Cortical vein thrombosis as per Harrison for pg medicine exam 10 marks
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed from Harrison's. Let me compose the comprehensive 10-mark PG exam answer.
Cortical Vein Thrombosis (Suppurative Intracranial Thrombophlebitis)
As per Harrison's Principles of Internal Medicine 22E - 10 Marks
Definition
Suppurative intracranial thrombophlebitis is septic venous thrombosis of cortical veins and sinuses. It may occur as a complication of:
- Bacterial meningitis
- Subdural empyema (SDE)
- Epidural abscess
- Infection in the skin of the face, paranasal sinuses, middle ear, or mastoid
Anatomy and Pathophysiology
A key anatomical feature is that cerebral veins and venous sinuses have no valves; therefore, blood within them can flow in either direction.
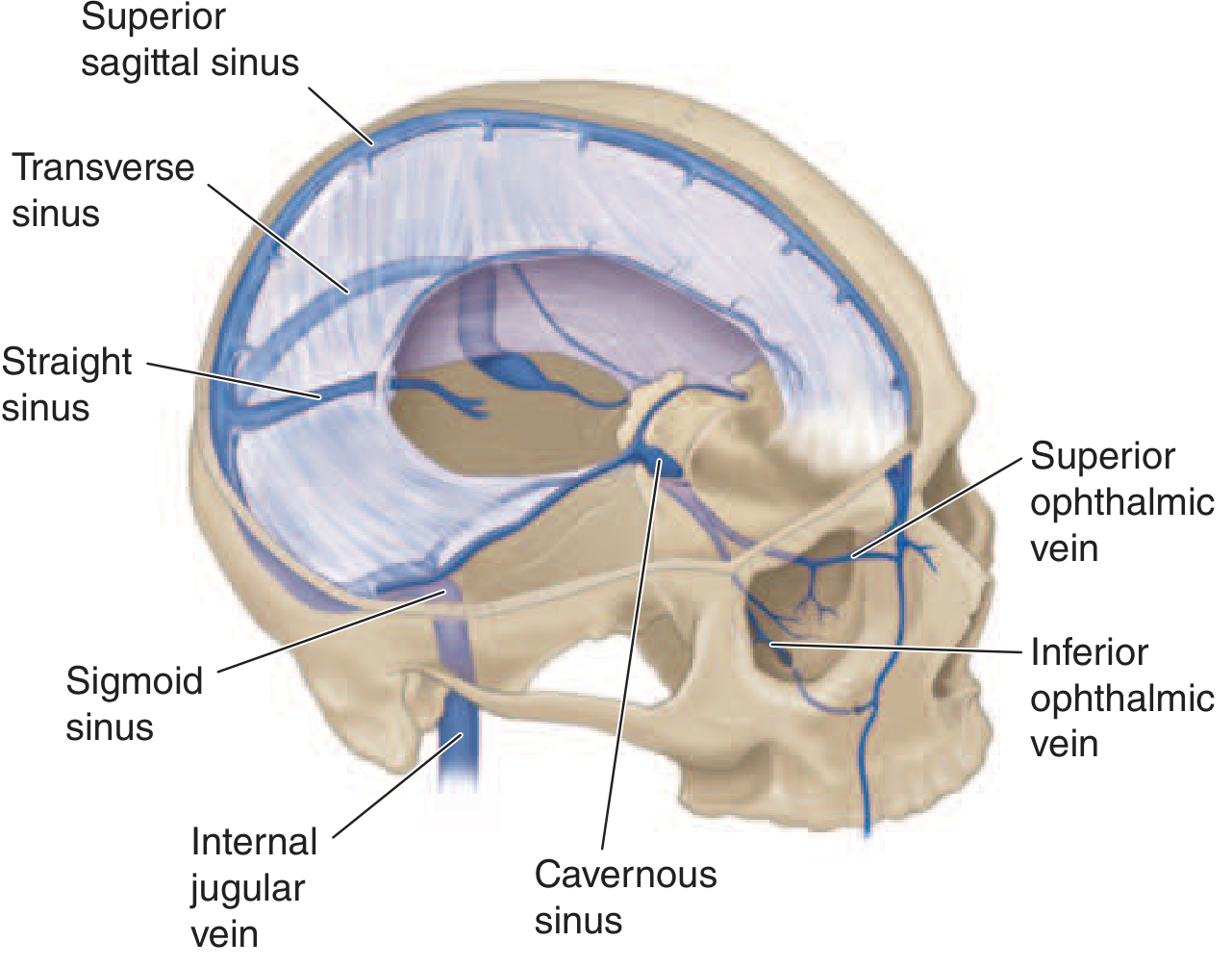
Superior Sagittal Sinus (SSS):
- The largest of the venous sinuses
- Receives blood from frontal, parietal, and occipital superior cerebral veins and the diploic veins
- The diploic veins communicate with meningeal veins and provide a route for spread of infection from meninges, especially from purulent exudate near the SSS
- Infection can also spread from nearby SDE or epidural abscess
- Additional contributors: dehydration from vomiting, hypercoagulable states, immunologic abnormalities (including circulating antiphospholipid antibodies)
- Thrombosis may extend from one sinus to another - at autopsy, thrombi of different histologic ages can be detected in several sinuses
- SSS thrombosis is often associated with thrombosis of superior cortical veins and small parenchymal hemorrhages
Transverse/Sigmoid Sinus:
- SSS drains into the transverse sinuses
- Transverse sinuses also receive venous drainage from middle ear and mastoid cells
- Transverse sinus → sigmoid sinus → internal jugular vein
- Septic transverse/sigmoid sinus thrombosis can complicate acute and chronic otitis media or mastoiditis
- Infection spreads via emissary veins or direct invasion from mastoid air cells
Cavernous Sinus:
- Inferior to SSS, at the base of the skull
- Receives blood from facial veins via superior and inferior ophthalmic veins
- Bacteria enter from facial veins or via emissary veins from sphenoid and ethmoid sinuses
- Sphenoid and ethmoid sinuses are the most common sites of primary infection in septic cavernous sinus thrombosis
Clinical Manifestations
Superior Sagittal Sinus Thrombosis
- Headache, fever, nausea and vomiting, confusion
- Focal or generalized seizures
- Rapid development of stupor and coma
- Weakness of lower extremities with bilateral Babinski's signs, or hemiparesis
- When complicating bacterial meningitis: nuchal rigidity, Kernig's and Brudzinski's signs
Cavernous Sinus Thrombosis
The following structures pass through the cavernous sinus: CN III, CN IV, CN VI, ophthalmic and maxillary branches of CN V, and the internal carotid artery.
- Fever, headache, frontal and retroorbital pain, diplopia
- Classic signs: ptosis, proptosis, chemosis, extraocular dysmotility (due to CN III, IV, VI deficits)
- Hyperesthesia of ophthalmic and maxillary divisions of CN V + decreased corneal reflex
- Dilated tortuous retinal veins and papilledema
Transverse/Sigmoid Sinus Thrombosis
- Headache and earache are most frequent symptoms
- Otitis media, sixth nerve palsy, retroorbital or facial pain = Gradenigo's syndrome
- Sigmoid sinus and internal jugular vein thrombosis may present with neck pain
Diagnosis
- Absent flow void within the affected venous sinus on MRI is the key suggestive finding
- Confirmed by: contrast-enhanced MR venography, CT venography, or venous phase of cerebral angiography
- Thrombophlebitis of intracerebral and meningeal veins is suggested by presence of intracerebral hemorrhage but requires venous phase of cerebral angiography for definitive diagnosis
Treatment
Antimicrobial Therapy
- Based on the bacteria responsible for the predisposing or associated condition
- Optimal duration unknown; antibiotics usually continued for 6 weeks or until radiographic evidence of resolution of thrombosis
Anticoagulation
- Unfractionated or low-molecular-weight heparin is recommended for:
- Aseptic venous sinus thrombosis
- Septic venous sinus thrombosis complicating bacterial meningitis with progressive neurologic deterioration despite antimicrobial therapy and IV fluids
- A small intracerebral hemorrhage from septic thrombophlebitis is not an absolute contraindication to heparin therapy
Surgical/Interventional
- Removal of infected tissue and thrombus in septic lateral or cavernous sinus thrombosis
- Successful management of aseptic cases has been reported with:
- Surgical thrombectomy
- Catheter-directed urokinase therapy
- Combination of intrathrombus rtPA + IV heparin
- However, insufficient data to recommend these in septic venous sinus thrombosis
Quick Summary Table for Exam
| Sinus | Primary Source | Key Features |
|---|---|---|
| Superior Sagittal | Meningitis, SDE | Seizures, lower limb weakness, bilateral Babinski's |
| Cavernous | Sphenoid/ethmoid sinusitis, face | Ptosis, proptosis, chemosis, CN III/IV/VI palsy |
| Transverse/Sigmoid | Otitis media, mastoiditis | Headache, earache, Gradenigo's syndrome |
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 145 - Suppurative Thrombophlebitis.
This is a shared conversation. Sign in to Orris to start your own chat.