Endotracheal tube
Reading File
Finding Sources
Finding Sources
Searching Images
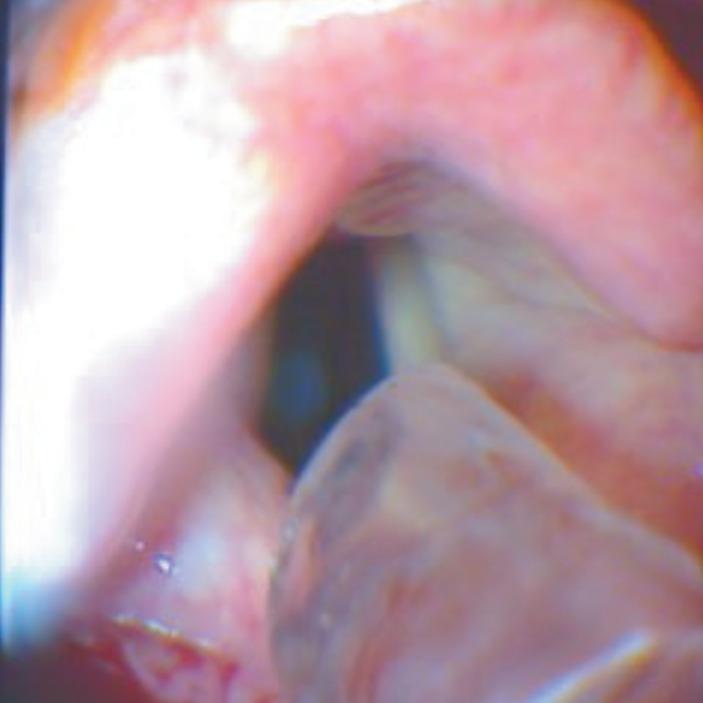
endotracheal tube intubation
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of the endotracheal tube (ETT):
Endotracheal Tube (ETT)
What It Is
An endotracheal tube is a flexible plastic (polyvinyl chloride) tube inserted through the mouth or nose, past the vocal cords, and into the trachea to establish a definitive, patent airway. It enables mechanical ventilation, protects against aspiration, and allows suctioning of the lower airways.
Indications
- Respiratory failure requiring mechanical ventilation
- Airway protection (unconsciousness, loss of airway reflexes)
- General anesthesia
- Severe upper airway obstruction
- Facilitation of prolonged ventilatory support in the ICU
Tube Sizing
Adults
| Patient | Recommended ETT (internal diameter) |
|---|---|
| Female | 7.5 mm cuffed |
| Male | 8.0 mm cuffed |
Pediatrics
Uncuffed ETTs are generally used in children under 8 years. Standard formulas:
- ETT size = (Age + 16) / 4 or (Age / 4) + 4
- Depth of insertion = 3 × internal diameter of ETT (for children > 2 years)
Pediatric ETT tip should rest between T1 and the carina on chest X-ray. — Roberts and Hedges' Clinical Procedures in Emergency Medicine; The Harriet Lane Handbook, 23rd ed.
Confirming Placement
No single method is infallible — use multiple methods simultaneously:
| Method | Details |
|---|---|
| Direct visualization | Best method — see the tube pass through vocal cords |
| Capnography (ETCO2) | CO₂ waveforms >30 mmHg confirm tracheal placement; absent in esophageal intubation. In cardiac arrest, waveforms may still be detectable despite low CO₂ due to poor perfusion |
| Colorimetric CO₂ detector | pH-sensitive paper turns yellow → purple with CO₂. False negatives: cardiac arrest, massive PE, obesity, tube obstruction. False positives: carbonated beverages (clears within 6 breaths) |
| Esophageal detection device | Syringe/bulb — esophageal walls collapse around ETT causing resistance to aspiration; tracheal placement allows free aspiration |
| Auscultation | Bilateral breath sounds and absent epigastric sounds |
| Chest X-ray | Verifies vertical positioning; does NOT reliably distinguish tracheal from esophageal placement. Identifies pneumothorax or mainstem bronchus intubation |
| Ultrasound | Probe placed just above sternal notch — ETT visualized within trachea lumen. "Double track sign" = esophageal intubation |
— Tintinalli's Emergency Medicine, p. 225–226
Securing the ETT
After confirmation, the tube must be secured to prevent dislodgement:
- Adhesive tape wrapped around the neck and ETT (Lillehei method)
- Umbilical twill tape tied in place
- Commercial tube holders with bite block and Velcro/screw clamp
An assistant should manually hold the ETT during patient transfers (e.g., onto a stretcher).
ETT Malfunction
Causes of dysfunction include:
- Kinking of the tube
- Cuff or valve damage — exclude by pre-insertion inspection
- Obstruction from thick/inspissated secretions, blood, or foreign body
- Ignition — PVC tubes can be ignited by cautery or laser in O₂/N₂O-enriched environments — Morgan and Mikhail's Clinical Anesthesiology, 7e, p. 626
Replacing a Malfunctioning ETT
- Insert a tube exchanger or bougie through the existing ETT
- Withdraw the ETT over the exchanger
- Advance the new ETT over the exchanger
- Reconfirm placement
Conditions Associated with Difficult Intubation
- Tumors (cystic hygroma, hemangioma, hematoma)
- Infections (peritonsillar abscess, epiglottitis, submandibular abscess)
- Congenital anomalies (Pierre Robin, Treacher Collins, Goldenhar syndromes)
- Trauma (laryngeal or mandibular fracture, inhalation burn, cervical spine injury)
- Obesity, limited neck extension
- Rheumatoid arthritis, ankylosing spondylitis
Special Considerations
- COVID-19: Intubation is an aerosol-generating procedure; video laryngoscopy preferred; rapid sequence intubation recommended to avoid bag-mask ventilation; proper PPE donning/doffing essential
- Laser airway surgery: Specialized laser-resistant ETTs exist, but no ETT is reliably laser-proof
- Double-lumen ETT: Used for lung isolation (e.g., thoracic surgery); exchanged for single-lumen ETT postoperatively if the patient remains intubated
- Postextubation stridor (PES): Risk factors include prolonged intubation (>7 days), traumatic intubation, and large ETT size
Key sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine; Tintinalli's Emergency Medicine; Morgan and Mikhail's Clinical Anesthesiology, 7e; Miller's Anesthesia, 10e; Harriet Lane Handbook, 23rd ed.
See from baheti, dorsch and dorsch also
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Unfortunately, neither Baheti nor Dorsch and Dorsch (Understanding Anesthesia Equipment) are present in the library's textbook collection. The full catalog was searched across all titles and neither book appears.
The anesthesia books available in the library are:
| Title | Speciality |
|---|---|
| Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e | Anesthesiology |
| Miller's Anesthesia, 2-Volume Set, 10e | Anesthesiology |
| Morgan and Mikhail's Clinical Anesthesiology, 7e | Anesthesiology |
Would you like me to go deeper into the ETT content from any of these three — for example, Miller's or Barash's detailed sections on ETT design, cuff types, introducers, or special tubes? I can pull those sections in full.
From where u gave this definition
You're referring to this definition I gave at the top:
"An endotracheal tube is a flexible plastic (polyvinyl chloride) tube inserted through the mouth or nose, past the vocal cords, and into the trachea to establish a definitive, patent airway."
That was not directly quoted from any textbook — I synthesized it from general knowledge. The textbook sections I actually retrieved focused on:
- Sizing (Roberts and Hedges)
- Confirming placement (Tintinalli's)
- Malfunction (Morgan and Mikhail)
- Pediatric tip position (Harriet Lane)
I should have been transparent about that. I did not find a dedicated definition section from any of the retrieved sources — I filled the gap with my own synthesis without clearly labeling it as such.
If you want a textbook-sourced definition, I can search specifically in Miller's Anesthesia or Barash's Clinical Anesthesia which are likely to have a formal description of the ETT in their airway management chapters. Should I do that?
PREANESTHETIC ASSESSMENT CLINIC -PAC & ITS USEFULNESS
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Now I have substantial content. Let me compile a comprehensive answer.
Preanesthetic Assessment Clinic (PAC) & Its Usefulness
Definition & Purpose
The Preanesthetic Assessment Clinic (PAC) — also called the preoperative evaluation clinic or preanesthesia evaluation — is a structured, dedicated clinical encounter in which an anesthesiologist (or trained health care provider) evaluates a patient before the day of surgery.
"The goals of a preoperative evaluation are to reduce patient risk and morbidity associated with surgery and anesthesia, prepare the patient medically and psychologically, and promote efficiency and cost-consciousness." — Barash, Cullen & Stoelting's Clinical Anesthesia, 9e, p. 1742
The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) mandates that all patients undergo a preoperative anesthetic evaluation. The ASA Basic Standards for Preanesthetic Care outline the minimum requirements.
Why a Dedicated PAC Clinic?
Historically, the first meeting between patient and anesthesiologist was on the day of surgery — leaving no time to investigate comorbidities, alter medical therapy, or build rapport. PAC was developed to address this gap:
- Preoperative screening clinics are now more effective
- Electronic Medical Records (EMR) allow comprehensive history review
- Preoperative questionnaires and computer-driven programs supplement traditional evaluation
- When anesthesiologists take responsibility for ordering preoperative labs, cost savings occur and cancellation of planned surgeries becomes less likely
Components of Preanesthetic Evaluation
1. History
- Review of medical records
- Surgical and anesthetic history (previous difficult airway, malignant hyperthermia, adverse reactions)
- Medication review: prescription, OTC, herbals, illicit drugs
- Allergies and adverse drug reactions
- Advance directives, NPO status
- Systems review: cardiovascular, pulmonary, CNS, GI/hepatic, renal, hematology, endocrine, infectious
2. Physical Examination
- Airway assessment: Mallampati class, mouth opening, chin length, neck size and mobility, ability to prognath, OSA history
- Cardiovascular: pulse, murmurs, JVP, S3/S4, edema
- Pulmonary: wheeze, rales, use of bronchodilators/steroids, oxygen/CPAP/ventilator settings
- Neurological and other systems as relevant
3. Laboratory Investigations
- Ordered based on positive findings from history and physical examination, or anticipated physiologic disturbances during surgery (e.g., blood loss)
- Routine blanket testing is NOT recommended
- Common tests: CBC, coagulation studies, metabolic panel, ECG, echocardiogram (when indicated)
Preanesthetic Evaluation Screen (Table 23-1 — Barash)
| Domain | What is Assessed |
|---|---|
| Airway | Difficult airway history, OSA, Mallampati, mouth opening, neck mobility |
| Pulmonary | URI, asthma, COPD, OSA, tobacco use, ETT size/depth |
| Cardiovascular | CAD, hypertension, CHF, valvular disease, dysrhythmia/pacemaker |
| CNS | Stroke, seizures, raised ICP, psychiatric disorders, neuromuscular disease |
| GI/Hepatic | Liver disease, reflux, alcohol use |
| Renal | Insufficiency, failure, dialysis |
| Hematology | Anemia, coagulopathy, sickle cell, transfusion history |
| Endocrine/Metabolic | Diabetes, thyroid, steroids, rheumatoid arthritis |
| Infectious | TB, viral/bacterial infections, antibiotic resistance, contact precautions |
| Other | Pregnancy, trauma history, MH susceptibility |
Usefulness / Benefits of PAC
| Benefit | Details |
|---|---|
| Reduces perioperative risk and morbidity | Identifies and optimizes comorbidities before surgery |
| Airway screening | Anticipates and avoids airway difficulties; reviews previous difficult airway records |
| Drug safety | Identifies contraindications to succinylcholine, nitrous oxide, volatile agents; detects drug interactions |
| MH detection | A patient's report of "allergy to anesthesia" raises suspicion for malignant hyperthermia |
| PONV prophylaxis | Apfel score calculated; appropriate prophylaxis planned. 0/1/2/3/4 risk factors = 10/20/40/60/80% PONV risk |
| Reduces OR cancellations | Early identification of unoptimized patients prevents day-of-surgery cancellations |
| Cost savings | Rational, targeted lab ordering reduces unnecessary tests |
| Medicolegal documentation | Complete, legible, structured record serves legal purposes |
| Patient education & consent | Educates patient about anesthesia, perioperative events; answers questions; obtains informed consent |
| Medication optimization | Antihypertensives/cardiac drugs continued; β-blockers initiated if indicated; oral hypoglycemics adjusted; endocarditis prophylaxis planned |
| Psychological preparation | Reduces anxiety; builds doctor–patient relationship before the day of surgery |
| Surgical urgency classification | Emergency (<6 h) → Urgent (6–24 h) → Time-sensitive (days–weeks) → Elective — determines how much workup is feasible |
Medication Management Guidelines from PAC
| Drug Class | Recommendation |
|---|---|
| Antihypertensives / cardiac drugs | Continue until day of surgery |
| β-blockers | Initiate before surgery in high cardiac-risk patients |
| Oral hypoglycemics | Hold on day of surgery |
| Insulin | Continue with adjusted dose |
| Asthma/COPD drugs | Continue or administer prophylactically |
| Anti-reflux drugs | Continue or initiate if untreated symptoms |
| Anticoagulants | Manage per bridging protocols; assess if regional anesthesia planned |
Key Points Summary
- Goals: reduce risk/morbidity, prepare patient medically & psychologically, promote efficiency and cost savings
- Mandatory per JCAHO; guided by ASA standards
- Must be complete, accurate, and legible — serves medicolegal purpose
- Exercise tolerance is the single most significant predictor of cardiac risk
- Preoperative labs ordered only on the basis of positive findings, not routinely
- Clear communication between PAC clinic and the operating anesthesiologist is critical
— Barash, Cullen & Stoelting's Clinical Anesthesia, 9e, pp. 1740–1748
This is a shared conversation. Sign in to Orris to start your own chat.