Tendinopathy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of tendinopathy:
Tendinopathy
Definition & Terminology
Tendinopathy is an umbrella term for painful, impaired tendons. It encompasses:
- Tendinitis — historically implied acute inflammation
- Tendinosis — now preferred; reflects the true pathology: a degenerative process with few or no inflammatory cells on histopathology
Histopathologic analysis of most tendinopathies reveals degenerative tendon pathology rather than true inflammation, which is why the terminology has shifted.
Epidemiology
- ~30% of all musculoskeletal evaluations in emergency or urgent care settings involve tendinopathy
- The incidence is rising, paralleling a 3.6% increase in athletic/fitness participation over a 12-year period
- Accounts for the 5th most days away from work among non-fatal injuries in the U.S. (~14 days average)
- Economic impact: estimated ~$800 billion in healthcare costs over 3 years
- Workers with 25–35 years of service are 7.1× more likely to develop tendinopathy
Pathophysiology
Acute Tendon Healing Stages
- Hemorrhagic phase — blood accumulates and clots
- Inflammatory phase — neutrophils and macrophages perform phagocytosis of necrotic material
- Proliferative phase — extrinsic and intrinsic cells migrate; type III collagen synthesized (thinner, less tensile strength than type I)
- Formative phase (up to 2 months) — collagen fibers mature and orient to handle tensile forces
- Remodeling phase — normalization of type I:III collagen ratio; physiologic load reintroduced
Full strength recovery may take up to 12 weeks.
Key Concept — Optimal Loading
- Complete immobilization is relatively contraindicated — atrophy worsens outcomes
- Optimal loading (graduated, incremental rehabilitation with eccentric training) is now the preferred approach
Etiology & Risk Factors
Intrinsic Factors
- Age, female sex, blood type O
- Adiposity, tobacco use
- Malalignment, joint laxity, muscle weakness/imbalance
Extrinsic Factors
- Ergonomics, abnormal movement patterns
- Excessive activity duration, frequency, or intensity
- Equipment changes, environmental conditions
Drug-Related Causes
| Agent | Risk |
|---|---|
| Fluoroquinolones | ↑ tendinopathy and rupture; greatest risk in first month of use, age >60, concurrent corticosteroids (14.7× risk of Achilles rupture), renal disease |
| Statins | ~2% incidence; simvastatin may actually reduce risk |
Systemic Causes
- Diabetes mellitus, gout, coronary artery disease
- Rheumatologic disorders
- Infectious (e.g., Mycobacterium)
Common Sites
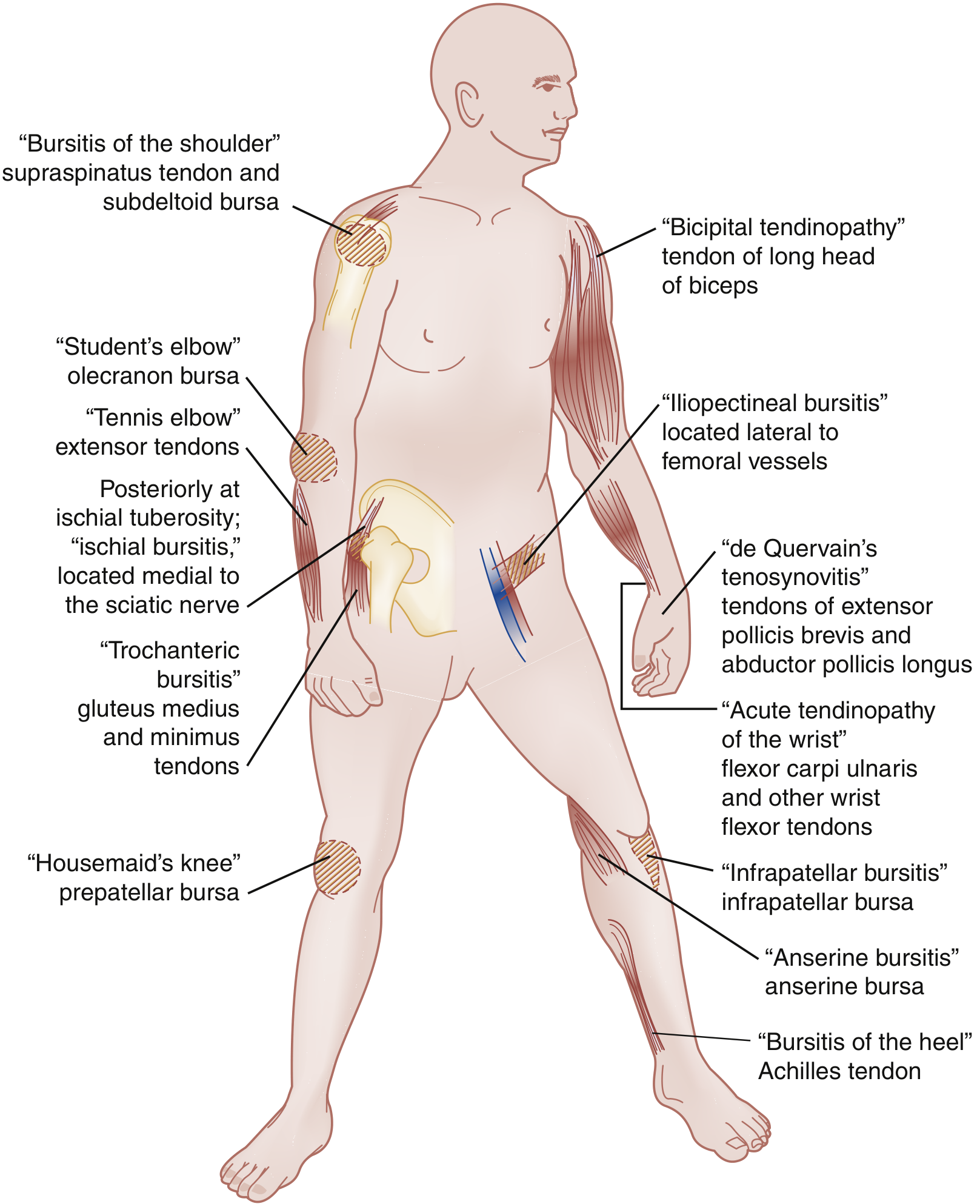
Key locations include: rotator cuff (supraspinatus), bicipital tendon, lateral epicondyle (tennis elbow — extensor carpi radialis brevis), medial epicondyle (golfer's elbow), Achilles tendon, patellar tendon, de Quervain's tenosynovitis (extensor pollicis brevis / abductor pollicis longus), and wrist flexors.
Clinical Features
- Non-radiating, localized pain at the tendon site — most common symptom
- Pain worse after rest (morning stiffness) or with loading
- History of repetitive stress (occupational or sports-related, often weeks to months prior)
- Ask about fluoroquinolone/statin use, systemic illness, recent ergonomic changes
Differential Diagnosis
- Tendon rupture
- Ligamentous injury
- Inflammatory arthritis (e.g., rheumatoid)
- Stress or avulsion fracture
- Bursitis, septic arthritis
- Tenosynovitis
- Osteochondrosis (e.g., Osgood-Schlatter)
- Tumors
Diagnosis
- Clinical in most cases
- Plain radiographs: useful to identify calcific tendinopathy or exclude bony pathology (~20% show calcification in lateral epicondylitis)
- Ultrasound: recommended first-line imaging; identifies tendon disruption/rupture, useful for guided procedures (e.g., calcific tendinopathy lavage)
- MRI: gold standard for detailed soft tissue evaluation
Management
Box: Components of Tendinopathy Management
- Identify and eliminate the cause
- Analgesics — short-term NSAIDs
- Protection + relative rest (avoid complete immobilization)
- Optimal loading — ergonomic alteration, graduated eccentric exercises
- Ice, compression, elevation
- Patient education and behavior modification
- Vitamin D supplementation
- Referral for rehabilitation (PT, sports medicine, orthopaedics)
Pharmacological Adjuncts
| Treatment | Notes |
|---|---|
| NSAIDs | First-line for analgesia; short-term use |
| Nitroglycerin patches | Effective for lateral/medial epicondylitis, noninsertional Achilles, and rotator cuff tendinopathy; less evidence for patellar; off-label use |
| Corticosteroid injection | Short-term pain relief only; avoid intratendinous injection (risk of rupture, especially Achilles and patellar); peritendinous injection acceptable in select conditions (e.g., de Quervain's) |
| PRP (Platelet-Rich Plasma) | Variable evidence; not first-line; best delivered under ultrasound guidance |
Surgical
- Indicated for tendon rupture (primary repair) or refractory cases that have failed conservative treatment
- Débridement for recalcitrant cases (e.g., patellar tendinopathy)
Prognosis
- Overuse tendinopathies: full recovery typically within 3–6 months
- Recurrence common — 49% of athletes with patellar tendinopathy; 40–50% of rotator cuff tendinopathy patients symptomatic at 6–12 months
Sources: Rosen's Emergency Medicine: Concepts and Clinical Practice; Textbook of Family Medicine 9e; Imaging Anatomy: Bones, Joints, Vessels and Nerves
This is a shared conversation. Sign in to Orris to start your own chat.