Heart block
Reading File
Finding Sources
Finding Sources
Searching PubMed
"atrioventricular block" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information to deliver a thorough answer on heart block. Let me compile it:
Heart Block (Atrioventricular Block)
Heart block refers to a disturbance in impulse conduction between the atria and ventricles through the AV junction. It must be distinguished from interference - a normal phenomenon where conduction is blocked simply due to physiologic refractoriness after a preceding impulse. True AV block exists when the atrial impulse is conducted with delay or fails entirely when the AV junction is not physiologically refractory.
Anatomy of the Conduction System
The only normal pathway for impulses to travel from atria to ventricles is through the AV bundle (Bundle of His). Block can occur at three levels:
- The AV node
- The His bundle itself
- The bundle branches (intraventricular/infranodal block)
The level of block has important prognostic implications - nodal block tends to be more benign, while infranodal (His-Purkinje) block is more serious.
Classification
AV block is classified by severity into three degrees:
| Classification | AV Conduction | ECG Findings | Clinical Features | Treatment |
|---|---|---|---|---|
| 1st degree | 1:1 (all conducted) | PR interval > 0.20 sec; narrow QRS | Usually asymptomatic | None (avoid nodal-blocking agents) |
| 2nd degree Mobitz I (Wenckebach) | Intermittent | PR progressively lengthens until a P wave drops; PR resets after dropped beat; narrow QRS (<0.12 sec) | Associated with inferior MI; rarely progresses to 3rd degree | Observation or atropine |
| 2nd degree Mobitz II | Intermittent | Fixed PR interval, then sudden dropped QRS; QRS often widened (BBB pattern due to infranodal damage) | Associated with anterior MI; frequently progresses to 3rd degree | Pacemaker |
| 3rd degree (complete) | None | P waves and QRS completely dissociated; ventricular rate depends on escape pacemaker | Bradycardia, hypotension, syncope, sudden death | Pacemaker |
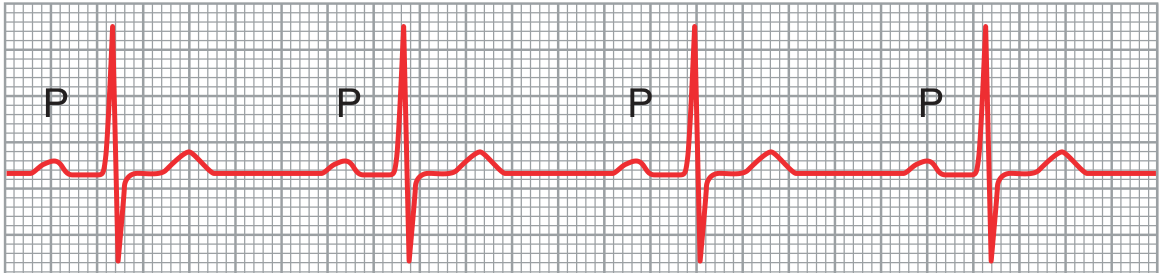
First-Degree AV Block
Every atrial impulse reaches the ventricles but with delay - the PR interval exceeds 0.20 seconds in adults. PR intervals as long as 1.0 second have been reported. The site of delay is almost always the AV node when the QRS is narrow. If the QRS shows a bundle branch block pattern, delay can be in the His-Purkinje system and a His bundle electrogram is needed to localize it. First-degree block is a normal variant in up to 2% of healthy young adults and requires no specific treatment.
ECG - First-Degree AV Block (Guyton & Hall):
Second-Degree AV Block
Some atrial impulses fail to reach the ventricles. The conduction ratio (e.g., 3:2, 4:3, 2:1) describes P waves to QRS complexes.
Type I - Mobitz I (Wenckebach)
- Progressive lengthening of the PR interval until a P wave is blocked (dropped beat), then the cycle resets
- The R-R interval actually shortens before the dropped beat (increment in PR gets smaller each cycle)
- Reflects progressive fatigue of conduction within the AV node
- Often associated with increased vagal tone, inferior MI, or drug effects (digoxin, beta-blockers)
- Generally benign; rarely progresses to complete block
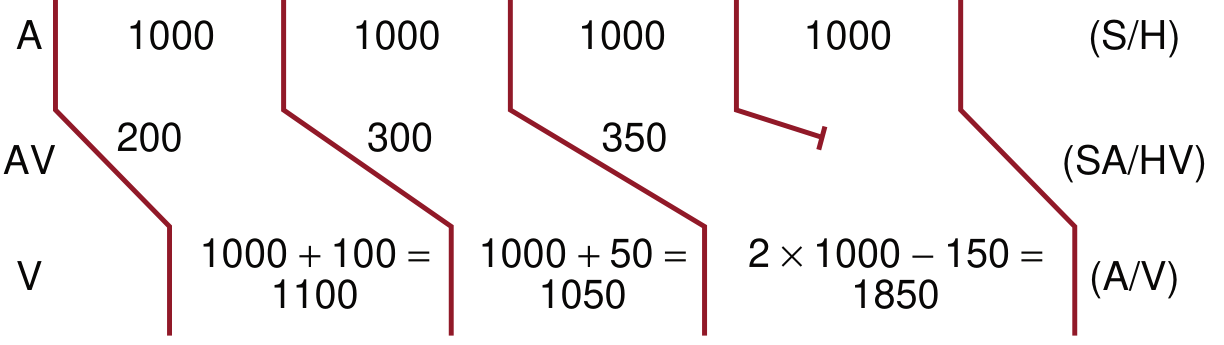
Ladder diagram of a 4:3 Wenckebach cycle:
Type II - Mobitz II
- Fixed PR interval with sudden, unexpected failure of a P wave to conduct
- Located below the AV node (His bundle or bundle branches)
- QRS is often wide (bundle branch block pattern) indicating extensive infranodal disease
- Associated with anterior MI; carries a high risk of progressing to complete heart block
- Requires pacemaker implantation
2:1 AV Block
- A special case where every other P wave is blocked - cannot be classified as Mobitz I or II on ECG alone
- Narrow QRS with slower atrial rate suggests nodal (Mobitz I); wide QRS suggests infranodal (Mobitz II)
Third-Degree (Complete) AV Block
No atrial impulses reach the ventricles. The atria and ventricles beat completely independently (AV dissociation). The ventricular rate is maintained by an escape pacemaker:
- Junctional escape (AV node/His bundle origin): rate 40-60 bpm, narrow QRS - more stable
- Ventricular escape (below the His): rate 20-40 bpm, wide QRS - less reliable, high risk of asystole
Clinical consequences include severe bradycardia, hypotension, dyspnea, angina, syncope (Stokes-Adams attacks), and sudden death. Requires urgent pacemaker insertion.
Etiology
Causes of AV block include:
- Fibrosis/degeneration of the conduction system (most common in the elderly - Lenegre's disease and Lev's disease)
- Ischemic heart disease - coronary insufficiency causing ischemia of the AV node or bundle
- Medications - beta-blockers, calcium channel blockers (verapamil, diltiazem), digoxin, adenosine, amiodarone
- Sarcoidosis - accounts for ~34% of unexplained 2nd/3rd degree AV block in patients under 60; 27% of these later develop VT or heart failure
- Inflammatory/infectious - rheumatic fever, Lyme disease, viral myocarditis, diphtheria, endocarditis
- Compression by scar tissue or calcified cardiac structures
- Hyperkalemia and other electrolyte disturbances
- Valvular heart disease - calcification extending into the conduction system
- Cardiac procedures - transcatheter aortic valve implantation (TAVI), cardiac surgery
- Vagal stimulation - carotid sinus hypersensitivity, increased vagal tone
- Neuromuscular diseases - myotonic dystrophy, Kearns-Sayre syndrome, Erb dystrophy
- Hypothyroidism, amyloidosis
Note: Most patients with AV block attributed to verapamil, diltiazem, or beta-blockers have underlying conduction disease - >80% will experience AV block even off the medications.
Clinical Features
- 1st degree: Asymptomatic; incidental ECG finding
- 2nd degree Mobitz I: Usually asymptomatic; may feel palpitations from "dropped beats"
- 2nd degree Mobitz II / 3rd degree: Symptomatic bradycardia - fatigue, dyspnea, presyncope, syncope (Stokes-Adams attacks), hypotension, angina, or sudden death
Diagnosis
AV block is diagnosed by ECG or monitoring. Criteria requiring treatment include:
- Third-degree AV block on any monitoring
- Advanced second-degree AV block (≥2 consecutively blocked P waves) with: symptoms, ventricular arrhythmias, asystole ≥3 seconds, escape rate <40 bpm, or infranodal escape rhythm
- Symptomatic second-degree AV block (regardless of type)
Management
Acute / Transient
- Atropine (0.5-1 mg IV) for symptomatic nodal block (1st or 2nd degree Mobitz I)
- Temporary transvenous pacing for hemodynamically unstable complete heart block or Mobitz II
- Treat reversible causes: withdraw offending drugs, correct hyperkalemia, treat ischemia/infection
Permanent Pacemaker - Class I Indications (pacemaker required)
| Condition | Specifics |
|---|---|
| 3rd-degree / advanced 2nd-degree with symptomatic bradycardia | Any cause |
| Asymptomatic 3rd-degree AV block with awake asystole >3 sec or escape rate <40 bpm | Or infranodal escape |
| Atrial fibrillation with pause ≥5 sec | |
| Post-operative AV block not expected to resolve | |
| Neuromuscular disease with AV block | Myotonic dystrophy, Kearns-Sayre, Erb |
| Asymptomatic 3rd-degree AV block with cardiomegaly/LV dysfunction | Or block below AV node |
| Chronic bifascicular block with advanced 2nd-degree or intermittent 3rd-degree AV block | |
| Post-MI: infranodal 3rd-degree or advanced 2nd-degree with BBB |
Permanent Pacemaker - Class IIa Indications (reasonable)
- Persistent 3rd-degree AV block with escape rate >40 bpm in asymptomatic adults without cardiomegaly
- Asymptomatic 2nd-degree infranodal AV block
- Asymptomatic Mobitz II with narrow QRS
- 1st or 2nd degree AV block with pacemaker-syndrome-like symptoms
- Bifascicular block with syncope (other causes excluded) or HV interval ≥100 ms
Key Distinguishing Points
| Feature | Mobitz I | Mobitz II |
|---|---|---|
| Site of block | AV node | Below AV node (His-Purkinje) |
| QRS width | Narrow | Often wide (BBB) |
| PR before dropped beat | Longest in cycle | Fixed (unchanged) |
| Association | Inferior MI, vagal tone | Anterior MI |
| Prognosis | Benign | High risk of complete block |
| Treatment | Usually none / atropine | Pacemaker |
Sources: Braunwald's Heart Disease (9780323722193); Goldman-Cecil Medicine (9780323930345); Guyton and Hall Textbook of Medical Physiology (9780443111013); Symptom to Diagnosis, 4th Ed. (9781260121117); Rosen's Emergency Medicine (9780323757898)
Atrial fibrillation.
Finding Sources
Searching PubMed
"atrial fibrillation"[MeSH Terms] AND management
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have everything needed for a thorough, well-structured answer. Let me compile it:
Atrial Fibrillation (AF)
AF is the most common sustained cardiac arrhythmia in clinical practice, affecting more than 2 million Americans. Prevalence rises sharply with age - about 1% of those over 60, 5% over 69, and ~12-18% of those over 75-85 years.
Definition and ECG Features
AF is characterized by rapid, completely disorganized atrial electrical activity (300-600 impulses/min) driven by multiple micro-reentry circuits, producing:
- No discernible P waves - replaced by a chaotic, irregular fibrillatory baseline (best seen in V1 and inferior leads)
- Irregularly irregular QRS complexes - the hallmark finding
- Ventricular rate in adults is typically 150-170 bpm (rarely exceeds this unless an accessory pathway is present)
ECG - Coarse Atrial Fibrillation (Goldman-Cecil Medicine):
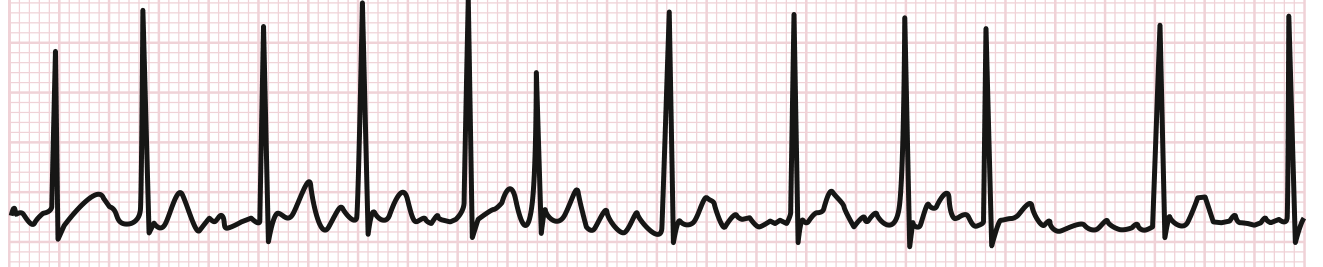
Important differential: AF can mimic a regular rhythm when complete AV block or VT coexists. A ventricular rate >200 bpm strongly suggests an accessory pathway (e.g., WPW) - do NOT use nodal blocking agents in that situation, as they can paradoxically accelerate ventricular response and precipitate VF.
Classification
| Type | Definition |
|---|---|
| Paroxysmal | Terminates spontaneously (usually within 48 h, by definition within 7 days) |
| Persistent | Lasts >7 days or requires cardioversion to terminate |
| Long-standing persistent | Continuous AF for >1 year |
| Permanent | AF accepted as the ongoing rhythm; no further attempts to restore sinus rhythm planned |
AF is almost always a recurrent disorder - the exception is AF arising from hyperthyroidism or cardiac surgery, which may resolve with treatment of the underlying cause.
Pathophysiology
AF requires two components:
1. Triggers
Atrial premature depolarizations - most commonly arising from the pulmonary veins (PVs) - initiate the arrhythmia. The muscular sleeves extending from the left atrium into the PVs have short refractory periods and exhibit both automatic and triggered activity. This is why pulmonary vein isolation is the cornerstone of catheter ablation.
2. Substrate
A susceptible atrial substrate sustains the arrhythmia via:
- Multiple-wavelet reentry (Moe's hypothesis) - multiple simultaneous reentrant circuits
- Rotor/focal driver activity - a small number of high-frequency rotating circuits or focal sources that drive the rest of the atrium into fibrillation
- Atrial remodeling - prolonged AF causes electrical remodeling (shortened atrial action potential due to downregulation of L-type Ca²+ current) and structural remodeling (fibrosis, gap junction remodeling), both of which perpetuate AF ("AF begets AF")
Ion Channel Abnormalities
- Gain-of-function mutations in IK (delayed rectifier K+ channels) shorten APD and atrial refractoriness, facilitating fibrillatory activity
- Mutations in KCNJ2, KCNA5, and the connexin-40 gene (GJA5) are linked to familial AF
- Genome-wide association studies have identified variants in HCN4, PRRX1, and CAV1
Hemodynamic Consequences
- Loss of atrial kick: In normal individuals, atrial contraction contributes ~15% of ventricular filling - this is usually well tolerated. In patients with stiff, non-compliant ventricles (aortic stenosis, hypertrophic cardiomyopathy, long-standing hypertension), up to 40% of filling depends on atrial contraction - these patients may develop acute pulmonary edema when AF starts
- Tachycardia-induced cardiomyopathy: Sustained rapid ventricular rates (>120 bpm for weeks) can cause biventricular dysfunction, which is often reversible with rate/rhythm control
Causes and Risk Factors
Cardiac causes:
- Hypertensive heart disease (most common)
- Ischemic heart disease / CAD
- Valvular disease (especially mitral)
- Cardiomyopathy (dilated, hypertrophic, restrictive)
- Heart failure (~one-third of HF patients have AF)
- Pericarditis
- Sick sinus syndrome
- WPW / accessory pathway
- Myocardial contusion / cardiac surgery
Systemic causes:
- Hyperthyroidism
- Obstructive sleep apnea
- Obesity
- Diabetes mellitus
- Pulmonary embolism
- Catecholamine excess
Lifestyle/Other:
- Acute alcohol intoxication ("holiday heart")
- Long-term significant alcohol use
- Vagally-mediated AF (post-exercise, after large meals)
- Excessive caffeine (rare)
- About 20% of patients have no identifiable comorbidity ("lone AF")
Clinical Manifestations
Symptoms include:
- Palpitations (most common in young patients; less prominent with chronic AF)
- Dyspnea, chest pain/discomfort
- Fatigue, reduced exercise tolerance
- Lightheadedness / presyncope
- Syncope - usually due to a conversion pause when AF terminates
Many patients are asymptomatic, particularly with chronic AF or when ventricular rate is controlled. Older patients especially may present atypically - acute pulmonary edema, fall, or stroke as the first manifestation.
Complications
1. Thromboembolism / Stroke
- Non-valvular AF is associated with a 5-fold increase in stroke risk
- Primary mechanism: thrombus formation in the left atrial appendage (LAA) during stasis, followed by embolization
- Even subclinical ("silent") AF carries a 2.5-fold increased risk of ischemic stroke
- Risk is independent of AF pattern (paroxysmal = persistent in stroke risk)
- ~12% of embolic events are extracranial (~70% to limbs, remainder to mesenteric circulation)
- AF is associated with a 1.4-fold higher risk of cognitive impairment and dementia
2. Heart Failure
- Tachycardia-induced cardiomyopathy with ventricular rates >120 bpm
3. Increased Mortality
- AF in older adults associated with decreased physical performance, shorter disability-free survival, and increased mortality
Stroke Risk Assessment: CHA₂DS₂-VASc Score
| Risk Factor | Points |
|---|---|
| C - Congestive heart failure | 1 |
| H - Hypertension | 1 |
| A₂ - Age ≥75 years | 2 |
| D - Diabetes mellitus | 1 |
| S₂ - Stroke / TIA (prior) | 2 |
| V - Vascular disease (prior MI, PAD, aortic plaque) | 1 |
| A - Age 65-74 years | 1 |
| Sc - Sex category (female) | 1 |
| Maximum | 9 |
Anticoagulation recommendations:
- Score ≥2: Anticoagulation indicated (DOAC preferred over warfarin)
- Score 1: Anticoagulation or no therapy (shared decision with patient)
- Score 0: No therapy required
- All patients ≥75 years automatically score ≥2 and are candidates for anticoagulation regardless of AF pattern
Diagnosis and Initial Workup
- ECG: Irregularly irregular rhythm, absent P waves, fibrillatory baseline - minimum 2 minutes required for diagnosis by convention
- Blood work: CBC, electrolytes, creatinine, TSH (thyroid-stimulating hormone), glucose
- Echocardiogram: Assess for ventricular dysfunction, valvular disease, left atrial size
- Stress test: Only if clinical suspicion of ischemia; not required routinely
- Transesophageal echocardiogram (TEE): Required before cardioversion if AF duration >48 hours without adequate anticoagulation - to exclude LAA thrombus
Management
Step 1 - Assess and Treat Reversible Causes
Hypoxia, fever, electrolyte abnormalities, thyrotoxicosis, infections, medications.
Step 2 - Anticoagulation (guided by CHA₂DS₂-VASc)
DOACs are strongly preferred over warfarin (equal or better stroke prevention, similar or less bleeding):
- Dabigatran (direct thrombin inhibitor)
- Rivaroxaban, apixaban, edoxaban (factor Xa inhibitors)
- Dose adjustment required based on age, weight, renal function (especially for dabigatran and edoxaban)
- Warfarin (INR 2-3): reserved for mechanical valves; bioprosthetic valve patients may use rivaroxaban
Special situations:
- Patients with AF + stable CAD: DOAC monotherapy preferred; if stented, DOAC + P2Y12 inhibitor (clopidogrel) without aspirin has lower bleeding risk
- Mechanical valves: warfarin required (DOACs contraindicated)
- Patients unable to take anticoagulation: LAA occlusion (WATCHMAN device) is a non-inferior alternative
Step 3 - Rate Control vs. Rhythm Control
Rate Control:
| Agent | Route | Notes |
|---|---|---|
| Metoprolol | IV / PO | First-line; also useful in HF with reduced EF |
| Esmolol | IV | Titratable; useful acutely |
| Diltiazem | IV / PO | Avoid in HFrEF |
| Verapamil | IV / PO | Avoid in HFrEF |
| Digoxin | PO | Third-line; less effective during exercise/adrenergic states |
| Amiodarone | IV/PO | When others fail; useful in acute HF |
Rate targets:
- Lenient control (<110 bpm at rest) is acceptable for asymptomatic patients with preserved LV function
- Strict control (<80 bpm at rest) is a Class IIa recommendation when symptoms persist
Rhythm Control:
Restoring and maintaining sinus rhythm is pursued when:
- Rate control fails to relieve symptoms
- Patient is hemodynamically unstable (cardiovert immediately)
- First episode with reasonable chance of success
- Patient preference
Pharmacologic cardioversion:
- Flecainide (300 mg PO - "pill-in-the-pocket") or propafenone (600 mg PO) - for paroxysmal AF without structural heart disease
- Amiodarone - preferred in structural heart disease or HF
- Ibutilide IV - for acute cardioversion in hospital setting
Electrical cardioversion (DC cardioversion):
- Synchronized DC shock (typically 100-360 J biphasic)
- If AF duration >48 hours: TEE to exclude LAA thrombus first, OR anticoagulate for ≥3 weeks before cardioversion (and continue for ≥4 weeks after, regardless of CHA₂DS₂-VASc - due to "stunning" of atrial mechanical function)
- For AF ≤48 hours or patient on therapeutic anticoagulation: cardioversion can proceed without TEE
Approach after cardioversion - "wait-and-see":
- About 50% of acute-onset AF converts spontaneously within 48-96 hours; a brief period of rate control with delayed cardioversion (if no spontaneous conversion by 48 hours) is as effective as early cardioversion at 1 month
Step 4 - Long-Term Rhythm Control Strategy
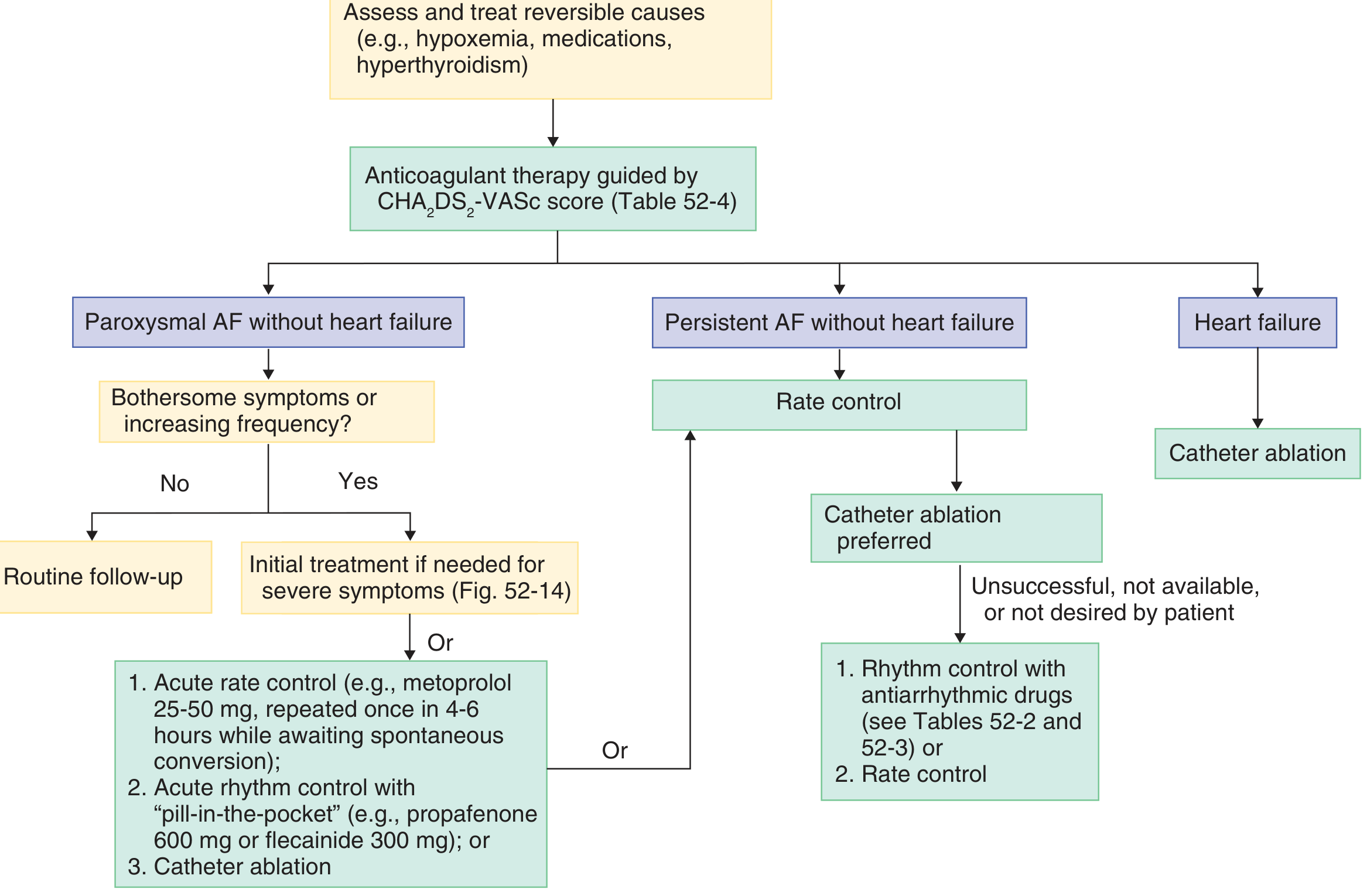
Treatment algorithm for recurrent AF:
Catheter Ablation
Pulmonary vein isolation (PVI) is the cornerstone of ablation:
- Success rates: 75-85% at 1 year for paroxysmal AF; 60-75% for persistent AF
- Reduces AF recurrence by 50-70% compared with antiarrhythmic drugs alone in symptomatic paroxysmal AF
- First-line ablation (without prior antiarrhythmic drug failure) results in similar or better outcomes and may be preferred
- For AF with heart failure: catheter ablation (but NOT antiarrhythmic drugs) is associated with reduced all-cause mortality and is the preferred initial therapy
- Early intervention may reduce progression from paroxysmal to permanent AF and reduce stroke/death
Complications (~2% overall risk):
- Atrial perforation / cardiac tamponade
- Thromboembolism
- Atrioesophageal fistula (rare but life-threatening)
- Phrenic nerve injury
- Pulmonary vein stenosis
- Left atrial macro-reentrant tachycardia (requiring repeat ablation)
AV node ablation + pacemaker: For refractory AF with uncontrolled ventricular rate despite maximal pharmacologic therapy - intentional complete AV block created, requiring permanent pacemaker; improves symptoms and LV function.
Ashman Phenomenon
A common ECG finding in AF - aberrant conduction of an early-arriving impulse following a long R-R interval (long-short cycle sequence), producing a wide QRS complex (typically RBBB pattern). Ashman beats can be mistaken for PVCs or runs of VT.
AF in Special Contexts
WPW / Accessory pathway:
- AF with anterograde accessory pathway conduction can produce rapid, irregularly irregular wide-complex tachycardia at >200 bpm
- AV nodal blocking agents (beta-blockers, calcium channel blockers, digoxin, adenosine) are contraindicated - they block the AV node but spare the accessory pathway, potentially accelerating ventricular response → VF
- Treatment: IV procainamide or ibutilide; electrical cardioversion if unstable
Post-cardiac surgery AF:
- Very common (~30-50% of CABG patients)
- Usually transient; beta-blockers and amiodarone are used for prophylaxis
Hypertrophic cardiomyopathy:
- AF is poorly tolerated due to heavy dependence on atrial kick
- Disopyramide and amiodarone are preferred antiarrhythmic agents; ablation considered for refractory cases
Prognosis
Paroxysmal AF often progresses to persistent and then permanent AF over years. AF is associated with increased mortality, largely driven by stroke, heart failure, and sudden death. Early rhythm control strategies, including catheter ablation, appear to reduce adverse outcomes compared with rate control alone in selected patients, particularly those with heart failure.
Recent evidence (2024-2025):
- The 2024 ESC Guidelines for AF management are the most current practice guidelines [PMID: 39210723]
- A meta-analysis of RCTs ([PMID: 38727662], JACC Clin Electrophysiol 2024) compared rhythm vs. rate control strategies
- For AF + stable coronary disease: anticoagulation alone (without antiplatelet) is supported by recent meta-analysis data [PMID: 39918465]
Sources: Braunwald's Heart Disease (9780323722193); Goldman-Cecil Medicine (9780323930345); Rosen's Emergency Medicine (9780323757898); Guyton & Hall Physiology (9780443111013); Symptom to Diagnosis, 4th Ed. (9781260121117)
JVP waves , NT - proBNP, PSVT
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
I have thorough content for all three topics. Let me now compile the full answer:
1. JVP Waves (Jugular Venous Pulse)
The JVP reflects right atrial pressure and provides non-invasive hemodynamic information. The internal jugular vein is used (not external, unless jugular venous valve insufficiency is present). JVP height is measured by adding 5 cm to the height of observed distention above the sternal angle of Louis (normal: 5-10 cm H₂O).
Timing tip: The a wave precedes the carotid upstroke and S1. Once identified, the next positive deflection is the v wave. Never use the radial pulse as reference (delayed vs. carotid); use carotid palpation with the contralateral hand or simultaneous auscultation.
Normal JVP Waveform Components
JVP tracing with heart sounds showing A, C, X, V, Y components:
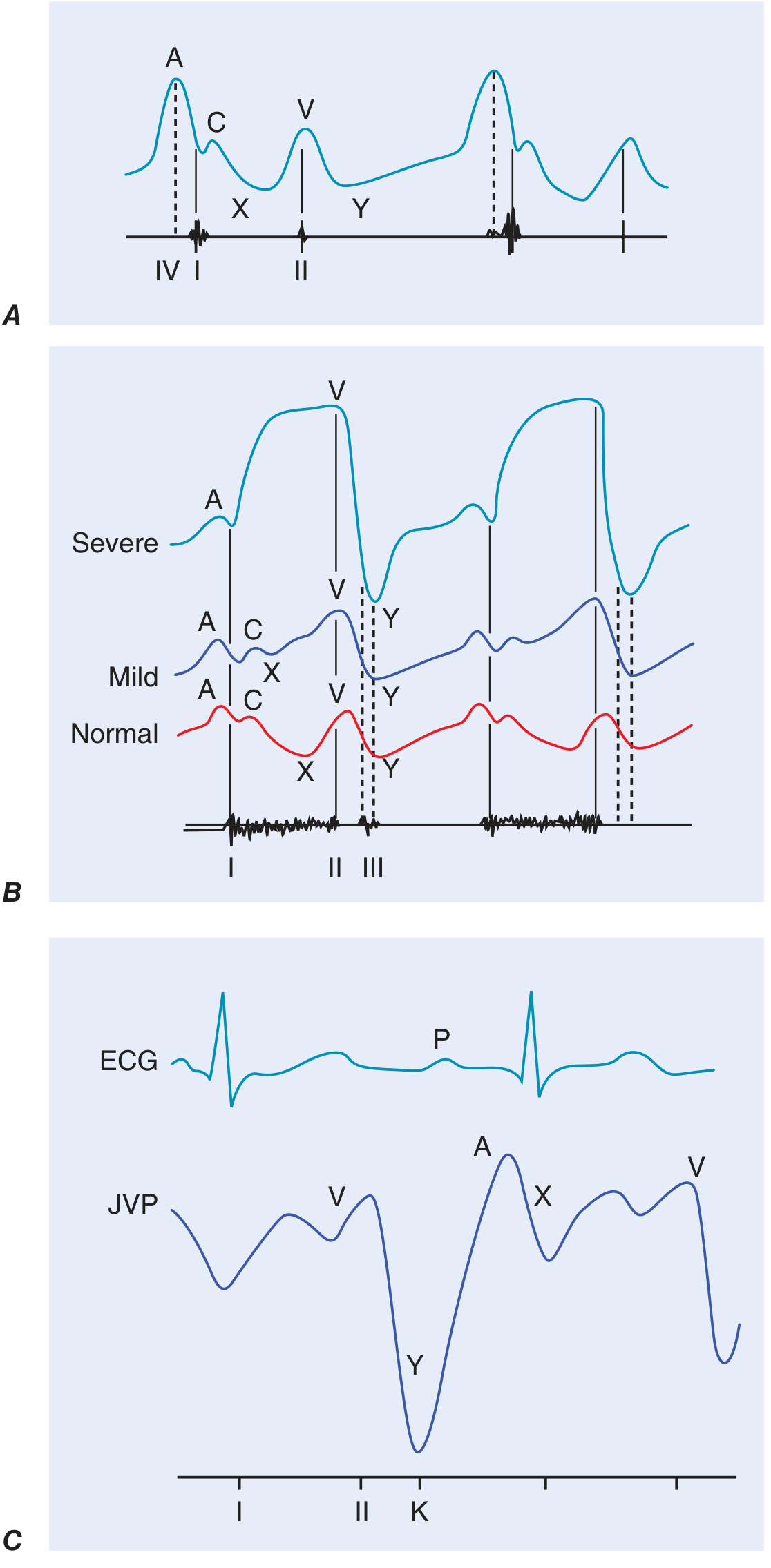
| Component | Mechanism | Timing | ECG Correlation |
|---|---|---|---|
| a wave | Right atrial presystolic contraction | Just after P wave, before S1 | After P wave |
| c wave | Tricuspid valve bulging into RA during early ventricular systole (also partly carotid pulsation artifact) | After S1 | After QRS begins |
| x descent | Right atrial relaxation + downward displacement of tricuspid annulus during ventricular systole | After a wave / c wave; during systole | - |
| v wave | Venous return to RA while tricuspid valve is closed (atrial diastole during ventricular systole) | During ventricular systole, peaks at S2 | After T wave |
| y descent | Tricuspid valve opens → early RV diastolic filling | After v wave peak | - |
In normal persons, the a wave is larger than the v wave.
Abnormalities of Each Component
A Wave Abnormalities
| Finding | Cause | Mechanism |
|---|---|---|
| Large/prominent a wave | Pulmonary hypertension, pulmonary stenosis, RV diastolic dysfunction, restrictive cardiomyopathy | Increased RA contraction against stiff/non-compliant RV |
| Giant a wave | Tricuspid stenosis | Atrial contraction against stenotic valve |
| Cannon a waves (irregular, variable) | Complete heart block | RA contracts against closed tricuspid valve (AV dissociation) - diagnostic of VT in wide-complex tachycardia |
| Cannon a waves (regular) | AVNRT, junctional rhythm | RA and RV contract simultaneously |
| Absent a wave | Atrial fibrillation | No organized atrial contraction |
Key clinical pearl: Variable cannon a waves in bradycardia = complete heart block. Regular cannon a waves in narrow tachycardia = AVNRT. Cannon a waves in wide-complex tachycardia = ventricular tachycardia (not aberrancy).
In atrial flutter, small regular flutter waves may be seen instead of a waves.
X Descent Abnormalities
| Finding | Cause |
|---|---|
| Blunted/absent x descent | Atrial fibrillation (loss of atrial relaxation); myopathic diseases with reduced annular motion; tricuspid regurgitation (positive v wave replaces x descent) |
| Deep x descent | Constrictive pericarditis (enhanced annular descent + preserved atrial relaxation) |
V Wave Abnormalities
| Finding | Cause |
|---|---|
| Large v wave | Tricuspid regurgitation (TR) - retrograde systolic flow into RA; also RV failure, VSD |
| "Ventriculrized" waveform | Severe TR - v wave merges with c wave; rapid y descent follows |
Y Descent Abnormalities
| Finding | Cause |
|---|---|
| Blunted/slow y descent | Tricuspid stenosis, cardiac tamponade (obstruction to RV filling) |
| Deep/rapid y descent | Constrictive pericarditis, severe TR |
Special Signs
- Kussmaul's sign: Rise (or failure to fall) in JVP with inspiration. Classic in constrictive pericarditis; also in restrictive cardiomyopathy, massive PE, RV infarction, advanced LV systolic HF
- Abdominojugular reflux: Sustained rise >3 cm in JVP with firm RUQ pressure for >15 sec = positive; predicts pulmonary artery wedge pressure >15 mmHg in HF
- Normal response: JVP falls ≥3 mmHg within 15 seconds
Disease-Specific JVP Patterns Summary
| Condition | Pattern |
|---|---|
| Tricuspid regurgitation | Absent x, large v wave, rapid y descent; "ventriculrized" waveform |
| Tricuspid stenosis | Giant a wave, slow y descent |
| Cardiac tamponade | Blunted y descent, preserved x descent; pulsus paradoxus |
| Constrictive pericarditis | Deep x AND deep y descents ("W" or "M" pattern); Kussmaul's sign |
| Atrial fibrillation | Absent a wave, blunted x descent |
| Complete heart block | Variable cannon a waves |
| Pulmonary hypertension | Prominent a wave, elevated JVP |
| RV infarction | Elevated JVP + clear lungs + hypotension (Bezold-Jarisch triad) |
2. NT-proBNP (N-Terminal Pro-Brain Natriuretic Peptide)
Biochemistry
BNP (B-type / Brain Natriuretic Peptide) is a neurohormone synthesized primarily in ventricular cardiomyocytes in response to increased wall stress (volume overload, pressure overload). The precursor proBNP (108 amino acids) is cleaved by corin and other proteases into:
- BNP (32 aa) - the biologically active peptide
- NT-proBNP (76 aa) - the inactive N-terminal fragment
Both are released in equimolar amounts, but NT-proBNP has a longer half-life (~120 min vs. ~20 min for BNP) and higher circulating concentrations. Importantly, BNP is cleaved by neprilysin (hence sacubitril/valsartan raises BNP levels - NT-proBNP is NOT a neprilysin substrate and can be used to monitor HF in patients on sacubitril/valsartan).
Clinical Actions of BNP
- Promotes natriuresis and diuresis
- Vasodilation
- Inhibits the renin-angiotensin-aldosterone system
- Anti-fibrotic, anti-hypertrophic effects
Diagnostic Use
Diagnosing Acute Heart Failure in the ED (Acute Dyspnea)
Key trial: PRIDE study (ProBNP Investigation of Dyspnea in the Emergency Department)
| Cutoff | Use |
|---|---|
| NT-proBNP <300 pg/mL | Excludes acute decompensated HF (high negative predictive value) |
| NT-proBNP ≥900 pg/mL | Comparable performance to BNP 100 pg/mL for diagnosis of HF |
| Age-stratified positive cutoffs | Improves PPV: younger patients have lower thresholds; older patients have higher expected baseline values |
For BNP: cutoff of 100 pg/mL (Breathing Not Properly trial) is highly accurate for acute decompensated HF.
Age-Stratified NT-proBNP Cutoffs (ICON study)
| Age | Positive cutoff |
|---|---|
| <50 years | 450 pg/mL |
| 50-75 years | 900 pg/mL |
| >75 years | 1800 pg/mL |
| All ages - Rule out | <300 pg/mL |
Outpatient Setting
- NT-proBNP values are considerably lower in stable outpatients
- ED cutoffs should NOT be applied; use lower thresholds optimized for negative predictive value (ruling out HF)
Prognostic Use
- BNP/NT-proBNP levels provide prognostic information across all ACC/AHA stages of HF, even after adjusting for history, physical exam, echo, and exercise testing
- Serial measurements add incremental prognostic value
- Failure to decrease BNP/NT-proBNP by ≥30% at hospital discharge predicts higher morbidity/mortality
- Chronically elevated or rising natriuretic peptide levels = high-risk patient
- HF therapies that lower natriuretic peptides are associated with improved prognosis
Factors Affecting Levels
| Increases NT-proBNP | Decreases NT-proBNP |
|---|---|
| Age | Obesity (reduced secretion) |
| Renal dysfunction (reduced clearance) | Flash pulmonary edema (may not yet be elevated) |
| Pulmonary hypertension | Neprilysin inhibitors (affect BNP but NOT NT-proBNP) |
| Sepsis, PE, critical illness | Effective HF treatment |
| AF, RV dysfunction | - |
| Cardiac tamponade, constrictive pericarditis | - |
BNP is sensitive (~95-99%) but less specific (~50-60%) for HF. Always interpret in clinical context - natriuretic peptides supplement but do not replace clinical judgment.
Key Distinction: BNP vs. NT-proBNP
| Feature | BNP | NT-proBNP |
|---|---|---|
| Activity | Biologically active | Inactive fragment |
| Half-life | ~20 min | ~120 min |
| Neprilysin substrate | Yes (sacubitril raises BNP) | No |
| Use with sacubitril/valsartan | Cannot monitor HF | Can monitor HF |
| Lower cutoff (rule out, acute) | 100 pg/mL | 300 pg/mL |
3. PSVT (Paroxysmal Supraventricular Tachycardia)
Definition
PSVT is a clinical syndrome of rapid, regular tachycardia with abrupt onset and abrupt termination. The term encompasses all supraventricular tachycardias except AF, atrial flutter, and multifocal AT - those that depend on the AV node for their circuit.
Mechanisms and Types
| Type | Proportion | Mechanism |
|---|---|---|
| AVNRT (AV nodal reentrant tachycardia) | ~60-80% | Reentry within the AV node using fast and slow pathways |
| AVRT (AV reentrant tachycardia - orthodromic) | ~15-20% | Reentry via accessory pathway (anterograde AV node, retrograde accessory) |
| Atrial tachycardia (focal AT) | ~5-10% | Ectopic atrial focus with enhanced automaticity or triggered activity |
AVNRT (most common)
The AV node has two pathways:
- Slow pathway: slower conduction, shorter refractory period
- Fast pathway: faster conduction, longer refractory period
In typical (slow/fast) AVNRT: anterograde conduction via slow pathway, retrograde via fast pathway. This produces near-simultaneous atrial and ventricular activation - P wave is buried in or just after the QRS.
In atypical AVNRT: anterograde fast, retrograde slow - P wave visible before QRS (long RP tachycardia).
ECG Features
| Feature | Typical AVNRT finding |
|---|---|
| Rate | 150-250 bpm (usually 170-180 bpm; range 130-300) |
| Rhythm | Regular |
| P waves | Absent/buried in QRS (~70%) or retrograde P just after QRS (<70ms RP); inverted in II, III, aVF |
| QRS | Narrow (<100 ms), unless aberrant conduction |
| Onset/offset | Abrupt ("paroxysmal") |
A pseudo-R' in V1 or pseudo-S in inferior leads (retrograde P distorting the QRS end) is a classic ECG sign of AVNRT.
Clinical Features
- More common in females
- Peak incidence in late teens and young adults
- Majority without structural heart disease
- Symptoms: palpitations (prominent, often "pounding in throat" due to cannon a waves), lightheadedness, dyspnea, chest discomfort, anxiety, near-syncope
- Patients can often describe exact onset and self-termination
Management
Treatment algorithm for regular narrow-complex tachycardia (Harrison's 2025):
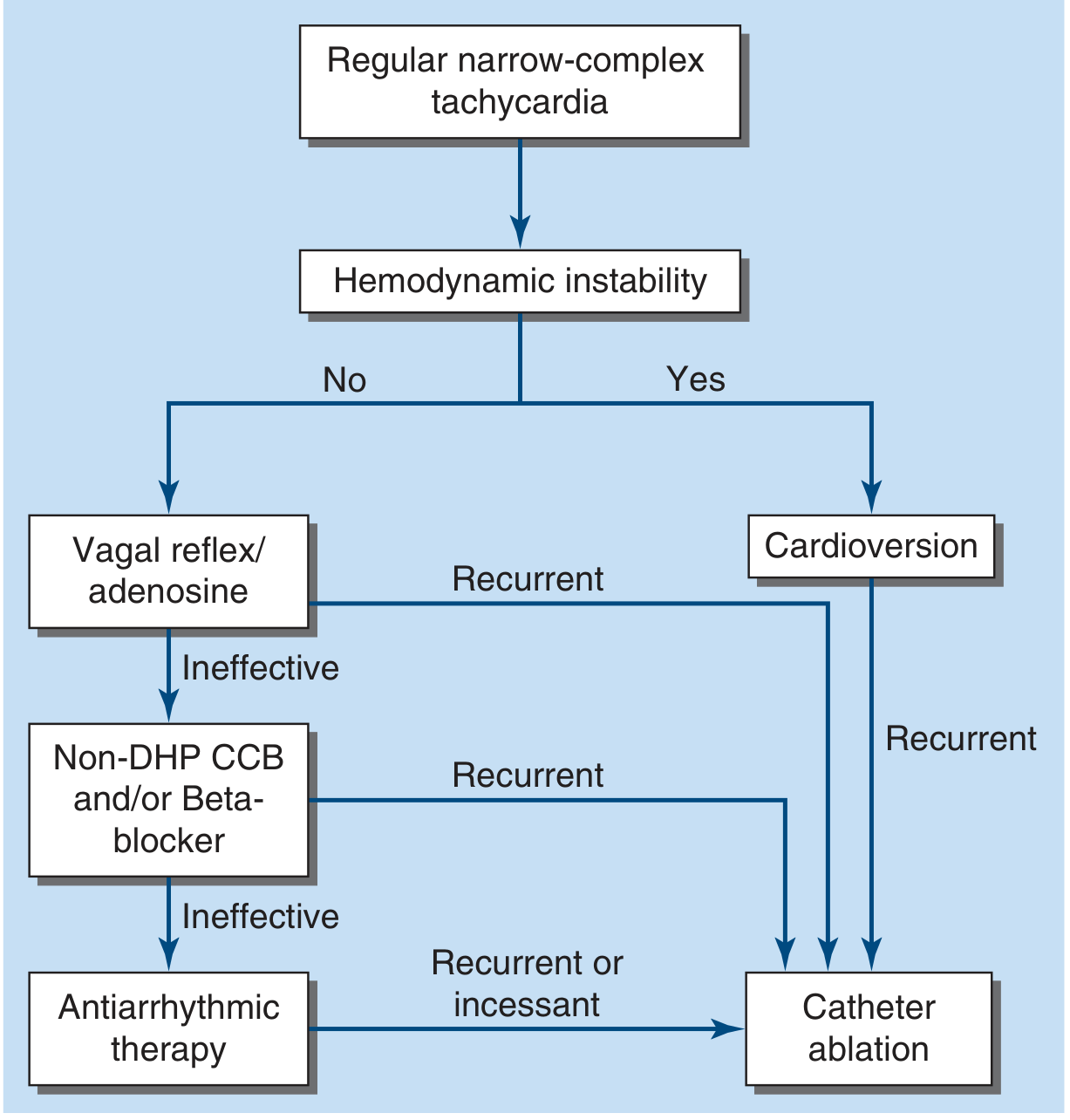
Acute Management
Step 1 - Vagal maneuvers (first-line for stable patients):
- Valsalva maneuver - patient bears down; modified supine Valsalva (legs elevated after straining) has higher success (~43% vs ~17%)
- Carotid sinus massage - only if no carotid bruits, no prior stroke history
- Success is often related to how early in the episode they are applied
Step 2 - IV Adenosine (if vagal maneuvers fail):
- Dose: 6 mg rapid IV bolus; repeat with 12 mg if no effect
- Mechanism: transiently blocks AV node conduction, terminating AV-node-dependent tachycardias
- Onset: within seconds; half-life: ~10 sec
- Side effects: chest pain, dyspnea, anxiety, flushing (transient, ~10-15 sec)
- Contraindications: cardiac transplant (hypersensitivity), severe asthma (relative), WPW with anterograde pre-excitation (may precipitate AF → VF)
- Precipitates AF in ~15% of cases - use cautiously in WPW
- Diagnostic use: if adenosine produces AV block but tachycardia continues (ongoing P waves exposed), the mechanism is AT or atrial flutter - not AV-dependent reentry
Step 3 - IV Non-DHP CCB or Beta-blocker (if adenosine fails):
- Verapamil 5-10 mg IV, or diltiazem IV
- Metoprolol IV
- May cause hypotension; have longer duration of action than adenosine
- Can also be given orally as "pill-in-the-pocket" for out-of-hospital self-treatment
Step 4 - Hemodynamically unstable: Synchronized DC cardioversion immediately
Chronic/Long-Term Management
- Catheter ablation (preferred for recurrent symptomatic PSVT):
- AVNRT: slow pathway ablation - success rate ~95-98%; risk of complete AV block ~0.5-1%
- AVRT: accessory pathway ablation
- First-line for patients who prefer cure over ongoing drug therapy
- Antiarrhythmic drugs for those who decline ablation or as a bridge:
- Flecainide, propafenone (no structural heart disease)
- Diltiazem, verapamil, beta-blockers (rate-control + prevention)
- Amiodarone (structural heart disease, last resort due to toxicity)
Wide-Complex PSVT
- Treat as VT until proven otherwise
- If clearly PSVT with aberrancy (prior documented episodes): vagal maneuvers + adenosine reasonable
- If irregular wide-complex: likely preexcited AF/flutter → cardioversion, IV procainamide, or ibutilide
- Never use adenosine, verapamil, or diltiazem in preexcited AF (anterograde accessory pathway conduction - risk of VF)
Sources: Harrison's Principles of Internal Medicine 22E (9781265977061); Fuster and Hurst's The Heart, 15th Ed. (9781264257560); Goldman-Cecil Medicine (9780323930345); Braunwald's Heart Disease (9780323722193); Tintinalli's Emergency Medicine (9781260019933)
Insulin classification, miliary TB , pyrexia of unknown Origin ,, irregular pulse, myxoedema coma
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have thorough content for all five topics. Let me compile the complete answer:
1. Insulin Classification
Insulins are classified by their onset, peak, and duration of action. The goal is to mimic physiologic insulin secretion: basal insulin for fasting/overnight hepatic glucose regulation, and prandial (bolus) insulin for postmeal glucose control.
Classification Table
| Category | Examples | Onset | Peak | Duration | Use |
|---|---|---|---|---|---|
| Rapid-acting analogues | Lispro (Humalog), Aspart (NovoLog), Glulisine (Apidra) | 5-15 min | 30-90 min | 3-5 h | Prandial; inject <10 min before meal (or just after in gastroparesis) |
| Inhaled rapid-acting | Technosphere insulin (Afrezza) | 12-15 min | 30 min | 3 h | Faster onset than SC rapid-acting; requires FEV1 monitoring; contraindicated in lung disease/smokers |
| Short-acting (Regular) | Regular insulin (Humulin R, Novolin R) | 30-60 min | 2-4 h | 5-8 h | Prandial; inject 30-45 min before meals; also IV infusions (DKA, surgery) |
| Intermediate-acting | NPH (Humulin N, Novolin N) | 2-4 h | 4-10 h | 12-18 h | Basal (twice daily); mixed with regular in combination pens |
| Long-acting analogues | Glargine (Lantus, Basaglar), Detemir (Levemir) | 1-2 h | Peakless (glargine) | 20-24 h | Once-daily basal; glargine has no pronounced peak - less nocturnal hypoglycemia |
| Ultra-long-acting | Degludec (Tresiba) | 30-90 min | Peakless | >42 h | Once-daily basal; very flat profile; flexibility in dosing time |
Combination Insulins
Pre-mixed products contain a fixed ratio of NPH + rapid/short-acting:
- 70/30 - 70% NPH + 30% regular
- 50/50 - 50% NPH + 50% regular
- 75/25 - 75% NPH protamine lispro + 25% lispro
- Degludec/aspart (Ryzodeg) - ultra-long + rapid
Combination insulins are convenient (2 injections/day) but cannot independently adjust short and long components - not appropriate for Type 1 DM management.
Key Clinical Points
- Rapid-acting analogues should be injected <10 min before meals (regular: 30-45 min before)
- Basal insulin (glargine, degludec) provides ~50% of daily insulin requirements; prandial provides the other 50%
- Type 1 DM: typically 0.4-1.0 units/kg/day total, split between basal and prandial
- Glargine vs. degludec: Both peakless; degludec has longer duration and is more flexible in dosing time
- Exogenous insulin enters the systemic (not portal) circulation → subphysiologic hepatic insulin levels; higher peripheral levels needed → no current regimen perfectly mimics pancreatic secretion
- Inhaled insulin: faster onset than SC; requires FEV1 screening; can cause bronchospasm/cough
Basal-Bolus (MDI) Regimen
The most physiologic approach:
- Basal: once-daily glargine or degludec (dose adjusted to fasting glucose)
- Prandial bolus: rapid-acting (aspart/lispro/glulisine) before each meal, dosed by an insulin-to-carbohydrate ratio (commonly 1 unit per 10-15 g carbohydrate in Type 1 DM) plus correction dose for premeal hyperglycemia
2. Miliary Tuberculosis
Definition and Origin of the Term
"Miliary" derives from the Latin milium (millet seed) - referring to the gross pathological appearance of the lung studded with numerous small (~2 mm), yellow-white foci resembling millet seeds. Miliary TB represents wide hematogenous dissemination of Mycobacterium tuberculosis either during primary infection or reactivation disease.
Pathogenesis
Miliary disease occurs when bacilli enter the bloodstream and seed multiple organs simultaneously:
- During primary TB: early hematogenous seeding occurs in ~95% of cases but is controlled by cell-mediated immunity. When immunity is overwhelmed, widespread disseminated disease results
- During secondary (reactivation) TB: miliary pulmonary disease occurs when organisms draining through lymphatics enter the venous blood and circulate back to the lung - often in the setting of immunosuppression
- Histology: caseating or non-caseating granulomas with Langhans giant cells at multiple sites; immunocompromised patients may fail to form characteristic granulomas
Who Is at Risk
- Children (especially <5 years)
- Elderly
- Immunocompromised: HIV/AIDS (CD4 <200), organ transplant, anti-TNF therapy
- Malnutrition, diabetes, chronic kidney disease, hematologic malignancies
- Post-primary immunosuppression (steroids, biologics)
Clinical Features
Miliary reactivation - chronic, non-specific course:
- Prolonged fever, night sweats, anorexia, weight loss
- Dry cough, progressive dyspnea
- Splenomegaly, lymphadenopathy
- Hepatomegaly (hepatic involvement)
- Signs of multisystem illness
Miliary primary TB - more acute and severe:
- Can present with multiorgan failure, septic shock, ARDS
- Higher mortality than reactivation miliary TB
Special findings:
- Choroidal tubercles (on fundoscopy) - pathognomonic for miliary TB; present in ~13% of cases
- Cutaneous involvement: papules or vesiculopapules (tuberculosis cutis miliaris disseminata) - more common in HIV patients
- Meningitis may coexist (miliary TB frequently seeds the meninges)
- Adrenal involvement → Addison's disease
Investigations
| Test | Finding |
|---|---|
| CXR / CT chest | Diffuse bilateral 1-3 mm nodules ("snowstorm" pattern) in random distribution; may be normal early |
| HRCT | More sensitive than CXR; detects miliary pattern earlier |
| Sputum smear | AFB smear often negative in miliary TB (low yield) |
| BAL/bronchoscopy | Culture positive in ~50% |
| Blood cultures | Positive in ~50% of HIV patients |
| Bone marrow biopsy | High yield (~50-60%); granulomas on biopsy |
| Liver biopsy | Granulomas; high diagnostic yield |
| IGRA / TST | May be falsely negative due to anergy in severely immunocompromised |
| CSF | If meningitis suspected |
| Fundoscopy | Choroidal tubercles (pathognomonic) |
| Urine culture | Mycobacterial culture |
The classic radiographic miliary pattern may not appear on CXR until disease has progressed; CT detects it earlier. A miliary pattern is not specific to TB - also seen in histoplasmosis, malignancy (e.g., miliary carcinomatosis), sarcoidosis, and siderosis.
Treatment
Same as other active TB - RIPE regimen:
- Intensive phase (2 months): Rifampicin + Isoniazid + Pyrazinamide + Ethambutol (RIPE)
- Continuation phase (4-7 months): Rifampicin + Isoniazid (extending to 9-12 months total for CNS/bone disease)
- Adjunctive corticosteroids: indicated for TB meningitis and TB pericarditis; may be used in severe miliary disease with ARDS or adrenal insufficiency
3. Pyrexia of Unknown Origin (PUO / FUO)
Definition
Classical FUO (Petersdorf and Beeson, 1961 - updated):
- Fever >101°F (38.3°C) on several occasions
- Duration >3 weeks
- Diagnostic uncertainty despite appropriate evaluation including:
- At least 3 outpatient visits, OR
- At least 3 days in hospital
The key principle: atypical presentations of common diseases (e.g., TB, lymphoma, SLE) are far more likely than classic presentations of rare diseases.
Classification (Durack and Street, 1991 categories)
| Type | Definition |
|---|---|
| Classic FUO | As above |
| Nosocomial FUO | Fever in hospitalized patient not present on admission; >3 days' evaluation; (Clostridium difficile, drug fever, pulmonary embolism, sinusitis from NGT) |
| Immune-deficient FUO | Fever in neutropenic patient; >3 days' evaluation; (opportunistic infections) |
| HIV-associated FUO | Fever >4 weeks outpatient or >3 days inpatient in HIV+ patient; (MAC, CMV, PCP, lymphoma) |
Causes (Goldman-Cecil - by domain)
Infectious (most common overall, ~30-40%)
Common:
- Occult abscess (abdominal, pelvic, dental)
- Cytomegalovirus (CMV)
- Culture-negative endocarditis
- Epstein-Barr virus (EBV/infectious mononucleosis)
- M. tuberculosis (especially extrapulmonary)
- Osteomyelitis
Less common:
- Bartonella spp., Brucella spp.
- Hepatitis A, B, or E
- Acute HIV
- Salmonella spp., Toxoplasma
Malignant (~20-30%)
- Lymphoma (Hodgkin's and non-Hodgkin's) - most common malignant cause
- Leukemia
- Renal cell carcinoma ("internist's tumor")
- Hepatocellular carcinoma
- Atrial myxoma
- Castleman disease
- Myelodysplastic syndrome
Inflammatory / Rheumatologic (~20-30%)
- Adult-onset Still disease (classic triad: quotidian fever, evanescent salmon-pink rash, arthritis)
- Temporal (giant cell) arteritis - especially in elderly; ESR markedly elevated
- Polymyalgia rheumatica
- Systemic lupus erythematosus (SLE)
- Granulomatosis with polyangiitis (Wegener's)
- Inflammatory bowel disease
- Rheumatoid arthritis
- Sarcoidosis
- Polyarteritis nodosa, Takayasu arteritis
Miscellaneous
- Drug fever (common, often overlooked)
- Factitious fever
- Hyperthyroidism / subacute thyroiditis (de Quervain)
- Pheochromocytoma
- Chronic pulmonary embolism
- Hemophagocytic lymphohistiocytosis (HLH)
- Periodic fever syndromes (e.g., FMF, PFAPA)
- Hematoma
- Adrenal insufficiency (hypoadrenalism)
Undiagnosed (~10-15%)
Many resolve spontaneously; a favorable sign (usually not malignant).
Diagnostic Approach (Goldman-Cecil)
Initial evaluation (history, physical, basic tests):
| Test | Rationale |
|---|---|
| CBC with differential | Anemia (malignancy, chronic disease), atypical lymphocytes (EBV), eosinophilia (parasites) |
| CMP (metabolic panel) | Liver function, renal function |
| Urinalysis + sediment | UTI, renal cell carcinoma, vasculitis |
| ESR + CRP | Elevation: infection, inflammatory, malignancy |
| Blood cultures x3 | Spaced ≥12 h apart, at least 2 drawn over ≥74 hours |
| HIV Ag/Ab (4th generation) | |
| CMV IgM/IgG | |
| EBV heterophile antibody | |
| TB-IGRA (or TST) | |
| ANA, RF | SLE, rheumatoid arthritis |
| TSH | Thyroid disease |
| LDH, uric acid | Lymphoma, hemolysis |
| CXR, abdominal ultrasound | Abscess, malignancy, organomegaly |
If initial evaluation unrevealing:
- FDG-PET/CT scan: identifies a cause in 30-60% of cases; can detect large-vessel vasculitis, metabolically active tumor, occult infection, or guide biopsy site
- Echocardiography: endocarditis, atrial myxoma
- CT chest/abdomen/pelvis: lymphoma, abscess, malignancy
- Tissue biopsy (lymph node, liver, bone marrow, temporal artery): guided by imaging or clinical clues
Management:
- Treat reversible causes; avoid empiric antibiotics/steroids unless patient is critically ill (they mask the diagnosis)
- If no diagnosis after full workup: watchful waiting or shared-decision trial of NSAIDs/corticosteroids for presumed inflammatory etiology
- Periodically reassess (new symptoms, new findings)
4. Irregular Pulse
An irregular pulse indicates that cardiac beats do not occur at regular intervals. It is classified as:
Types of Irregular Pulse
A. Irregularly Irregular
Every beat occurs at a completely unpredictable interval - no repeating pattern.
| Cause | Key Features |
|---|---|
| Atrial fibrillation (most common) | Classic "irregularly irregular" pulse; absent a wave on JVP; pulse deficit present; no P waves on ECG |
| Multifocal atrial tachycardia (MAT) | Rate 100-180 bpm; ≥3 distinct P-wave morphologies; common in COPD, critically ill |
| Atrial flutter with variable block | Sawtooth flutter waves at 300 bpm with varying AV conduction ratios |
| Multiple extrasystoles (PVCs/PACs) | Irregular but with a pattern of premature beats followed by compensatory pauses |
| Wandering atrial pacemaker | Slow, irregular; P-wave morphology changes |
Clinical clue: In AF, the peripheral pulse rate is less than the apical rate (pulse deficit) because short R-R intervals don't allow sufficient LV filling to produce a palpable radial pulse.
B. Regularly Irregular
Irregularity follows a predictable pattern.
| Cause | Key Features |
|---|---|
| 2nd-degree AV block (Mobitz I / Wenckebach) | Group beating; PR progressively lengthens, then dropped beat |
| Bigeminy (alternating normal beat + ectopic) | Every second beat is early (PVC or PAC); "pulse every other beat" sensation |
| Trigeminy | Every third beat is ectopic |
| Sinus arrhythmia | Heart rate increases with inspiration, decreases with expiration; normal in young people |
Examination Tips
- Feel the radial pulse for rhythm and rate
- Confirm with apical auscultation - count apical rate vs. radial rate (pulse deficit = AF)
- JVP inspection: absent a waves = AF; cannon a waves = complete heart block or VT
- Always confirm with ECG - history and exam narrow the differential, but rhythm diagnosis requires ECG
Key Clinical Associations
| Finding | Think of |
|---|---|
| Irregular pulse + elderly + hypertension | AF |
| Irregular pulse + palpitations + young female | AVNRT or PACs/PVCs |
| Irregular pulse + severe COPD | MAT |
| Irregular pulse + slow rate + cannon a waves | Complete heart block |
| Irregular pulse post-MI | PVCs (bigeminy/trigeminy), AF, VT |
| Irregularly irregular + rate >200 bpm + wide QRS | Pre-excited AF (WPW) - emergency |
5. Myxedema Coma
Definition
Myxedema coma is the most severe, life-threatening manifestation of hypothyroidism, representing decompensated hypothyroidism with:
- Altered mental status (ranging from confusion/obtundation to frank coma)
- Hypothermia (a hallmark; temperature often 32-35°C)
- A precipitating event (almost always present)
Despite the name, actual coma is uncommon; most patients are severely obtunded. Mortality is up to 30% with optimal treatment and approaches 100% without treatment.
Precipitating Factors (Rosen's Box 117.6)
| Category | Examples |
|---|---|
| Infections | Pneumonia (most common), sepsis, UTI |
| Environmental | Cold exposure |
| Cardiovascular | Myocardial infarction, CHF, stroke |
| Drugs - CNS depression | Sedatives, narcotics, anesthetics, neuroleptics |
| Drugs - reduce thyroid hormone | Amiodarone, lithium, iodides |
| Drugs - enhance elimination | Phenytoin, rifampin |
| Non-compliance/absorption issues | Iron, calcium, cholestyramine (bind levothyroxine) |
| Metabolic | Hyponatremia, hypoglycemia, hypercapnia, hypoxia, hypercalcemia, DKA |
| Trauma/Burns | Any physiologic stress |
| GI bleeding | - |
Clinical Features
Hypothyroidism features + decompensation:
Vital signs:
- Hypothermia (core temperature often <35°C; severe hypothermia <30°C)
- Bradycardia
- Hypotension
- Hypoventilation (respiratory failure is a major cause of death)
Neurological:
- Confusion, obtundation, stupor, coma
- Seizures
- Delayed relaxation of deep tendon reflexes ("hung-up" reflexes)
- Cerebellar ataxia
Cardiovascular:
- Sinus bradycardia
- Long QT interval → ventricular arrhythmias
- Cardiomegaly, pericardial effusion
- Diastolic heart failure
Respiratory:
- Hypoventilation → hypercapnia → respiratory acidosis
- Pleural effusions
- Obstructive sleep apnea history
Metabolic:
- Hyponatremia (dilutional; impaired free water excretion) - associated with increased mortality; correct carefully to avoid osmotic demyelination
- Hypoglycemia (esp. in children)
- Elevated CPK
- Anemia
Classic Appearance:
- Dry, coarse, cool, pale-yellow skin
- Periorbital and facial puffiness (non-pitting myxedema)
- Macroglossia
- Lateral eyebrow thinning (Queen Anne's sign)
- Husky, deep voice
- Goiter (if Hashimoto's) or absent thyroid (post-thyroidectomy/RAI)
Investigations
- TSH: markedly elevated (primary hypothyroidism); may be low/normal in central hypothyroidism
- Free T4: very low
- Free T3: low
- Cortisol: measure before steroids; adrenal insufficiency may coexist
- ABG: hypoxia, hypercapnia, respiratory acidosis
- Electrolytes: hyponatremia
- Glucose: hypoglycemia
- ECG: bradycardia, long QT, low-voltage complexes, T-wave changes
- CXR: cardiomegaly, pleural/pericardial effusion
- CBC: normocytic anemia
Treatment (ICU Setting)
1. Thyroid Hormone Replacement (cornerstone)
IV levothyroxine (T4):
- Loading dose: 200-400 µg IV (lower end for elderly, small body habitus, known CAD, or arrhythmias)
- Maintenance: 1.6 µg/kg/day IV (reduce to 75% of IV dose when switching to oral)
T3 (liothyronine) - optional addition:
- Considered in severely ill patients for faster effect (T4→T3 conversion is impaired in critical illness)
- Use with extreme caution - elevated serum T3 is associated with increased mortality; lower doses (5-10 µg IV q8h)
2. Glucocorticoids (stress dose)
- Hydrocortisone 100 mg IV q8h (covers possible concurrent adrenal insufficiency - up to 10% of myxedema coma cases)
- Taper as the patient recovers; can discontinue once adrenal function is confirmed normal
3. Supportive Care
| Issue | Management |
|---|---|
| Respiratory failure | Mechanical ventilation (often required); avoid sedatives/narcotics (prolonged effects due to slowed metabolism) |
| Hypothermia | Passive rewarming (blankets); active rewarming rarely needed (thyroid hormone replacement will correct it) |
| Hypotension | IV crystalloids; vasopressors if refractory; thyroid hormone replacement alone often improves BP |
| Hyponatremia | Fluid restrict; hypertonic saline only for severe symptoms (seizures, coma) - then correct slowly to avoid osmotic demyelination |
| Hypoglycemia | IV glucose |
| Infection | Broad-spectrum antibiotics empirically (pneumonia is most common precipitant) |
| Drug metabolism | Reduce doses of all sedatives, opioids, anesthetics - metabolism is markedly slowed |
Disposition
- All myxedema coma patients: ICU admission
- Regular hypothyroidism: outpatient management
Sources: Harrison's Principles of Internal Medicine 22E (9781265977061); Goldman-Cecil Medicine (9780323930345); Rosen's Emergency Medicine (9780323757898); Tintinalli's Emergency Medicine (9781260019933); Robbins & Cotran Pathologic Basis of Disease (9780443264528); Braunwald's Heart Disease (9780323722193)
Polycyclic kidney disease, IBS, ulcerative colitis, pneumothorax
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content for all four topics. Let me compile the complete answer:
1. Polycystic Kidney Disease (PKD)
PKD encompasses a group of genetic disorders characterized by bilateral renal cysts that progressively replace normal parenchyma, leading to chronic kidney disease (CKD) and often end-stage renal disease (ESRD).
A. Autosomal Dominant PKD (ADPKD)
Genetics
| Feature | Details |
|---|---|
| Inheritance | Autosomal dominant |
| Prevalence | ~1:400-1:1000; most common inherited cause of ESRD requiring dialysis/transplant |
| PKD1 gene | Chromosome 16p13.3; encodes polycystin-1; accounts for ~85% of cases; more severe phenotype |
| PKD2 gene | Chromosome 4q21-23; encodes polycystin-2 (a calcium channel); accounts for ~15%; slower progression |
| Penetrance | Variable; ~50% of affected individuals eventually develop ESRD |
| "Two-hit" hypothesis | Germline mutation in one allele + somatic mutation in the second allele triggers cyst formation in individual tubular cells |
Polycystin proteins are located on primary cilia of renal tubular epithelial cells. Loss of function disrupts calcium signaling, leading to increased cAMP, cell proliferation, and fluid secretion into cysts.
Risk Factors for ESRD Progression
- Early age of presentation
- Male sex
- PKD1 mutation (worse than PKD2)
- Hypertension (present in >75% by age 20-30)
- African ethnicity
- Larger total kidney volume (TKV) - measured by MRI/CT
Clinical Features
Renal:
- Abdominal/flank pain (distension, cyst hemorrhage, infection, nephrolithiasis)
- Hematuria (gross or microscopic; cyst rupture)
- Palpable bilateral flank/abdominal masses
- Hypertension (early, due to intrarenal RAAS activation - often before any decline in GFR)
- Recurrent UTIs and cyst infections
- Progressive decline in GFR → ESRD (median age ~58 years for PKD1, ~79 years for PKD2)
- Nephrolithiasis (uric acid and calcium oxalate stones, in ~20%)
Extrarenal manifestations:
| Organ | Manifestation |
|---|---|
| Liver | Hepatic cysts (most common extrarenal; ~80%; rarely cause liver failure) |
| Intracranial | Berry (saccular) aneurysms in 10-30% → subarachnoid hemorrhage; risk is higher with family history |
| Cardiovascular | Mitral valve prolapse (~25%); aortic root dilation |
| Pancreas | Pancreatic cysts (~10%) |
| Seminal vesicles | Cysts |
| Arachnoid membranes | Cysts |
| Colon | Diverticulosis (increased risk) |
Key exam pearl: Intracranial aneurysms (10-30%) can cause sudden death from SAH in young adults with ADPKD. Screen patients with family history of SAH or aneurysm with MR angiography.
Diagnosis
- Ultrasound: most practical; age-specific criteria - in PKD1 family: ≥3 cysts (one kidney) in patients 15-39 years; ≥2 per kidney age 40-59; ≥4 per kidney ≥60
- CT/MRI: more sensitive; MRI used for TKV measurement (prognostic tool)
- Genetic testing: useful if atypical presentation or for living donor screening of family members before cysts develop
Treatment
Blood pressure control:
- Target: 110/75 mmHg in young patients (HALT-PKD trial showed rigorous BP control with ACEi slowed TKV growth and preserved GFR)
- ACE inhibitors or ARBs (first-line; RAAS blockade)
Tolvaptan (vasopressin V2-receptor antagonist):
- FDA-approved for patients ≥18 years at risk of rapidly progressing ADPKD
- Reduces cAMP in collecting duct cells → inhibits cyst epithelial cell proliferation and fluid secretion
- TEMPO 3:4 trial: slowed TKV growth and rate of GFR decline
- Side effects: polyuria, polydipsia, nocturia; hepatotoxicity (monitor LFTs)
- Not for all patients - reserve for those with evidence of rapid progression (TKV >750 mL, age-adjusted mayo imaging class 1C/1D/1E)
Other approaches:
- Somatostatin analogues (octreotide-LAR): reduce cAMP; slowed renal function decline (ALADIN trial)
- mTOR inhibitors (sirolimus, everolimus): trialed but significant side effects; not standard care
- Pain management: simple analgesics; nerve block for refractory chronic pain (DIPAK trial)
- Cyst infection: fluoroquinolones (penetrate cysts); occasionally drainage
Renal replacement:
- Peritoneal dialysis and hemodialysis both used; PD may be challenging in very large kidneys
- Renal transplantation is preferred ESRD treatment
B. Autosomal Recessive PKD (ARPKD)
| Feature | Details |
|---|---|
| Inheritance | Autosomal recessive |
| Prevalence | ~1:20,000 live births; carrier frequency ~1:70 |
| Gene | PKHD1 on chromosome 6p21.1-6p12.2; encodes fibrocystin/polyductin (FPC) |
| FPC | Large transmembrane protein on primary cilia of collecting ducts and bile ducts |
| Presentation | Neonates/infants; severe cases present with oligohydramnios, Potter sequence (pulmonary hypoplasia, limb deformities) |
| Renal | Fusiform dilation of collecting ducts; bilateral enlarged echogenic kidneys |
| Hepatic | Congenital hepatic fibrosis → portal hypertension; biliary dysgenesis (Caroli disease) |
| Prognosis | 30-50% die in neonatal period; survivors develop CKD; many progress to ESRD in childhood/early adulthood |
2. Irritable Bowel Syndrome (IBS)
Definition (Rome IV Criteria)
Recurrent abdominal pain, on average ≥1 day/week in the last 3 months (with onset ≥6 months ago), associated with ≥2 of:
- Related to defecation
- Associated with a change in stool frequency
- Associated with a change in stool form (appearance)
IBS is a disorder of gut-brain interaction (not a structural or inflammatory disease). No organic cause is identified on investigation.
Subtypes (by predominant stool pattern)
| Subtype | Abbreviation | Prevalence |
|---|---|---|
| Predominant diarrhea | IBS-D | 35-40% |
| Mixed bowel habits | IBS-M | 35-40% |
| Predominant constipation | IBS-C | ~25% |
| Unclassified | IBS-U | <5% |
Subtypes can transition over time in the same patient.
Epidemiology
- Global prevalence: 4.1% (Rome IV); higher with older criteria
- More common in women (5.2% vs 2.9% in men)
- Incidence: ~38 per 10,000 person-years
- Up to 50% of affected individuals never seek healthcare
- Generates ~4.4 million physician visits annually in the US alone
Pathophysiology
IBS results from dysregulation of gut-brain interactions, involving:
- Visceral hypersensitivity - abnormally increased pain perception in response to normal gut distension (lowered visceral pain threshold); strongest pathophysiologic mechanism
- Altered gut motility - slower transit in IBS-C, faster in IBS-D; no consistent specific pattern
- Gut microbiota dysbiosis - altered composition; post-infectious IBS develops in ~10% after gastroenteritis
- Mucosal immune activation - increased mast cells, inflammatory mediators, increased intestinal permeability
- Enteroendocrine dysfunction - abnormal serotonin (5-HT) signaling; serotonin plays a key role in gut motility and visceral sensation
- Autonomic nervous system dysregulation
- CNS modulation - altered central processing of visceral input; comorbid anxiety/depression in >50%
Risk factors:
- Genetic predisposition (familial clustering, 1.75-2.75x odds)
- Adverse childhood experiences
- Post-infectious gastroenteritis (bacterial, viral, or parasitic)
- Food (FODMAPs, fat, caffeine)
- Psychological stress
Clinical Features
- Abdominal pain/discomfort: crampy, variable location; relieved (partially) by defecation
- Altered bowel habits: diarrhea, constipation, or both; urgency; incomplete evacuation; mucus in stool
- Bloating/distension: very common, especially post-meal
- Absence of alarm features: no weight loss, no blood in stool, no nocturnal symptoms, no fever
Associated features (non-GI):
- Fibromyalgia, chronic fatigue syndrome
- Dyspareunia, urinary urgency
- Anxiety, depression (>50% comorbidity)
- Headache
Diagnosis
IBS is a positive clinical diagnosis based on Rome IV criteria - not a diagnosis of exclusion in all cases.
"Red flag" features requiring investigation:
- Age >50 at onset (or family history of colorectal cancer → colonoscopy)
- Unexplained weight loss
- Blood in stool / iron-deficiency anemia
- Fever
- Nocturnal symptoms waking from sleep
- Recent antibiotic use (Clostridioides difficile)
- Inflammatory markers elevated (ESR, CRP, fecal calprotectin)
Minimum investigations in typical presentation:
- CBC (anemia)
- CRP, fecal calprotectin (rule out IBD)
- TSH (thyroid disease)
- Celiac serology (anti-tTG IgA) - important as celiac disease mimics IBS-D
- Consider stool culture/O&P if infectious etiology suspected
Treatment
Lifestyle and Dietary
- Low-FODMAP diet (Fermentable Oligosaccharides, Disaccharides, Monosaccharides And Polyols): strongest evidence; reduces symptoms in ~50-70% of IBS patients; guided by dietitian
- Regular exercise; adequate sleep
- Identify and avoid trigger foods
Pharmacological (symptom-directed)
IBS-C:
| Drug | Mechanism | Notes |
|---|---|---|
| Lubiprostone | Chloride channel activator | Increases intestinal fluid secretion |
| Linaclotide | Guanylate cyclase-C agonist | Reduces visceral pain + increases secretion |
| Plecanatide | Guanylate cyclase-C agonist | Similar to linaclotide |
| Tegaserod | 5-HT4 partial agonist | Prokinetic; restricted use (cardiovascular risk) |
| Psyllium / soluble fiber | Bulking | Modest benefit |
| PEG laxatives | Osmotic | For constipation symptoms (not pain) |
IBS-D:
| Drug | Mechanism | Notes |
|---|---|---|
| Loperamide | μ-opioid agonist | Reduces diarrhea; not pain |
| Alosetron | 5-HT3 antagonist | Women with severe IBS-D; REMS program (ischemic colitis risk) |
| Eluxadoline | Mixed opioid agonist/antagonist | IBS-D; contraindicated without gallbladder |
| Rifaximin | Non-absorbable antibiotic | 2-week course for IBS-D; targets gut microbiota |
| Cholestyramine | Bile acid sequestrant | Useful in bile acid malabsorption |
For pain (all subtypes):
- Antispasmodics: dicyclomine, hyoscine (anticholinergics); mebeverine; peppermint oil
- Low-dose TCAs (amitriptyline, desipramine): for pain; especially IBS-D (slow transit)
- SSRIs: for pain + comorbid depression; better for IBS-C (faster transit)
- Gabapentin/pregabalin: visceral hypersensitivity
Psychological:
- Cognitive behavioral therapy (CBT): strong evidence
- Gut-directed hypnotherapy
- Mindfulness-based therapy
3. Ulcerative Colitis (UC)
Definition and Pathology
UC is a chronic, relapsing inflammatory bowel disease affecting the mucosa and submucosa of the colon, characteristically starting in the rectum and extending proximally in a continuous pattern. It affects only the colon (not the small bowel).
Gross and Histologic Features
| Stage | Gross | Histology |
|---|---|---|
| Mild | Granular, hyperemic, edematous mucosa | Epithelial necrosis, acute inflammatory infiltrate in lamina propria, cryptitis, crypt abscesses |
| Severe | Ulceration, friability, bleeds on touch | Lymphocytic infiltrate, crypt architectural distortion |
| Chronic | Pseudopolyps (epithelial regeneration), loss of fold pattern, shortened/narrowed colon | Crypt distortion, mucosal atrophy |
Endoscopic appearance: starts at rectum, continuous involvement, no skip lesions; loss of vascular pattern → granularity → friability → ulcers → pseudopolyps
Comparison: UC vs Crohn's Disease
| Feature | Ulcerative Colitis | Crohn Disease |
|---|---|---|
| Location | Colon only (rectum → proximal) | Mouth to anus (terminal ileum in 70%) |
| Pattern | Continuous | Skip lesions |
| Depth | Mucosal/submucosal | Transmural |
| Ulceration | Continuous | Discrete, aphthous → cobblestoning |
| Fistulas | No | Yes |
| Strictures | No (late complication) | Yes |
| Perianal disease | No | Yes (30%) |
| Granulomas | No | Yes (noncaseating, ~30% on biopsy) |
| ASCA | <15% | 40-70% |
| pANCA | 55% | 20% |
Clinical Features
- Bloody diarrhea (hallmark - mucus and blood)
- Rectal urgency, tenesmus
- Abdominal cramping (before defecation)
- Constitutional symptoms in severe disease: fever, weight loss, anemia, hypoalbuminemia
Disease extent classification:
- Proctitis: rectum only (~30%)
- Left-sided colitis: rectum to splenic flexure (~30%)
- Extensive/pancolitis: beyond splenic flexure (~40%)
Severity Classification (Truelove & Witts)
| Severity | Stools/day | Bleeding | Temp | HR | Hb | ESR |
|---|---|---|---|---|---|---|
| Mild | <4 | Small | Normal | Normal | >11 g/dL | <20 mm/hr |
| Moderate | 4-6 | Moderate | <37.8°C | <90 | 10.5-11 | 20-30 |
| Severe | >6 | Severe | >37.8°C | >90 | <10.5 | >30 |
Severe UC = medical emergency (risk of toxic megacolon, perforation)
Extraintestinal Manifestations
| System | Manifestation |
|---|---|
| Joints | Peripheral arthritis (parallels bowel activity); ankylosing spondylitis / sacroiliitis (independent of bowel activity) |
| Skin | Erythema nodosum (parallels bowel activity); pyoderma gangrenosum |
| Eyes | Uveitis/iritis; episcleritis |
| Liver | Primary sclerosing cholangitis (PSC) - in 5% of UC; independent of bowel activity; increases colorectal cancer risk |
| Hematologic | Anemia (blood loss, chronic disease, B12/folate deficiency); thromboembolic disease (hypercoagulable state) |
Cancer Risk
- Colorectal cancer (CRC) risk increases with: extent of disease, duration (significant after 8-10 years), severity, concomitant PSC
- Surveillance colonoscopy recommended starting 8-10 years after diagnosis; every 1-3 years
Medical Treatment
Step 1 - Mild to Moderate UC
5-Aminosalicylates (5-ASA) - topical anti-inflammatory (first-line):
- Mesalamine (oral + rectal enema/suppository) - mainstay; induction and maintenance of remission
- Sulfasalazine (5-ASA + sulfapyridine carrier) - less preferred due to side effects
- Olsalazine, balsalazide - prodrugs released by bacterial cleavage in colon
- Rectal preparations (suppositories, enemas) for proctitis/left-sided disease
Step 2 - Moderate to Severe UC
Corticosteroids (to induce remission; not for maintenance):
- Oral prednisone 40-60 mg/day, tapered over 8-12 weeks
- IV methylprednisolone 40-60 mg/day for severe disease
- Budesonide MMX (colonic release) for mild-moderate UC; lower systemic bioavailability
Step 3 - Immunomodulators
- Azathioprine / 6-mercaptopurine (6-MP): steroid-sparing maintenance therapy; slow onset (3-6 months); risk of lymphoma, pancreatitis, myelosuppression
- Methotrexate: mainly Crohn's; less used in UC
- Ozanimod (S1P receptor modulator): new oral agent for moderately-severely active UC
Step 4 - Biologics (moderate-severe, or steroid-refractory)
| Drug | Target | Notes |
|---|---|---|
| Infliximab | Anti-TNFα | IV infusion; rescue therapy in acute severe UC |
| Adalimumab | Anti-TNFα | SC injection |
| Golimumab | Anti-TNFα | SC injection; UC-specific |
| Vedolizumab | Anti-α4β7 integrin | Gut-selective; preferred in patients with TB/hepatitis risk |
| Ustekinumab | Anti-IL-12/23 | SC/IV |
| Tofacitinib | JAK inhibitor | Oral; rapid onset; thrombosis/cardiovascular risk |
| Filgotinib, Upadacitinib | JAK inhibitors | Newer oral agents |
Surgical Treatment
- Indications: medically refractory disease, fulminant/toxic megacolon, hemorrhage, perforation, high-grade dysplasia, or colorectal cancer
- Total proctocolectomy with ileal pouch-anal anastomosis (IPAA / J-pouch) - procedure of choice; curative
- Complications: pouchitis (up to 50%), pelvic sepsis, infertility (females)
4. Pneumothorax
Definition
Pneumothorax is the accumulation of air in the pleural space (between visceral and parietal pleura), causing partial or complete lung collapse.
Classification
By Cause
| Type | Definition | Common Causes |
|---|---|---|
| Primary spontaneous (PSP) | No underlying lung disease | Rupture of subpleural blebs (tall, thin young males; Marfan syndrome); smoking |
| Secondary spontaneous (SSP) | Underlying lung disease | COPD (most common), asthma, cystic fibrosis, TB, PCP (in HIV), lung cancer, pulmonary fibrosis, LAM |
| Traumatic | Direct/indirect chest trauma | Rib fractures, penetrating injury |
| Iatrogenic | Medical procedure | Central line placement, thoracentesis, transbronchial/pleural biopsy, CT-guided lung biopsy, positive pressure ventilation |
| Tension pneumothorax | One-way valve mechanism | Air accumulates under pressure → compresses mediastinum; life-threatening emergency |
By Size
- Small: <20% of hemithorax or <3 cm from lung apex to chest wall
- Large: >20% or >3 cm
Pathophysiology
In spontaneous pneumothorax: alveolar or bleb rupture allows air to enter the pleural space. Normally the pleural space is maintained at negative pressure; air entry eliminates this negative pressure and the lung collapses due to its elastic recoil.
Tension pneumothorax: a ball-valve mechanism allows air to enter but not exit the pleural space with each breath. Progressive pressure:
- Compresses ipsilateral lung (complete collapse)
- Shifts mediastinum contralaterally (tracheal deviation away from affected side)
- Compresses vena cava → reduces venous return → obstructive shock
- Compresses heart
Clinical Features
Simple/Spontaneous
- Sudden onset pleuritic chest pain (sharp, worse with breathing)
- Dyspnea (severity proportional to size and underlying lung reserve)
- Dry cough
- Most occur at rest (not with exertion)
Physical examination:
| Sign | Finding |
|---|---|
| Inspection | Reduced chest wall movement on affected side |
| Palpation | Reduced tactile fremitus; trachea central or slightly deviated |
| Percussion | Hyperresonance on affected side |
| Auscultation | Reduced/absent breath sounds on affected side |
Tension Pneumothorax (Emergency)
- Tachycardia
- Hypotension (obstructive shock)
- JVD (elevated JVP due to impaired venous return)
- Tracheal deviation away from affected side
- Absent breath sounds + hyperresonance on affected side
- Progressive respiratory failure and cardiac arrest if untreated
- Elevated peak airway pressure (if mechanically ventilated)
In tension pneumothorax: Do NOT wait for imaging - treat immediately based on clinical findings.
Investigations
- CXR (PA/erect): absent lung markings peripheral to the visceral pleural line; collapsed lung; mediastinal shift in tension
- Ultrasound (POCUS): absence of "lung sliding" sign at point of care - fast and sensitive
- CT chest: most sensitive; identifies blebs, underlying lung disease, exact size
Treatment
Management algorithm (Mulholland's Surgery):
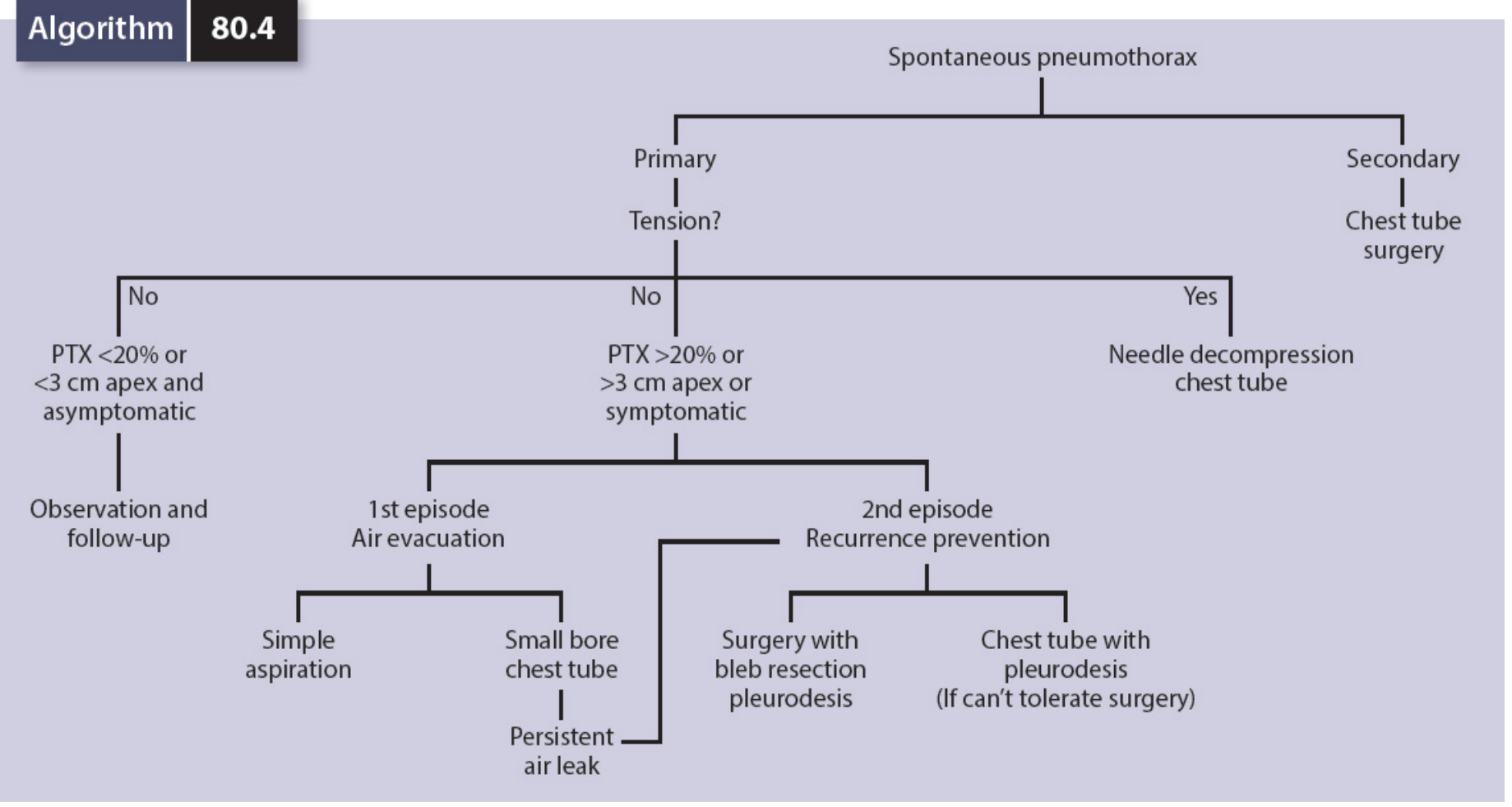
Tension Pneumothorax - IMMEDIATE
- Needle decompression: 14-16G needle, 2nd intercostal space, midclavicular line → converts to simple pneumothorax
- Follow with chest tube (tube thoracostomy)
Primary Spontaneous Pneumothorax
- Small (<20% or <3 cm) + asymptomatic + no underlying lung disease: Observation; supplemental O₂ (accelerates reabsorption by ~4x); repeat CXR in 4-6 hours
- Large (>20% or >3 cm) or symptomatic:
- 1st episode: needle aspiration (85% success rate) OR small-bore chest tube (24Fr or pigtail catheter via Seldinger technique) connected to water-seal drainage ± suction (-20 cm H₂O)
- Chest tube removed when lung re-expanded and air leak has stopped (4-hour clamp test before removal)
Secondary Spontaneous Pneumothorax
- Observation has NO role - even small SSP requires intervention (poor reserve, high risk of tension)
- Chest tube + consider early surgical/thoracoscopic intervention even on first episode
- VATS (video-assisted thoracoscopic surgery) with bleb resection + pleurodesis
Recurrence Prevention (2nd episode or persistent air leak)
- Chemical pleurodesis: talc instilled via chest tube
- Surgical pleurodesis: VATS with mechanical pleurodesis + bleb/bullae resection (preferred when patient can tolerate surgery)
- Recurrence rate: ~30% within 2 years without pleurodesis; VATS reduces recurrence to <5%
Iatrogenic Pneumothorax
- Manage same as spontaneous
- Small + asymptomatic + not on PPV: observation acceptable
- On any form of positive pressure ventilation: drain immediately (risk of tension)
Practical Notes
- Persistent air leak initially: suction at -20 cm H₂O to promote visceral-parietal pleural apposition
- Switch to water seal only after air leak resolves, then confirm with CXR before tube removal
- Loculated pneumothoraces: drain under US or CT guidance
Sources: Bailey & Love's Surgery 28th Ed. (9780367548117); Harrison's Internal Medicine 22E (9781265977061); Goldman-Cecil Medicine (9780323930345); Mulholland & Greenfield's Surgery 7E (9781975143169); Sleisenger & Fordtran's GI Disease (9780323609623); Roberts & Hedges' Clinical Procedures in Emergency Medicine (9780323354783)
ARDS
Finding Sources
Searching PubMed
"acute respiratory distress syndrome"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
I now have everything needed. Here is the comprehensive answer:
Acute Respiratory Distress Syndrome (ARDS)
ARDS is a life-threatening syndrome of acute, diffuse, inflammatory lung injury resulting in non-cardiogenic pulmonary edema, severe hypoxemia, decreased lung compliance, and a mortality rate that commonly exceeds 30%.
Definition - The Berlin Definition (2012)
The Berlin definition replaced the older American-European Consensus Conference (AECC) criteria and classifies ARDS by severity:
| Criterion | Requirement |
|---|---|
| Timing | Onset within 7 days of a known clinical insult or new/worsening respiratory symptoms |
| Chest imaging | Bilateral opacities on CXR or CT not fully explained by effusions, lobar/lung collapse, or nodules |
| Origin of edema | Respiratory failure not fully explained by cardiac failure or fluid overload (if no risk factor present, objective assessment needed - e.g., echo) |
| Oxygenation (on ≥5 cm H₂O PEEP) | See severity classification below |
Severity Classification
| Severity | PaO₂/FiO₂ ratio | PEEP |
|---|---|---|
| Mild | 201-300 mmHg | ≥5 cm H₂O |
| Moderate | 101-200 mmHg | ≥5 cm H₂O |
| Severe | ≤100 mmHg | ≥5 cm H₂O |
The PaO₂/FiO₂ (P/F ratio) is the key diagnostic and severity marker. Normal P/F ratio ≈ 400-500 mmHg. ARDS was formerly called acute lung injury (ALI) when P/F was 200-300; the Berlin definition eliminates this term.
Causes and Risk Factors
ARDS can result from direct (pulmonary) or indirect (extrapulmonary) lung insults:
Direct (Pulmonary)
| Cause | Notes |
|---|---|
| Pneumonia (bacterial, viral, fungal) | Most common direct cause; COVID-19 a prominent recent cause |
| Aspiration of gastric contents | Chemical pneumonitis + superinfection |
| Pulmonary contusion | Trauma |
| Near-drowning | |
| Inhalation injury | Smoke, toxic gases |
| Pulmonary vasculitis |
Indirect (Extrapulmonary)
| Cause | Notes |
|---|---|
| Sepsis | Most common overall cause of ARDS; non-pulmonary sepsis triggers ARDS via systemic cytokine storm |
| Major trauma / hemorrhagic shock | |
| Severe pancreatitis | ARDS develops in 15-20% of cases; accounts for up to 60% of deaths; phospholipase A2 degrades surfactant |
| Massive blood transfusion / TRALI | Transfusion-related acute lung injury |
| Burns | |
| Drug overdose | Opioids, salicylates, tricyclics |
| Cardiopulmonary bypass | |
| DIC |
Pathophysiology
Phases of ARDS (Diffuse Alveolar Damage - DAD)
Timeline of ARDS phases:

Phase 1: Exudative (Days 0-7) - the "wet lung"
Key events:
- Injury to alveolar-capillary membrane: damage to type I pneumocytes (alveolar epithelium) and pulmonary microvascular endothelial cells disrupts the normally tight barrier
- Protein-rich edema fluid floods the interstitium and alveolar spaces (non-cardiogenic pulmonary edema)
- Cytokine storm: proinflammatory mediators (IL-1, IL-6, IL-8, TNF-α, leukotriene B₂) recruit and activate neutrophils into alveoli and interstitium
- Hyaline membrane formation: condensed plasma proteins + cellular debris + dysfunctional surfactant aggregate in air spaces
- Surfactant dysfunction: reduced and qualitatively abnormal surfactant → alveolar collapse (atelectasis)
- Microvascular occlusion: microthrombi + fibrocellular proliferation in pulmonary vasculature → increased dead space + pulmonary hypertension
- Result: severe V/Q mismatch, intrapulmonary shunting, refractory hypoxemia, reduced compliance, increased work of breathing
Only ~50% of patients meeting clinical ARDS criteria show histologic DAD on biopsy/autopsy. Patients with confirmed DAD are younger, more severely ill, have lower P/F ratios, and are ~5× more likely to die of hypoxemic respiratory failure.
Phase 2: Proliferative (Days 7-14)
- Hyaline membranes are reorganized
- Type II pneumocyte proliferation to replace damaged type I cells (attempted repair)
- Interstitial inflammation; early fibroproliferation begins (collagen synthesis detectable in BAL as early as 24 hours)
- Decreased neutrophils; reduced pulmonary edema
- Many patients begin to recover; others progress
Phase 3: Fibrotic (Day 14+, weeks)
- Occurs in a subset with persistent ARDS (>2 weeks)
- Pulmonary fibrosis - obliteration of alveolar architecture
- Obliteration of pulmonary capillaries; interstitial and alveolar collagen deposition; bulla formation
- Markedly decreased compliance
- Sustained oxygen dependence; risk of barotrauma
Pathophysiologic Consequences
| Abnormality | Mechanism | Clinical Effect |
|---|---|---|
| Intrapulmonary shunting | Atelectatic alveoli perfused but not ventilated | Refractory hypoxemia (does not respond to O₂ alone) |
| Dead space increase | Microvascular occlusion → ventilated but non-perfused alveoli | Hypercapnia; increased minute ventilation requirement |
| Reduced compliance | Edema, atelectasis, fibrosis | High peak/plateau pressures; increased work of breathing |
| Pulmonary hypertension | Hypoxic vasoconstriction + microvascular obstruction | RV failure (cor pulmonale) in severe cases |
| Ventilator-induced lung injury (VILI) | Overdistension (volutrauma) and cyclic atelectasis (atelectrauma) → biotrauma (cytokine release → systemic organ failure) | Worsens lung injury; causes multi-organ failure |
The "baby lung" concept: in ARDS, the lung is not uniformly diseased. CT reveals:
- Dependent zones: consolidated/fluid-filled or recruitable atelectatic (posterior/inferior)
- Non-dependent zones: relatively normal (anterior/superior) - this is the "baby lung" that receives all the tidal volume if standard Vt used → overdistention
- Intermediate zones: poorly aerated but recruitable
This heterogeneity explains why large tidal volumes cause overdistension and lung injury even when plateau pressures seem acceptable.
Clinical Features and Diagnosis
Symptoms
- Acute onset dyspnea (usually within 12-36 hours of insult; occasionally up to 5-7 days)
- Rapid, shallow breathing; sensation of inability to get enough air
- Tachypnea; increased work of breathing → respiratory fatigue → respiratory failure
Signs
- Tachycardia, tachypnea
- Accessory muscle use, nasal flaring
- Widespread bilateral crackles on auscultation
- Cyanosis (refractory hypoxemia)
- Low SpO₂ despite supplemental O₂
Investigations
- ABG: hypoxemia (low PaO₂/FiO₂ <300), often hypocapnia early (respiratory alkalosis); hypercapnia develops as dead space increases and patient tires
- CXR: bilateral opacities involving ≥75% of lung fields; no cardiomegaly, no pleural effusions (unlike cardiogenic edema) - though difficult to distinguish clinically
- CT chest: bilateral infiltrates; demonstrates extensive heterogeneity; dependent consolidation; non-dependent relatively preserved areas
- Echocardiography: needed if no risk factor identified, to exclude cardiogenic edema; also evaluates RV function
- BAL: neutrophilia (>60% of cells); elevated protein (>0.5 total:serum protein ratio); elevated cytokines - not routinely done but supports diagnosis
Differential Diagnosis of Bilateral Infiltrates + Hypoxemia
- Cardiogenic pulmonary edema (most common mimic) - wedge pressure >18 mmHg
- Diffuse alveolar hemorrhage
- Bilateral pneumonia
- Acute eosinophilic pneumonia
- Cryptogenic organizing pneumonia
- Acute interstitial pneumonia (Hamman-Rich syndrome)
Management
Principle: No specific therapy reverses DAD. Management is supportive - protect the lungs while the underlying insult is treated.
1. Treat the Underlying Cause
- Antibiotics for sepsis/pneumonia
- Source control for sepsis
- Treat pancreatitis, reverse drug overdose, etc.
2. Lung-Protective Mechanical Ventilation (ARDSNet Protocol)
The cornerstone of ARDS management. Based on the landmark ARMA trial (ARDSNet, 2000): low tidal volume (6 mL/kg PBW) reduced mortality by ~22% absolute vs. 12 mL/kg PBW.
ARDSNet Ventilation Strategy:
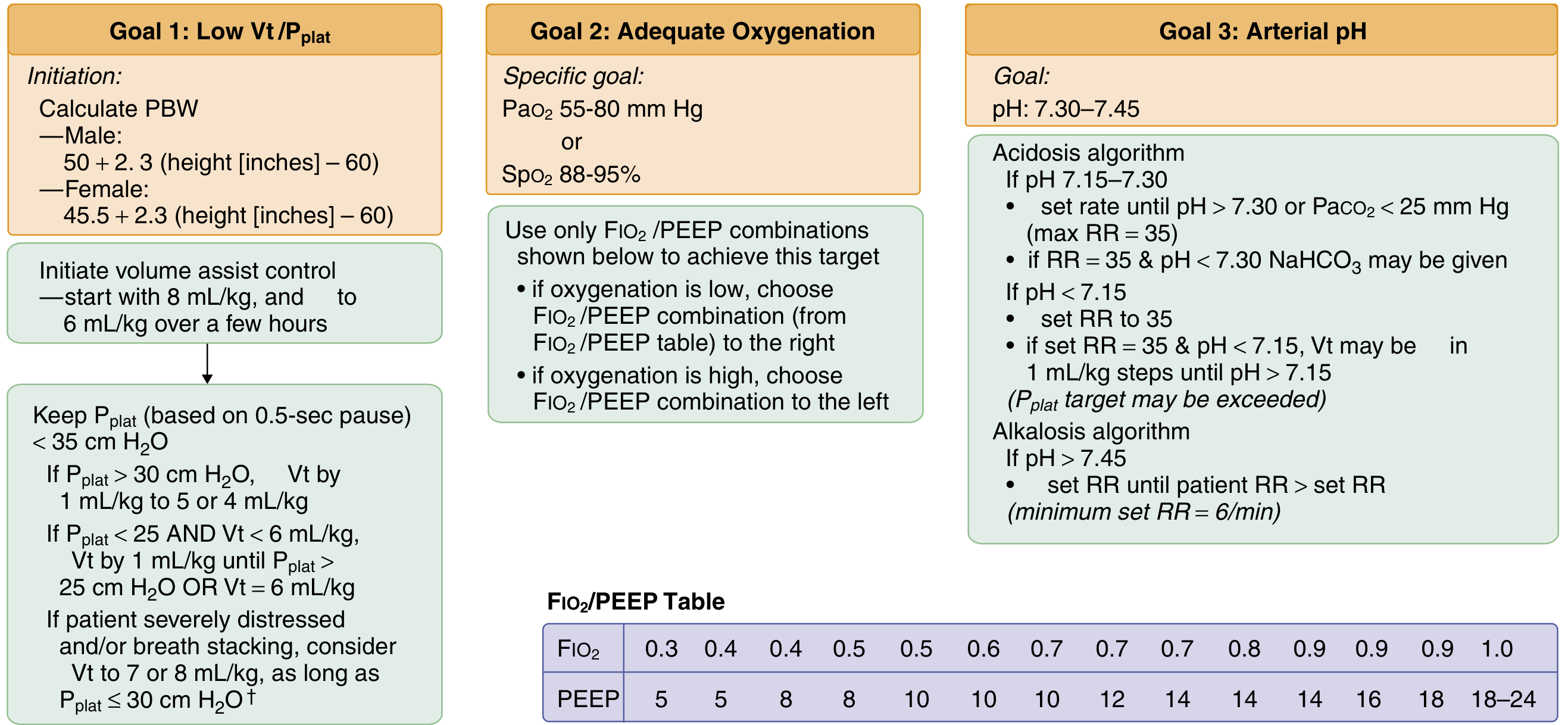
Key parameters:
| Parameter | Target |
|---|---|
| Mode | Volume assist-control (A/C) |
| Tidal volume (Vt) | 6 mL/kg predicted body weight (PBW) (start at 8, decrease over hours) |
| Plateau pressure (Pplat) | ≤30 cm H₂O (measured by 0.5s inspiratory hold) |
| PaO₂ target | 55-80 mmHg |
| SpO₂ target | 88-95% |
| pH target | 7.30-7.45 |
| PEEP | Titrated per FiO₂/PEEP table (see image) |
| Driving pressure | = Pplat - PEEP; target <15 cm H₂O |
Predicted body weight calculation:
- Male: PBW (kg) = 50 + 2.3 × (height [inches] - 60)
- Female: PBW (kg) = 45.5 + 2.3 × (height [inches] - 60)
Permissive hypercapnia: accepting elevated PaCO₂ to avoid volutrauma/barotrauma. If pH 7.15-7.30: increase RR (max 35); if pH <7.15: increase Vt in 1 mL/kg steps until pH >7.15 (Pplat target may be exceeded)
PEEP:
- Required to reduce atelectasis, keep alveoli open, reduce shunting
- Higher PEEP (~12-13 cm H₂O) may benefit moderate-severe ARDS (P/F <200) but not mild ARDS
- Guided by FiO₂/PEEP table (see ARDSNet algorithm) or esophageal pressure monitoring in obese/chest wall stiff patients
- Very high PEEP + aggressive recruitment maneuvers can be harmful (ART trial - increased mortality)
3. Prone Positioning
Evidence: PROSEVA trial (Guérin et al., 2013) - multicenter RCT in severe ARDS:
- Prone positioning for ≥16 hours/day in patients with P/F <150 mmHg
- Reduced 28-day mortality: 32.8% vs. 16% (absolute risk reduction ~17%)
- Mechanism: more uniform distribution of pleural pressure and ventilation; recruits dependent lung; reduces VILI; improves V/Q matching
Current recommendation:
- Indicated for severe ARDS (P/F <150 mmHg) refractory to conventional ventilation
- Should be initiated early (within 12-24h of intubation)
- Used irrespective of its effect on oxygenation in individual patients (mortality benefit is the goal)
- Requires experienced personnel; careful coordination with nursing; risk of accidental extubation, line dislodgement
4. Neuromuscular Blockade (NMB)
- ACURASYS trial (2010): 48h cisatracurium infusion in moderate-severe ARDS improved 90-day mortality
- ROSE trial (2019): routine NMB showed no benefit over light sedation with deep sedation as needed
- Current recommendation: not routinely recommended in all moderate-severe ARDS; judicious use for patient-ventilator asynchrony, breath stacking, or very large patient-driven tidal volumes
- Facilitates lung-protective ventilation when patients strongly override ventilator settings
5. Fluid Management
- Conservative fluid strategy (FACTT trial): compared liberal vs. conservative fluid management
- Conservative strategy: improved oxygenation (higher P/F, more ventilator-free days, more ICU-free days)
- No mortality difference, but the conservative group had shorter duration of mechanical ventilation
- Goal: euvolemia to mild negative fluid balance; use diuretics to reduce extrapulmonary edema; avoid aggressive fluid resuscitation unless hemodynamically unstable
- Optimize fluid status before increasing FiO₂ or PEEP
6. Corticosteroids
- Rationale: reduce inflammation; may limit fibroproliferative phase
- Evidence: mixed and controversial
- Low-to-moderate dose methylprednisolone (1-2 mg/kg/day) in early ARDS: may improve oxygenation and reduce ventilator days in some trials
- DEXA-ARDS trial (2020): dexamethasone 20 mg/day × 5 days then 10 mg/day × 5 days significantly reduced ventilator days and 60-day mortality in moderate-severe ARDS
- Steroids given late (>2 weeks after onset) may increase mortality - avoid in late fibrotic phase
- Current use: considered in moderate-severe ARDS not improving with standard measures; avoid in septic shock unless already indicated; do not use routinely
7. Rescue/Salvage Therapies (Refractory Hypoxemia)
For ARDS not responding to conventional management:
| Therapy | Evidence | Notes |
|---|---|---|
| Prone positioning | Mortality benefit (PROSEVA) | First-line rescue; should be done early |
| Inhaled nitric oxide (iNO) | Improves oxygenation; no mortality benefit | Selective pulmonary vasodilator; transient use for bridging; rebound hypoxemia on weaning |
| Inhaled prostacyclin (epoprostenol, iloprost) | Improves oxygenation; no mortality benefit | Similar mechanism to iNO; cheaper |
| High-frequency oscillatory ventilation (HFOV) | No mortality benefit (OSCILLATE, OSCAR trials); may increase mortality | Not recommended |
| Recruitment maneuvers | Transient oxygenation improvement; no mortality benefit; may cause harm (ART trial) | Use with caution |
| Extracorporeal CO₂ removal (ECCO₂R) | Allows ultra-low Vt; evidence limited | Investigational |
| VV-ECMO | CESAR trial: benefit when referred to ECMO center; EOLIA trial: no significant benefit (stopped early; ~10% crossover) | For refractory severe ARDS; final option; centers with experience |
Key principle: inhaled NO, prostacyclin, and HFOV improve oxygenation but have not been shown to reduce mortality - use only as bridging strategies.
8. Supportive ICU Care
| Issue | Management |
|---|---|
| Sedation | Minimize; use ABCDEF bundle (Awaken, Breathe, Coordinate, Delirium, Exercise, Family); propofol or dexmedetomidine; avoid prolonged benzodiazepines |
| DVT prophylaxis | Pharmacologic (heparin/LMWH) unless contraindicated; mechanical if pharmacologic contraindicated |
| Stress ulcer prophylaxis | H2 blocker or PPI in mechanically ventilated patients |
| Nutrition | Early enteral nutrition (within 24-48h); goal 12-25 kcal/kg/day in critical illness; avoid overfeeding |
| Glucose control | Target 140-180 mg/dL (tight control <110 increases hypoglycemia risk) |
| VAP prevention | Head-of-bed elevation 30-45°, oral chlorhexidine, subglottic suctioning, daily sedation interruption |
| Anemia | Transfuse for Hb <7 g/dL (TRICC threshold) unless active ischemia |
9. Liberation from Mechanical Ventilation
Daily screening for readiness to wean:
- Underlying cause improving/resolved
- P/F ratio >150-200 on FiO₂ ≤0.4 and PEEP ≤8 cm H₂O
- Hemodynamically stable (minimal/no vasopressors)
- Able to initiate respiratory effort
- Adequate secretion management
Spontaneous Breathing Trial (SBT): 30-120 minutes on T-piece or low-level PSV/CPAP; extubate if tolerated. Failure = tachycardia, tachypnea, hypoxemia, diaphoresis, agitation.
Prognosis and Outcomes
- Overall ICU mortality: 30-45% (varies by severity and cause)
- Mild ARDS: ~27%
- Moderate ARDS: ~32%
- Severe ARDS: ~45%
- Most deaths in ARDS are from multi-organ failure (not hypoxemic respiratory failure per se)
- Survivors: commonly experience long-term impairments:
- Reduced exercise tolerance and lung function (restrictive pattern)
- Cognitive impairment, PTSD, depression (post-intensive care syndrome - PICS)
- Muscle weakness and fatigue (ICU-acquired weakness)
- Quality of life frequently impaired for months to years
Summary: Key Evidence-Based Interventions That Reduce Mortality
| Intervention | Trial | Mortality Benefit |
|---|---|---|
| Low Vt (6 mL/kg PBW) | ARDSNet ARMA (2000) | ↓ 22% absolute mortality |
| Prone positioning (P/F <150) | PROSEVA (2013) | ↓ ~17% absolute mortality |
| Conservative fluid management | FACTT | ↓ Ventilator days (not mortality) |
| Dexamethasone | DEXA-ARDS (2020) | ↓ Ventilator days; ↓ 60-day mortality |
| Treat underlying cause | - | Foundational |
NOT proven to reduce mortality: HFOV, inhaled NO, inhaled prostacyclin, recruitment maneuvers. ECMO remains uncertain (EOLIA).
Sources: Goldman-Cecil Medicine (9780323930345); Murray & Nadel's Respiratory Medicine (9780323655873); Harrison's Internal Medicine 22E (9781265977061); Fishman's Pulmonary Diseases (9781260473940); Sabiston Textbook of Surgery (9780443124341); Mulholland & Greenfield's Surgery (9781975143169); Rosen's Emergency Medicine (9780323757898)
Sarcoidosis, lupus nephritis, approach to a patient with diarrhoea, portal hypertension, acute exacerbation of COPD
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
All five topics are now covered comprehensively. Here is a quick orientation to what was covered:
Summary of All 5 Topics
1. Sarcoidosis
A systemic granulomatous disease of unknown cause driven by a Th1-mediated immune response forming non-caseating granulomas. Affects lungs (90%), skin, eyes, heart, and CNS. Key investigations: ACE level, serum calcium, CXR (bilateral hilar lymphadenopathy), HRCT, tissue biopsy showing non-caseating granulomas. Scadding staging (0-IV) guides prognosis. Treatment: prednisone first-line; hydroxychloroquine/methotrexate for steroid-sparing; anti-TNF for refractory cases. 50-70% spontaneous resolution; cardiac/neurological involvement carries worst prognosis.
2. Lupus Nephritis
Develops in 30-60% of SLE patients. The ISN/RPS classification (Classes I-VI) is central - Class IV diffuse proliferative is most severe. "Full house" immunofluorescence is characteristic. Treatment: induction with MMF or low-dose IV cyclophosphamide + prednisone; maintenance with MMF or azathioprine; hydroxychloroquine for all SLE patients. New agents: belimumab (FDA-approved for LN, BLISS-LN 2020) and voclosporin (AURORA trial). Monitor with anti-dsDNA, C3/C4, urine PCR.
3. Approach to Diarrhoea
Structured around the 4 mechanisms (osmotic, secretory, inflammatory, dysmotility/malabsorptive). Key algorithmic approach: assess hydration → history for duration/alarm features/epidemiology → examine for extra-intestinal signs → stool studies (including calprotectin, culture, PCR, osmotic gap) → blood tests (TTG-IgA for celiac, TFTs, CBC) → endoscopy/imaging if chronic. Never give antimotility agents in dysentery (E. coli O157, Shigella). ORS is the backbone of treatment.
4. Portal Hypertension
Defined as HVPG >5 mmHg; clinically significant ≥10 mmHg; varices/ascites develop at ≥12 mmHg. Mostly caused by cirrhosis. Central pathophysiology: raised portal pressure → splanchnic vasodilatation → reduced effective arterial volume → RAAS/SNS/ADH activation → ascites + hyponatremia + hepatorenal syndrome. Main complications: varices (managed with EVL + terlipressin + antibiotics; TIPS for refractory), ascites (diuretics + LVP + albumin), SBP (cefotaxime + albumin), hepatic encephalopathy (lactulose + rifaximin), hepatorenal syndrome (terlipressin + albumin).
5. Acute Exacerbation of COPD
Defined as acute worsening of respiratory symptoms without another explanation. Triggered mainly by viral/bacterial infection. Key investigations: ABG (pH guides NIV), CXR, ECG, cultures. Treatment in order: controlled O₂ (target SpO₂ 88-92%) → SABA ± SAMA nebulizers → systemic steroids (prednisone 40 mg × 5 days) → antibiotics if purulent sputum/severe → NIV (BiPAP) if pH ≤7.35 with hypercapnia (reduces mortality and intubation rate) → invasive ventilation if NIV fails. Always exclude pneumothorax, PE, and cardiac failure. Discharge on LABDs with pulmonary rehabilitation referral.
This is a shared conversation. Sign in to Orris to start your own chat.