Spinal Anaesthesia comprehensive review
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have all the material needed for a comprehensive review. Let me compile it.
Spinal Anaesthesia — Comprehensive Review
1. Anatomy
Relevant Structures (Surface to Subarachnoid Space)
- Skin → subcutaneous fat → supraspinous ligament → interspinous ligament → ligamentum flavum → epidural space → dura mater → subdural space → arachnoid mater → subarachnoid space (CSF)
- The spinal cord typically terminates at L1–L2 in adults (conus medullaris); the dural sac extends to S2. Below L2, the cauda equina floats freely in CSF — this is why lumbar puncture at L3–4 or L4–5 is safe.
- Neonates have a lower cord termination (L3) and relatively larger CSF volume (~10 mL/kg vs 1.5–2 mL/kg in adults), requiring proportionally higher local anesthetic doses.
Cerebrospinal Fluid
- CSF density: 1.00059 g/mL at 37°C
- Lumbosacral CSF pressure: ~15 cm H₂O
- CSF volume accounts for 80% of the variability in peak block height and regression of blockade. Body weight (BMI) inversely correlates with CSF volume (less CSF in obese patients)
(Miller's Anesthesia, 10e)
2. Mechanism of Action
Local anesthetics bind voltage-gated sodium channels, interrupting impulse transmission. Key target sites in spinal anaesthesia are:
- Spinal nerve roots (in the subarachnoid space) — most accessible and most easily blocked
- Dorsal root ganglia
- Superficial and deep portions of the spinal cord
Differential Nerve Block (order of susceptibility — most to least):
| Fibre | Size | Myelination | Function | Blocked First? |
|---|---|---|---|---|
| B fibres | 1–3 µm | Minimally | Preganglionic sympathetic | ✓ First |
| C fibres | 0.3–1 µm | Unmyelinated | Pain, temperature (cold) | ✓ Second |
| Aδ fibres | 1–4 µm | Myelinated | Pain (pinprick) | Third |
| Aβ fibres | 5–12 µm | Myelinated | Touch | Fourth |
| Aα fibres | 12–20 µm | Myelinated | Motor | Last |
Recovery follows the reverse order: motor returns first, then touch, then pinprick, then cold sensation.
Differential sensory block: sympathetic block is 1–2 segments above pinprick level; pinprick 1–2 segments above touch.
(Miller's Anesthesia, 10e)
3. Physiological Effects
Cardiovascular
- Hypotension — the most common cardiovascular complication; results from sympathectomy causing vasodilation and decreased venous return. Sympathetic block extends 2–6 dermatomes above the sensory level.
- In healthy normovolemic patients: systemic vascular resistance decreases ~15–18% even with near-total sympathectomy.
- In elderly patients with cardiac disease: SVR decreases ~25%, cardiac output decreases ~10%.
- Bradycardia — results from:
- Blockade of T1–T4 cardiac accelerator fibres
- Reduced venous return → reduced stretch of right atrial chronotropic receptors → increased vagal tone
- The Bezold–Jarisch reflex (small end-diastolic LV volume triggers mechanoreceptor-mediated bradycardia) — particularly in young, healthy, hypovolaemic patients
- Risk factors for exaggerated bradycardia (40–50 bpm): baseline HR <60, age <37, male sex, β-blockade, prolonged case duration
- Cardiac arrest is rare but more likely in young, healthy, conscious patients with high spinal when T1 is blocked
Coronary Circulation
- High thoracic block (T4) can improve myocardial function in ischaemic patients by reducing LV afterload and myocardial oxygen demand.
Respiratory
- Low/mid spinal blocks: minimal respiratory effect (the diaphragm is innervated by C3–5)
- Very high blocks: progressive impairment; intercostal muscle paralysis leads to reduced tidal volume and limited ability to cough
- Total spinal: apnoea from brainstem involvement
Renal
- Modest, clinically unimportant decrease in renal blood flow
- Urinary retention: S2–S4 block inhibits the detrusor muscle; intrathecal opioids amplify the effect
(Miller's Anesthesia, 10e)
4. Indications
Spinal anaesthesia is most commonly used for:
- Lower extremity surgery (arthroplasty, fracture fixation)
- Perineum and pelvic girdle surgery
- Lower abdominal surgery (inguinal hernia, appendicectomy)
- Urological surgery (TURP, cystoscopy)
- Obstetric surgery (caesarean section — preferred over general anaesthesia due to lower maternal morbidity/mortality, better neonatal outcomes)
- Lumbar spine surgery
- Laparoscopic cholecystectomy (described)
- When the patient wishes to remain conscious, or when comorbidities (severe respiratory disease, difficult airway) make general anaesthesia higher risk
- Ex-premature infants undergoing hernia repair (reduces post-operative apnoea risk)
(Miller's Anesthesia, 10e; Morgan & Mikhail, 7e)
5. Contraindications
Absolute
- Patient refusal
- Localised infection at the injection site (risk of meningitis/abscess)
- Allergy to planned drugs
- Severe uncorrected hypovolaemia (high risk of cardiovascular collapse)
- Raised intracranial pressure with mass lesion (risk of brainstem herniation)
- Severe coagulopathy / therapeutic anticoagulation (see ASRA guidelines)
Relative
- Uncooperative patient
- Sepsis (bacteraemia — risk of haematogenous seeding)
- Pre-existing neurological disease (medicolegal concerns)
- Severe aortic stenosis / hypertrophic cardiomyopathy (fixed cardiac output cannot compensate for vasodilation)
- Prior spinal surgery / anatomical abnormalities (technical difficulty, unpredictable spread)
- Anticoagulation (timing per ASRA Fourth Edition guidelines)
(Miller's Anesthesia, 10e)
6. Factors Affecting Block Height
Drug Factors (most controllable)
| Factor | Effect |
|---|---|
| Baricity | Most important. Hyperbaric > isobaric for predictability |
| Dose | Most important determinant of duration and block height |
| Volume | Less important than dose |
| Concentration | Less important than dose |
Baricity
- Baricity = density of LA solution / density of CSF
- Hyperbaric (density > 1.00059 g/mL): spread to dependent regions; more predictable; shorter duration than isobaric; dextrose added
- Hypobaric (density < 1.00059 g/mL): spread to non-dependent regions; sterile water added
- Isobaric: not influenced by gravity
- Clinical application: administer hyperbaric solution in lateral decubitus → preferential block of dependent (operative) side
Lumbar Lordosis
- In the supine position, L3–L4 is the most caudal point; T5–T6 the lowest thoracic point
- Hyperbaric solution injected at L3–4 will pool in the lumbar lordosis or flow cephalad to T5–T6, depending on positioning
Patient Factors (less controllable)
- CSF volume (accounts for 80% of variability)
- BMI (high BMI → less CSF volume → higher block)
- Age (elderly → less CSF)
- Pregnancy (engorged epidural veins compress subarachnoid space → higher spread)
- Height (less important than CSF volume)
(Miller's Anesthesia, 10e)
7. Pharmacology — Local Anaesthetics
| Agent | Type | Classification | Dose Range | Onset | Duration | Notes |
|---|---|---|---|---|---|---|
| Procaine | Ester | Short | 50–200 mg | Slow | Short | Rarely used; high failure rate, nausea |
| Chloroprocaine | Ester | Ultra-short | 30–60 mg | Rapid | 45–60 min | Ideal for ambulatory; modern preservative-free preparations; TNS possible |
| Articaine | Amide/Ester hybrid | Short | — | — | Short | Emerging |
| Lidocaine | Amide | Intermediate | 20–100 mg | Fast | 60–120 min | High TNS risk; avoid for ambulatory |
| Mepivacaine | Amide | Intermediate | — | Fast | 90–150 min | Alternative to lidocaine with less TNS |
| Prilocaine | Amide | Intermediate | — | Moderate | ~100 min | Lower TNS risk than lidocaine |
| Bupivacaine | Amide | Long | 5–20 mg | Moderate | 2–4 h | Most widely used; hyperbaric 0.5% standard |
| Levobupivacaine | Amide | Long | — | Moderate | 2–4 h | Less cardiotoxic than racemic bupivacaine |
| Ropivacaine | Amide | Long | — | Moderate | 2–3 h | Less motor block than bupivacaine |
| Tetracaine | Ester | Long | 5–20 mg | Moderate | 2–4 h | Widely used in paediatrics |
(Miller's Anesthesia, 10e)
8. Additives (Adjuvants)
Opioids
Opioids act on dorsal horn μ-receptors. Intrathecal: intravenous potency ratio = 200–300:1 for morphine, but only 10–20:1 for lipophilic agents (fentanyl, sufentanil).
| Opioid | Lipophilicity | Dose | Onset | Duration | Notes |
|---|---|---|---|---|---|
| Morphine | Hydrophilic | 100–300 mcg | Slow | Up to 24 h | Best for major surgery; delayed respiratory depression risk |
| Diamorphine | Intermediate | 0.3–0.4 mg | Moderate | Long | UK only; prodrug to morphine |
| Fentanyl | Lipophilic | 10–30 mcg | 10–20 min | 4–6 h | Ambulatory use; reduces LA dose requirement |
| Sufentanil | Highly lipophilic | 5–7.5 mcg | Rapid | 2–4 h | Labour analgesia and CS |
| Meperidine | Intermediate | 10–20 mg | Moderate | — | Also has intrinsic LA properties |
Side effects of intrathecal opioids: pruritus (30–100%), nausea/vomiting, urinary retention, respiratory depression (delayed with morphine — up to 24 h later)
Vasoconstrictors
- Epinephrine (100–200 mcg) and phenylephrine prolong block by causing local vasoconstriction, reducing LA vascular uptake; also have direct spinal cord α₂ effects
- Epinephrine extends bupivacaine and tetracaine block by 30–50%
α₂-Agonists
- Clonidine (15–75 mcg intrathecally): prolongs sensory > motor block; mechanism involves K⁺-channel opening and membrane hyperpolarisation; side effects: hypotension, bradycardia, sedation
- Dexmedetomidine: increasing evidence for prolonging block
(Miller's Anesthesia, 10e)
9. Technique
Patient Positioning
- Sitting (flexed): best CSF identification, clearest landmarks; CSF drops readily into needle; preferred for obese patients and saddle blocks
- Lateral decubitus: patient more comfortable; allows selective block with hyperbaric/hypobaric solutions
Approach
Midline approach: most common
- Identify L3–4 or L4–5 interspace (Tuffier's line = iliac crest = L4 vertebral body)
- Raise skin wheal with local anaesthetic
- Insert introducer, then spinal needle with bevel parallel to dural fibres (reduces PDPH)
- Advance through supraspinous → interspinous ligament → ligamentum flavum (resistance) → dura (pop)
- Confirm free CSF flow; inject slowly, aspirating to confirm position before and after
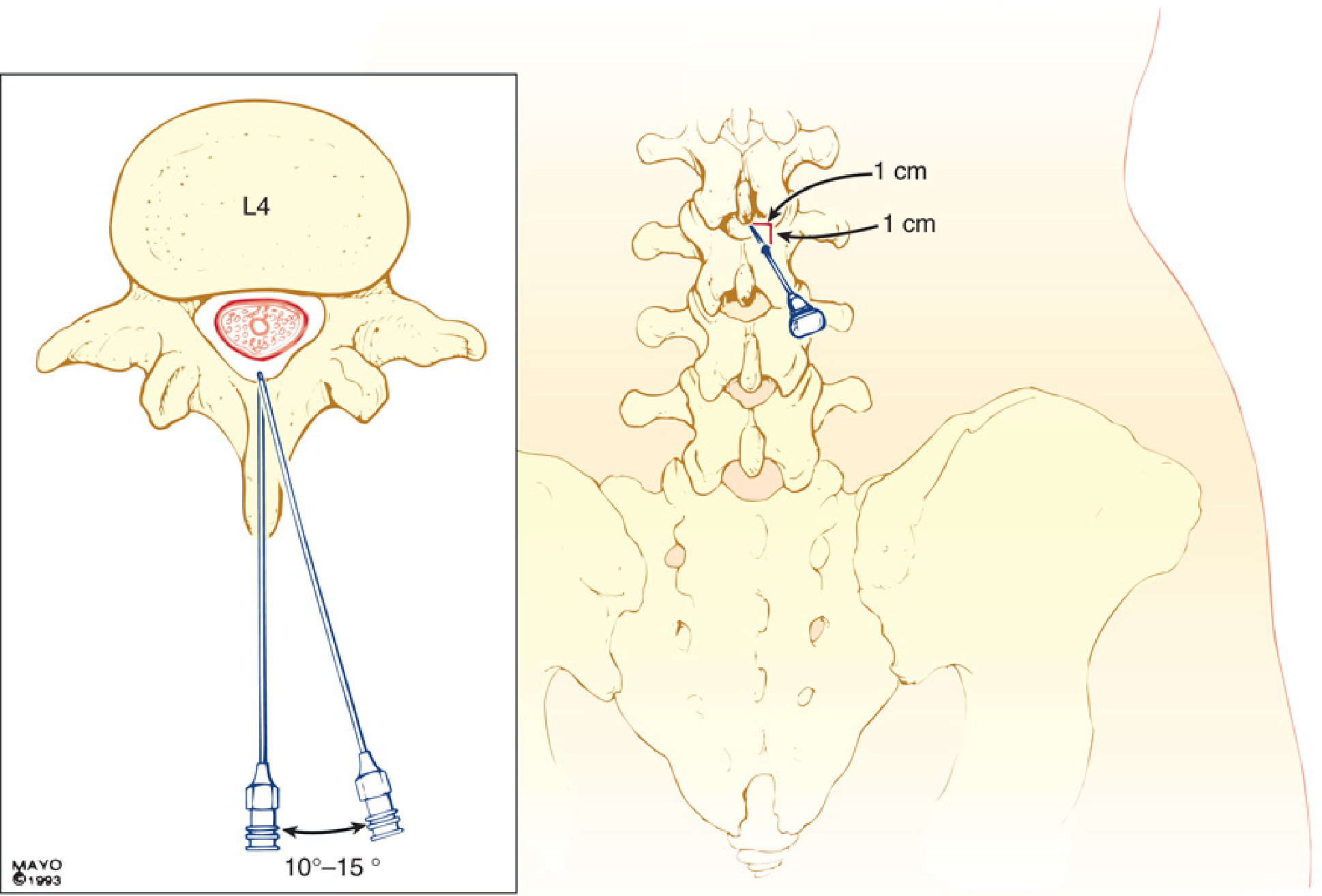
Paramedian approach: useful when calcified interspinous ligaments prevent midline access
- Entry point: 1 cm lateral to superior edge of inferior spinous process
- Direction: 10–15° off the sagittal plane, cephalomedially
- Does not traverse supraspinous/interspinous ligaments
Needle Types
- Cutting (Quincke): sharp bevel; easier to insert; higher PDPH rate; bevel should face cephalad (parallel to longitudinal dural fibres)
- Pencil-point (Whitacre, Sprotte, Gertie Marx): blunt tip, lateral opening; lower PDPH rate — preferred; slightly more resistance to insertion
- Gauge: 25–27G for ambulatory (lowest PDPH); 22G for children and difficult cases
Use of Ultrasound
Ultrasound can identify intervertebral levels, midline spinous processes, interspinous windows, and paramedian interlaminar windows. Particularly valuable in obese patients and those with difficult surface landmarks. Bone casts hypoechoic acoustic shadows; interspinous windows appear as an absence of shadows.
Dermatomal Requirements for Common Surgeries
| Surgery | Minimum Level |
|---|---|
| Perineal/saddle | S1–S5 |
| Lower limb (below knee) | T12 |
| Hip surgery | T10 |
| TURP / lower abdominal | T10 |
| Caesarean section | T4–T6 |
| Intra-abdominal (peritoneum) | T4 |
| Upper abdominal | T4 |
(Miller's Anesthesia, 10e)
10. Complications
Hypotension
- Most common complication; incidence up to 33% in non-obstetric and >80% in obstetric cases without prophylaxis
- Mechanism: sympathectomy → vasodilation → reduced venous return → reduced CO
- Management: IV fluid preloading or co-loading, vasopressors (phenylephrine first-line in obstetrics to maintain uteroplacental flow; ephedrine for bradycardia-associated hypotension), left uterine displacement in pregnancy
Post-Dural Puncture Headache (PDPH)
- Caused by CSF leak through dural hole → reduced CSF pressure → traction on pain-sensitive structures
- Character: postural — worse upright, relieved supine; often with neck stiffness, photophobia, diplopia
- Risk factors (Box 41.2 from Miller's):
- Younger age, female sex, pregnancy
- Larger needle gauge, cutting needle design
- Multiple punctures
- Treatment:
- Conservative: supine position, hydration, caffeine, analgesics, sumatriptan
- Definitive: epidural blood patch (15–20 mL autologous blood at or below the culprit level) — ~90% initial improvement, 61–75% persistent resolution; best performed ≥24 h after dural puncture
Transient Neurological Symptoms (TNS)
- Traditionally associated with lidocaine (incidence 10–40%), especially in lithotomy position
- Bilateral buttock/thigh pain without neurological deficit, appearing 12–24 h post-block, resolving within 1 week
- Mechanism unclear; may involve direct neurotoxicity
- Modern chloroprocaine preparations have similar TNS risk to lidocaine; bupivacaine TNS risk is low
Total Spinal / High Spinal
- Excessive rostral spread of intrathecal LA (or epidural drug entering subarachnoid space)
- Features: profound hypotension, bradycardia → possible cardiac arrest; progressive respiratory paralysis → apnoea; loss of consciousness; dilated pupils
- Management: immediate airway management (intubation), CPR if needed, vasopressors (epinephrine for cardiovascular collapse), left uterine displacement in pregnant patients
Urinary Retention
- S2–S4 block inhibits detrusor contractility; opioid additives worsen this
- Resolves spontaneously when block regresses below S2–3
- Intrathecal morphine strongly associated; routine catheterisation not recommended for hip/knee arthroplasty
Pruritus
- Most common opioid side effect: 30–100% incidence
- Mechanism: central μ-receptor activation, not histamine release
- Treatment: naloxone, nalbuphine, ondansetron, propofol; reducing sufentanil dose to 1.5 mcg reduces pruritus without compromising analgesia
Shivering
- Incidence up to 55%; less severe than with epidural (profound motor block limits shivering)
- Prevention: pre-warm with forced-air warmer ≥15 min; avoid cold IV/epidural fluids; intrathecal fentanyl or meperidine
Neuraxial Haematoma
- Rare but catastrophic; risk increased with anticoagulation
- ASRA Fourth Edition guidelines define mandatory intervals between anticoagulant doses and neuraxial procedures
- Presents as new or progressive neurological deficit, severe back pain
- Requires urgent MRI and surgical decompression within 8 h of symptom onset for best outcome
Meningitis / Epidural Abscess
- Bacterial (usually Streptococcus from provider's oropharynx — strict aseptic technique required) or aseptic
- Requires fever, headache, meningismus, culture/CSF analysis, antibiotics
Cauda Equina Syndrome
- Rare; associated with concentrated LA (5% lidocaine), small-bore catheter for continuous spinal, maldistribution of drug
- Permanent sacral nerve deficit: bladder/bowel dysfunction, perineal anaesthesia, lower limb weakness
(Miller's Anesthesia, 10e; Barash, 9e; Morgan & Mikhail, 7e)
11. Special Situations
Obstetrics (Caesarean Section)
- Spinal anaesthesia is the technique of choice in most centres for elective CS
- Standard: hyperbaric bupivacaine 0.5% (10–12.5 mg) + intrathecal fentanyl (15–25 mcg) + morphine (100 mcg)
- Target level: T4 bilaterally (loss of sensation to cold at the xiphisternum)
- Hypotension prevention: phenylephrine infusion + IV co-loading; left uterine displacement
Paediatric Spinal
- Main indication: inguinal hernia repair in ex-premature infants (<60 weeks post-conceptual age) to avoid post-operative apnoea from general anaesthesia
- Failure rate up to 20% — general anaesthesia must be available as backup
- Higher LA doses per kg required (larger CSF volume relative to body weight)
- Haemodynamic instability unusual in children <5 years (immature sympathetic system)
- Drug of choice: hyperbaric tetracaine or bupivacaine
Ambulatory Surgery
- Prefer short-acting agents: chloroprocaine (30–60 mg) — fastest discharge readiness (76 min faster than bupivacaine in one study)
- Avoid lidocaine (TNS risk), avoid bupivacaine (prolonged motor block)
- Low-dose fentanyl (10–25 mcg) added to reduce LA dose while minimising delay to discharge
Continuous Spinal Anaesthesia
- Catheter placed in subarachnoid space (usually via 28G microcatheter after intentional dural puncture with Tuohy needle)
- Indications: uncertain surgical duration, severe cardiac disease (incremental dosing → haemodynamic stability), failed single-shot
- Risk: cauda equina syndrome with maldistribution of concentrated LA
(Miller's Anesthesia, 10e; Morgan & Mikhail, 7e; Barash, 9e)
12. Combined Spinal–Epidural (CSE)
- Needle-through-needle technique: spinal injection followed by epidural catheter placement at the same interspace
- Advantages: rapid dense block from spinal component; indefinite duration from epidural catheter; lower total drug dose
- Disadvantages: cannot confirm epidural catheter function before the spinal wears off; epidural saline injection raises intrathecal pressure, increasing block height unpredictably
- Indications: labour analgesia (especially walking epidural), prolonged surgery, cases where duration is uncertain
13. Anticoagulation and Neuraxial Techniques (ASRA 2018 Guidelines — Key Points)
| Drug | Interval Before Spinal | Interval Before Removing Catheter | Restart After |
|---|---|---|---|
| LMWH prophylactic | 12 h | 12 h | 4 h |
| LMWH therapeutic | 24 h | 24 h | 4 h |
| Unfractionated heparin infusion | 4–6 h (check aPTT) | 4 h (check aPTT) | 1 h |
| Warfarin | INR ≤1.4 | INR ≤1.5 | — |
| Aspirin | No mandatory wait | No mandatory wait | — |
| Clopidogrel | 7 days | 7 days | — |
| Novel oral anticoagulants | 72 h (renal-dependent) | 6 h | 6 h |
(Miller's Anesthesia, 10e — Table 41.1, from Horlocker et al. 2018)
Summary
Spinal anaesthesia is a safe, reliable, and cost-effective technique for procedures below the mid-thoracic level. Its success depends on understanding the anatomy and the pharmacology of baricity and drug choice, anticipating and managing cardiovascular effects proactively, and selecting appropriate patients. The major determinants of block height are CSF volume and baricity, while dose is the primary determinant of duration. Complications range from the common and manageable (hypotension, PDPH, pruritus) to the rare but life-threatening (total spinal, haematoma, cauda equina syndrome), all of which are reduced by meticulous technique, appropriate patient selection, and adherence to anticoagulation guidelines.
Sources: Miller's Anesthesia 10e (primary), Barash Clinical Anesthesia 9e, Morgan & Mikhail's Clinical Anesthesiology 7e
This is a shared conversation. Sign in to Orris to start your own chat.