance lies in directing surgical technique — "
"specifically the mandate for individual superior pole vessel ligation and heightened awareness for high-risk "
"variants — to preserve cricothyroid function and protect the patient's voice quality. In an era of "
"evidence-based surgical practice and medico-legal accountability, awareness of this classification is "
"essential for every surgeon who operates on the thyroid gland."
))
story.append(space(16))
story.append(HRFlowable(width="100%", thickness=0.8, color=colors.HexColor("#cccccc"), spaceAfter=4))
story.append(Paragraph(
"<b>References:</b> Schwartz's Principles of Surgery 11e (Ch. 38) • "
"Current Surgical Therapy 14e (Anatomy) • "
"Mulholland & Greenfield's Surgery 7e (Ch. 75) • "
"Sabiston Textbook of Surgery (Ch. 73)",
style_source
))
# ── Build ─────────────────────────────────────────────────────────────────────
doc.build(story)
print(f"PDF created: {OUTPUT_PATH}")
Running Command
cd /home/daytona/workspace/cernea-classification && python create_pdf.py
Running Command
ls -lh /home/daytona/workspace/cernea-classification/
Your PDF is ready:
Cernea Classification Thyroid
PDF Document · PDF
The PDF includes:
- Formatted essay with all 8 sections (Introduction → Anatomy → Classification → Modified Classifications → Clinical Significance → Summary Table → Key Facts → Conclusion)
- The Cernea classification diagram embedded with caption
- A colour-coded summary table (Type 1 / 2A / 2B)
- References footer citing all four textbooks
- Clean A4 layout with professional styling suitable for exam revision
This is a shared conversation. Sign in to Orris to start your own chat.