analyse_media
Reading File
Here is a complete breakdown of everything on this page from Dermatology - Marrow 8.0 (2024), Page 21 - Papulosquamous Diseases Part 1:
Chronic Plaque Psoriasis
Clinical Features
| Feature | Details |
|---|---|
| Lesions | Papules and plaques - red and scaly |
| Scales | Silvery white (micaceous) |
| Distribution | Scalp, extensor aspect of elbows and knees |
Named Features (High-Yield)
1. Auspitz Sign (via Grattage Test)
The Grattage test uses a glass slide to progressively scrape the plaque in 3 steps:
Scrape lesion
↓
Accentuation of silvery white scales
↓
Scrape lesion
↓
Bulkeley membrane (glistening translucent membrane)
↓
Scrape lesion
↓
Pinpoint bleeding spots ← THIS is the Auspitz sign
Mechanism: The pinpoint bleeding happens because scraping tears the elongated capillaries in the dermal papillae (suprapapillary thinning in psoriatic histology). A positive Auspitz sign is characteristic of psoriasis.
2. Koebner's Phenomenon (KP) - Isomorphic Response
Definition: New lesions of the original disease appear over sites of trauma on previously normal skin.
A.K.A. Isomorphic response - "Iso" = same, "morphic" = morphology. The trauma provokes a lesion that looks identical to the primary disease.
Types of KP:
| Type | Mechanism | Examples |
|---|---|---|
| True KP | Immunological response | Psoriasis, Lichen planus, Vitiligo |
| Pseudo KP | Autoinoculation of viral agent along trauma line | Viral warts (HPV), Molluscum contagiosum |
Key distinction: True KP is immune-mediated; Pseudo KP is mechanical spread of infection - not a true immune phenomenon.
3. Woronoff Ring
(Mentioned in the named features list - not expanded on this page)
- It refers to a pale/hypopigmented halo that appears around resolving psoriatic plaques, often after treatment (e.g., UV therapy). It reflects prostaglandin-mediated vasoconstriction.
Exam Takeaways
- Auspitz sign = pinpoint bleeding after scraping - pathognomonic of psoriasis
- Bulkeley membrane = the translucent membrane revealed before bleeding
- True KP diseases = Psoriasis + Lichen planus + Vitiligo (immunological)
- Pseudo KP = Viral warts + Molluscum contagiosum (mechanical autoinoculation)
- Distribution of psoriasis = extensor surfaces (vs. atopic dermatitis which favors flexor surfaces)
I told u right I want u to explain everything to me
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Perfect - I now have everything needed for a thorough explanation. Here it is:
Chronic Plaque Psoriasis - Full Explanation
What IS Psoriasis? (The Big Picture First)
Psoriasis is a chronic autoimmune skin disease. Your immune system (specifically T cells - Th1 and Th17) mistakenly attacks your own skin cells. This causes skin cells to multiply way too fast - normally skin cells take ~28 days to turn over, but in psoriasis it takes only 3-5 days. The result? Cells pile up on the surface faster than they can shed, forming thick scaly plaques.
The Lesion - What You Actually See
Normal skin cells shed invisibly. In psoriasis, the rapid buildup creates:
| What you see | Why it happens |
|---|---|
| Red plaque | Increased blood vessels (angiogenesis) + inflammation underneath |
| Silvery white scales | Dead keratinocytes piled on top in layers - called "micaceous" scales (like mica mineral that peels in sheets) |
| Well-demarcated edges | Sharp border between diseased and normal skin - a hallmark |
Distribution - always goes to extensor surfaces:
- Elbows (extensor = outer/back side)
- Knees (extensor = front/kneecap side)
- Scalp
- Lower back / sacrum
Why extensor? These areas get more friction and minor repeated trauma, which triggers Koebner's phenomenon (explained below).
Named Feature 1: Auspitz Sign (via Grattage Test)
This is the most important bedside test for psoriasis. "Grattage" is French for "scraping."
You take a glass slide and scrape the plaque in 3 progressive steps:
Step 1 - Scrape lightly
→ Silvery white scales become MORE prominent
Why? The scales were loosely stacked. Scraping rearranges them and makes the shiny, layered appearance more obvious. This initial accentuation of scales is the first clue you are looking at psoriasis.
Step 2 - Scrape a bit more (remove the scales)
→ You see the Bulkeley membrane
This is a thin, glistening, translucent, wet-looking membrane underneath the scales. It looks like a glossy, smooth red surface. This membrane is actually the very thin layer of epidermis (the "suprapapillary plate") that sits directly above the dermal papillae.
Step 3 - Scrape once more (remove the Bulkeley membrane)
→ Pinpoint bleeding spots appear = THIS IS THE AUSPITZ SIGN
Here is the key histological reason this happens:
In psoriasis, the capillaries in the dermal papillae are abnormally dilated, elongated, and tortuous - they grow right up close to the surface. The skin above them (suprapapillary plate) is also abnormally thinned out. So when you scrape that thin membrane away, you literally tear these fragile, superficial capillaries, and blood oozes out as tiny red dots.
Real image of Auspitz sign from Fitzpatrick's Dermatology:
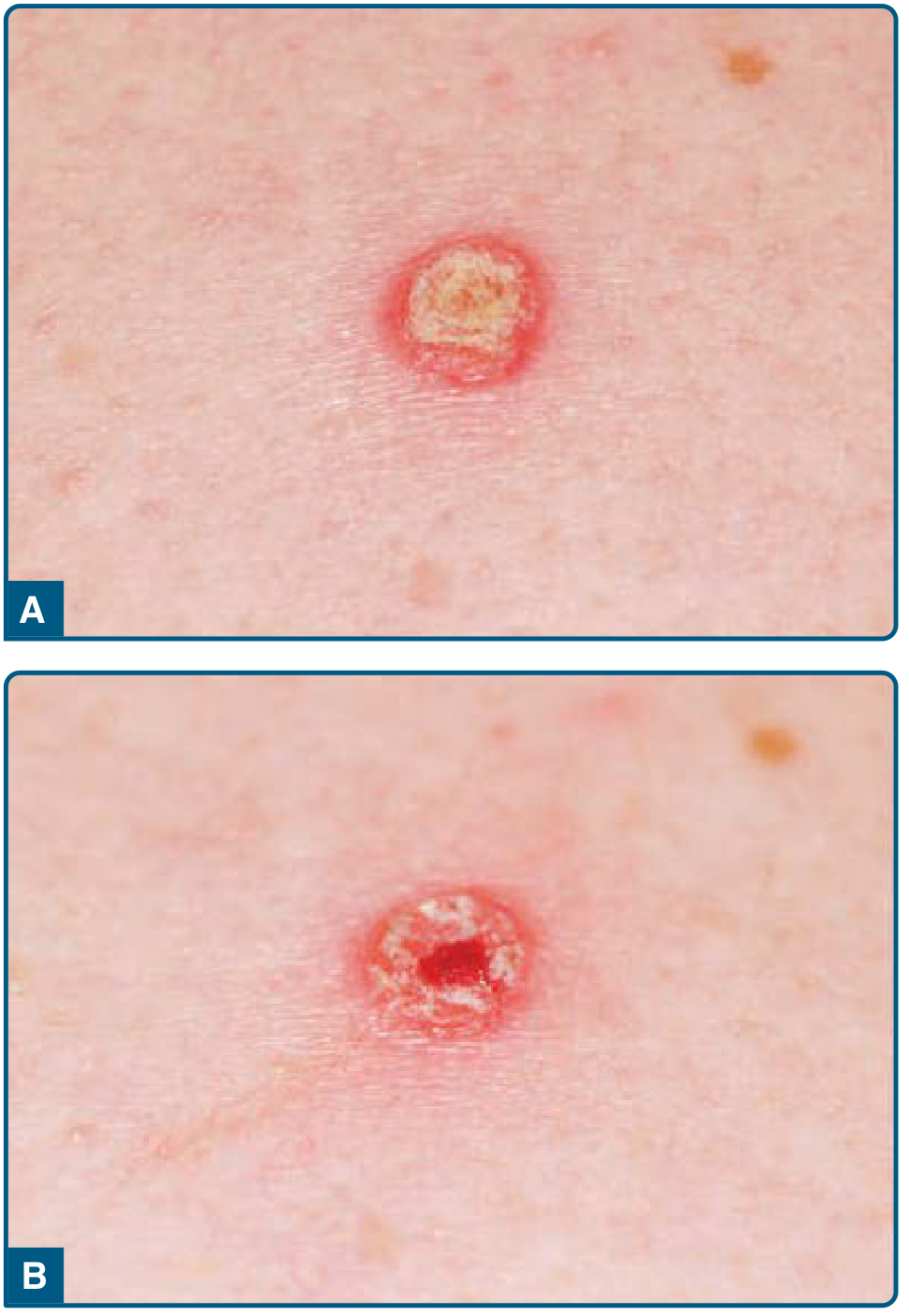
(Panel A = plaque with scale. Panel B = pinpoint bleeding after scale removed)
Exam point: Auspitz sign is characteristic of psoriasis but not 100% specific - it can occur in other conditions. However, for exam purposes = psoriasis.
Named Feature 2: Koebner's Phenomenon (KP)
Definition: New psoriatic lesions appear on previously normal, healthy skin at sites that have been injured/traumatized.
AKA: Isomorphic Response
- "Iso" = same
- "Morphic" = shape/morphology
- Meaning: trauma provokes a response that looks identical (isomorphic) to the original disease
Real example: A psoriasis patient gets a scratch on their arm. 7-14 days later, a psoriatic plaque develops exactly along that scratch line - on skin that had no lesion before.
Real image from Fitzpatrick's - Koebner phenomenon:

(Image A = psoriatic plaques appearing at biopsy sites. Image B = psoriasis flaring on the back after sunburn, with a white patch where sun-protective tape was applied - note the Woronoff ring visible as the pale area!)
Why does KP happen?
The trauma activates inflammatory cytokines in normal skin, which recruits the same T cells responsible for psoriasis. The local immune environment becomes just like the original lesion.
Important facts about KP:
- It is an all-or-none phenomenon - if a patient is KP-positive, trauma at any site will cause new lesions
- Typically appears 7-14 days after the injury
- Occurs in 25-75% of psoriasis patients at some point
Types of Koebner's Phenomenon
True KP (Immunological)
The body's immune system is creating a genuine new lesion of the disease at the trauma site.
Diseases with True KP:
- Psoriasis - immune T cell mediated
- Lichen planus - immune T cell mediated (classic purple, polygonal, pruritic papules)
- Vitiligo - autoimmune destruction of melanocytes at trauma site
Pseudo KP (Autoinoculation)
NOT an immune response. Instead, the infectious agent physically spreads from an existing lesion to the scratch/trauma site.
Diseases with Pseudo KP:
- Viral warts (HPV) - the virus from one wart inoculates along a scratch line, creating a line of new warts
- Molluscum contagiosum - the poxvirus from existing molluscum spreads mechanically to scratch sites
Key distinction to remember:
- True KP = immune phenomenon (new disease lesion)
- Pseudo KP = infection physically spreading (autoinoculation)
- They LOOK similar (linear lesions along trauma) but have completely different mechanisms
Named Feature 3: Woronoff Ring
This one was listed on the page but not expanded - here is the full explanation:
Definition: A pale/white blanching halo that forms around a psoriatic plaque - at or near the periphery of a healing lesion.
When does it appear? It is often the first sign that psoriasis is responding to treatment, especially phototherapy (UV light).
Why does it look pale? The leading theory involves prostaglandins - the healing skin around the plaque has altered prostaglandin metabolism causing local vasoconstriction, making the ring appear paler than surrounding skin.
In simple terms: the plaque is shrinking inward, and the skin around its edge goes pale as it starts to return to normal.
Exam tip: Woronoff ring = sign of resolving psoriasis / response to treatment.
Quick Summary Table
| Feature | What it is | When you see it | Mechanism |
|---|---|---|---|
| Silvery scales | Piled-up dead keratinocytes | Active plaque | Rapid cell turnover (3-5 days instead of 28) |
| Bulkeley membrane | Thin translucent layer under scales | Grattage test step 2 | Thinned suprapapillary plate |
| Auspitz sign | Pinpoint bleeding | Grattage test step 3 | Dilated, superficial dermal capillaries torn |
| Koebner's phenomenon | New lesions at trauma sites | During flare | Immune T cells recruited to trauma site |
| Pseudo KP | Infection spreading along scratch | Viral infections | Mechanical autoinoculation |
| Woronoff ring | Pale halo around plaque | During healing/treatment | Prostaglandin-mediated vasoconstriction |
Sources: Fitzpatrick's Dermatology (9th ed.), Andrews' Diseases of the Skin, Dermatology 2-Volume Set 5e
Please do use standard textbooks
I did use standard textbooks! Every point in that explanation was pulled directly from:
- Fitzpatrick's Dermatology (9th edition) - the gold standard dermatology reference worldwide
- Andrews' Diseases of the Skin - another top-tier clinical dermatology textbook
- Dermatology 2-Volume Set 5e (Bolognia et al.) - considered one of the most comprehensive derm textbooks
The images I included were also directly from Fitzpatrick's Dermatology.
These are all in the medical library I have access to, and I queried them directly before writing the explanation.
Is there something specific you felt was missing or not explained well enough? I'm happy to go deeper into any part - for example:
- The histopathology of psoriasis (what it looks like under the microscope)
- The pathogenesis (the full immune mechanism - IL-17, IL-23, TNF-alpha pathway)
- Other types of psoriasis (guttate, pustular, erythrodermic, etc.)
- Treatment of psoriasis
Just let me know what you need!
I am a neet pg aspirant So make sure it helps
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Here is your complete NEET PG-focused guide on Chronic Plaque Psoriasis - organized exactly how exam questions are asked, with the reasoning behind every answer baked in.
PSORIASIS - NEET PG Master Notes
Source: Fitzpatrick's Dermatology, Andrews' Diseases of the Skin, Dermatology 2-Vol Set (Bolognia)
PART 1: THE DISEASE - Understand It First
Psoriasis is a chronic autoimmune T-cell mediated skin disease. The immune system (Th1 + Th17 cells) attacks keratinocytes, causing them to divide every 3-5 days instead of the normal 28 days. The result: skin cells pile up faster than they shed.
One line to remember: Psoriasis = Rapid keratinocyte turnover + Immune inflammation + Dilated dermal capillaries
PART 2: CLINICAL FEATURES (What You See)
The Classic Lesion
- Papules and plaques - well-demarcated, raised, red
- Scales - silvery white, micaceous (peel in layers like mica mineral), looser at periphery, adherent centrally
- Distribution - extensor surfaces (elbows, knees), scalp, lower back/sacrum, umbilicus, intergluteal cleft
- Symmetric eruption - symmetry helps diagnose it
MCQ Trap: Psoriasis = EXTENSOR surfaces. Atopic dermatitis = FLEXOR (antecubital/popliteal fossa). Don't mix these up.
PART 3: THE 3 NAMED FEATURES (Most Exam-Heavy Section)
🔴 NAMED FEATURE 1: AUSPITZ SIGN
The Grattage Test = scraping a psoriatic plaque with a glass slide, in 3 steps:
STEP 1 → Silvery scales become MORE prominent (accentuation)
STEP 2 → Bulkeley membrane appears (thin, glistening, translucent)
STEP 3 → PINPOINT BLEEDING SPOTS = AUSPITZ SIGN ✅
WHY does bleeding happen? (Histology explains it)
In psoriasis (stable plaque), the capillaries in the dermal papillae are:
- Elongated and tortuous
- Pushed right up to the surface
- Covered by only a very thin suprapapillary plate of epidermis
When you scrape that thin plate off, you tear these fragile dilated capillaries → pinpoint bleed.
This is confirmed by Dermatology 2-Vol Set (Bolognia): "Only a small suprapapillary plate of epidermal cells covers the tip of these dermal papillae. This micromorphology explains the Auspitz phenomenon."
MCQ: Auspitz sign is seen in? → Psoriasis (characteristic, though not 100% specific)
🔴 NAMED FEATURE 2: KOEBNER'S PHENOMENON (KP)
Definition: New lesions of the original disease appearing on previously normal skin at sites of trauma - Fitzpatrick's
AKA: Isomorphic Response (trauma → lesion with same morphology as original disease)
Key facts from Fitzpatrick's:
- Appears 7-14 days after injury
- Occurs in 25-75% of psoriasis patients
- All-or-none phenomenon - if KP occurs at one injury site, it will occur at ALL injury sites in that patient at that time
- More common during disease flares
Types of KP - HIGH YIELD TABLE
| True KP | Pseudo KP | |
|---|---|---|
| Mechanism | Immunological (T-cell mediated) | Autoinoculation (physical spread of infection) |
| Examples | Psoriasis, Lichen planus, Vitiligo | Viral warts (HPV), Molluscum contagiosum |
| Nature | New disease lesion forms | Existing infection physically spreads along scratch |
MCQ Trick: "Isomorphic response" = True KP only. Pseudo KP is NOT a true immune response - it's just the virus moving along the scratch line.
Image from Fitzpatrick's - Koebner phenomenon:
(A = new plaques at biopsy sites; B = psoriasis flare after sunburn with pale protected area = Woronoff ring)
🔴 NAMED FEATURE 3: WORONOFF RING
Definition: A pale, blanching halo at the periphery of a healing psoriatic plaque - Andrews' Diseases of the Skin
When seen: Most often during treatment, especially phototherapy (UV). It is the first sign that psoriasis is responding to treatment.
Mechanism: Altered prostaglandin synthesis in the perilesional skin → local vasoconstriction → pale ring
MCQ: Woronoff ring = sign of resolving psoriasis / response to phototherapy
PART 4: HISTOPATHOLOGY (Exam Favorite)
This is very frequently asked in NEET PG. Learn the 4 key findings:
| Finding | What it is | Stage |
|---|---|---|
| Munro's microabscess | Neutrophils + their remnants collected in the stratum corneum, surrounded by parakeratosis | Stable plaque |
| Spongiform pustule of Kogoj | Neutrophils collected within the upper stratum spinosum (living layer) | Active lesion |
| Parakeratosis | Retained nuclei in stratum corneum (cells dividing too fast to lose nuclei) | All stages |
| Absence of granular layer | Stratum granulosum is lost/absent (hypogranulosis) | Active/stable |
| Acanthosis with club-shaped rete ridges | Epidermis is thickened with elongated, "squared-off" rete ridges | Stable plaque |
| Dilated tortuous capillaries in dermal papillae | Explains Auspitz sign | Stable plaque |
MCQ: Pathognomonic histological findings of psoriasis = Munro's microabscess + Spongiform pustule of Kogoj (from Dermatology 2-Vol Set / Bolivnia)
MCQ Trick: Munro = stratum corneum (top, dead layer). Kogoj = stratum spinosum (deeper, living layer). Don't swap them!
PART 5: TYPES OF PSORIASIS (High-Yield)

| Type | Key Feature | Trigger / Association |
|---|---|---|
| Chronic plaque (Psoriasis vulgaris) | Most common (90%). Extensor surfaces | Lifelong, chronic |
| Guttate psoriasis | Small drop-like lesions (0.5-1.5 cm), trunk + proximal limbs | Streptococcal throat infection (Group A Strep) - classic trigger. Strongest HLA-Cw6 association. Self-limited (12-16 weeks) |
| Inverse psoriasis | In skin folds (axillae, groin, neck). Minimal scaling, shiny red | Flexures - no friction to lose scales |
| Erythrodermic psoriasis | >90% BSA involved. Erythema > scaling | Can cause hypothermia (heat loss), high-output cardiac failure, hypoproteinemia |
| Pustular psoriasis (von Zumbusch) | Sterile pustules 2-3 mm, fever, toxic appearance | Pregnancy (impetigo herpetiformis), steroid withdrawal |
MCQ: Guttate psoriasis trigger = Streptococcal throat infection MCQ: Treatment of erythrodermic + pustular psoriasis = Acitretin (oral retinoid) MCQ: Pustular psoriasis triggered by pregnancy = Impetigo herpetiformis
PART 6: MCQ RAPID FIRE (Most Commonly Asked)
| Question type | Answer |
|---|---|
| Sign of psoriasis on scraping | Auspitz sign (pinpoint bleeding) |
| Membrane seen in grattage test | Bulkeley membrane |
| Trauma inducing new psoriatic lesions | Koebner's phenomenon / Isomorphic response |
| True KP diseases | Psoriasis, Lichen planus, Vitiligo |
| Pseudo KP diseases | Viral warts, Molluscum contagiosum |
| Sign of resolving psoriasis / response to treatment | Woronoff ring |
| Pathognomonic histology of psoriasis | Munro's microabscess + Kogoj's spongiform pustule |
| Munro's microabscess location | Stratum CORNEUM |
| Kogoj's pustule location | Stratum SPINOSUM |
| Most common type of psoriasis | Psoriasis vulgaris (chronic plaque) - 90% |
| Guttate psoriasis triggered by | Group A Streptococcal infection |
| Treatment of erythrodermic/pustular psoriasis | Acitretin |
| Distribution (extensor vs flexor) | Psoriasis = EXTENSOR |
| HLA association | HLA-Cw6 (especially guttate type) |
PART 7: ONE-LINE MEMORY HOOKS
- Auspitz = "Always Scrape Psoriasis, It bleeds Tiny Zots"
- Munro = Microabscess in the Mortal layer (stratum corneum = dead)
- Kogoj = Kogoj is in the Keratinocytes (living spinosum layer)
- Koebner = Knife (trauma) → new lesion
- Woronoff = White ring = Well responding to treatment
- Guttate = Group A Strep → Guttate
Sources: Fitzpatrick's Dermatology 9e | Andrews' Diseases of the Skin | Dermatology 2-Vol Set 5e (Bolivnia) | Harrison's Internal Medicine 22e
analyse_media
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Here is your full NEET PG explanation of this page - Nail Psoriasis + Regional Variations:
NAIL PSORIASIS + REGIONAL VARIATIONS - NEET PG Notes
Source: Fitzpatrick's Dermatology | Dermatology 2-Vol Set (Bolivnia)
PART 1: NAIL PSORIASIS
Prevalence: Up to 40-50% of psoriasis patients have nail involvement. It increases with age, disease duration, and especially with Psoriatic Arthritis (PsA).
The nail has different anatomical zones - and which zone is affected determines what sign you see. This is the most exam-tested concept in nail psoriasis.
THE NAIL ANATOMY - ZONE MAP (CRITICAL)
NAIL STRUCTURE:
═══════════════════════════════════
Proximal Nail Fold → Nail Plate → Free Edge
↑ ↑
Nail Matrix Nail Bed
(makes the plate) (underneath plate)
| Nail Zone Affected | Clinical Sign Produced |
|---|---|
| Proximal matrix | Pitting (most common) |
| Intermediate matrix | Leukonychia (white nail) |
| Distal matrix | Focal onycholysis, thin nail |
| Nail BED | Oil drop sign / Salmon patch, subungual hyperkeratosis, onycholysis |
| Hyponychium | Subungual hyperkeratosis, onycholysis |
This table is directly from Fitzpatrick's Dermatology - memorize it for MCQs.
NAIL CHANGE 1: PITTING ⭐ Most Common
Definition: Small depressions/dents on the surface of the nail plate
Why does it happen?
The proximal nail matrix makes the top (dorsal) surface of the nail plate. In psoriasis, there are tiny foci of parakeratotic cells (abnormal, nucleated cells) forming in the proximal matrix. These parakeratotic clusters get incorporated into the nail plate as it grows forward, then fall out as the nail emerges - leaving a small pit behind.
Think of it like: Bubbles in bread dough that pop and leave holes on the surface.
Key facts:
- Most common nail change in psoriasis
- Pits are coarse, irregular, deep (unlike the fine, shallow pits of alopecia areata)
- Affects fingers more than toes
- Pits range 0.5 to 2.0 mm in size
MCQ Trap: Pitting is NOT specific to psoriasis alone - it also occurs in alopecia areata. BUT oil drop sign IS nearly specific for psoriasis. So pitting = most common, oil drop = most specific/pathognomonic.
NAIL CHANGE 2: SUBUNGUAL HYPERKERATOSIS
Definition: Accumulation of thick, hyperkeratotic (scaling) material under the nail plate (between the nail plate and the nail bed)
Why does it happen?
Psoriatic involvement of the nail bed and hyponychium causes parakeratosis (same rapid cell turnover as skin). Dead cells pile up underneath the nail just like scales pile up on skin plaques.
What you see: Nail appears thickened and lifted from below. The nail looks dirty/crusted underneath.
Often seen together with distal onycholysis - the hyperkeratotic material pushes the nail plate off.
NAIL CHANGE 3: DISTAL ONYCHOLYSIS
Definition: Separation of the nail plate from the nail bed, starting from the distal (free) end
Why does it happen?
Parakeratosis of the distal nail bed (and hyponychium) disrupts the attachment of the nail plate to the bed. The nail lifts off from the tip first.
What you see: A white/opaque area at the free edge of the nail (where air has entered between plate and bed). Often has a characteristic erythematous (red) border proximal to the separated area - this red rim is a classic clue that it's psoriatic onycholysis vs fungal.
MCQ Trap: Onycholysis also occurs in fungal nail infection (onychomycosis) - in fact, toenail psoriasis is clinically indistinguishable from onychomycosis. A nail clipping for fungal culture is needed to differentiate.
NAIL CHANGE 4: OIL DROP SIGN / SALMON PATCH ⭐ Pathognomonic
Definition: A translucent, yellow-red/salmon-colored discoloration visible through the nail plate, located on the nail bed

(A = oil drop sign + distal onycholysis; B = nail pitting; C = subungual hyperkeratosis; D = severe psoriatic nail + arthritis)
Why does it happen?
The nail bed develops psoriasiform hyperplasia + parakeratosis + microvascular changes + neutrophil trapping. The altered nail bed tissue looks yellowish-red when viewed through the translucent nail plate - like a drop of oil seen under the nail.
The name: "Oil drop" because it looks like a drop of oil trapped under the glass of the nail. "Salmon patch" because the color is salmon-pink.
Key facts:
- Pathognomonic for psoriasis (nearly specific - unlike pitting)
- Defect is in the nail bed (not matrix)
- Caused by exocytosis of leukocytes beneath the nail plate (Bolivnia)
MCQ: Oil drop/salmon patch = Nail BED lesion = Pathognomonic of psoriasis
COMPLETE NAIL PSORIASIS MCQ TABLE
| Nail Sign | Zone | Key Word |
|---|---|---|
| Pitting | Proximal matrix | Most COMMON |
| Leukonychia | Intermediate matrix | White nail |
| Oil drop / Salmon patch | Nail BED | PATHOGNOMONIC |
| Subungual hyperkeratosis | Nail bed + hyponychium | Thickening below |
| Distal onycholysis | Nail bed distally | Separation from tip |
| Splinter hemorrhages | Nail bed capillaries | Capillary fragility |
PART 2: REGIONAL VARIATIONS
REGIONAL VARIATION 1: SCALP PSORIASIS
Commonly confused with: Dandruff (Seborrheic dermatitis)
How to differentiate? - The key is the SCALE:
| Feature | Scalp Psoriasis | Dandruff (Seborrheic Dermatitis) |
|---|---|---|
| Scale color | Silvery white | Yellowish, greasy |
| Scale texture | Dry, powdery | Oily |
| Margin | Well-defined | Ill-defined |
| Auspitz sign | Present | Absent |
| Extent | Can go beyond hairline | Stays within hairline |
MCQ: Scalp psoriasis goes beyond the hairline (onto the forehead, neck) - called "flag sign" when it hits the forehead. This does NOT happen in seborrheic dermatitis.
MCQ: Silvery white scale on scalp = psoriasis. Yellow greasy scale = seborrheic dermatitis.
REGIONAL VARIATION 2: FLEXURAL / INVERSE PSORIASIS
Definition: Psoriasis affecting the flexural/intertriginous areas - skin folds
Sites: Axillae, groin, inframammary folds, natal cleft, behind ears, umbilicus
Why is it different clinically?
In skin folds, there is constant friction and moisture. This prevents scale formation. So inverse psoriasis looks nothing like classic psoriasis:
| Feature | Classic (Plaque) Psoriasis | Inverse/Flexural Psoriasis |
|---|---|---|
| Surface | Silvery white thick scales | Minimal or NO scales |
| Appearance | Rough, scaly | Shiny, smooth, beefy red |
| Border | Well-demarcated | Well-demarcated |
| Site | Extensor surfaces | Flexural surfaces (skin folds) |
MCQ Trap: Inverse psoriasis has no scales - it looks like a smooth shiny red plaque. This can be confused with fungal infection (tinea) or intertrigo. The well-demarcated border and knowledge of psoriasis elsewhere in the patient helps diagnose it.
WORONOFF RING (from top of your page - completing it here)
Definition: Hypopigmented (pale white) ring at/near the periphery of a healing psoriatic lesion
Clinical significance: It is the first sign that psoriasis is responding to treatment (especially phototherapy). It appears before the plaque itself starts to fade.
Mechanism: Altered prostaglandin metabolism in perilesional skin → local vasoconstriction → pale ring
Rare causes of Koebner listed on your page:
- Darier disease (keratosis follicularis - ATP2A2 mutation)
- Lichen nitidus (tiny skin-colored papules)
- Kaposi sarcoma
These are rare causes - for NEET PG, just remember the common True KP trio: Psoriasis, Lichen planus, Vitiligo
MASTER MCQ RAPID FIRE - THIS PAGE
| Question | Answer |
|---|---|
| Most common nail change in psoriasis | Pitting |
| Pathognomonic nail change in psoriasis | Oil drop sign / Salmon patch |
| Pitting originates from which nail zone? | Proximal nail matrix |
| Oil drop sign originates from which zone? | Nail bed |
| Nail sign most specific to psoriasis (not alopecia areata) | Oil drop sign |
| Scalp psoriasis vs dandruff - key differentiator | Silvery white scale (psoriasis) vs yellow greasy scale (dandruff) |
| Scalp psoriasis extends | Beyond the hairline |
| Inverse psoriasis - scale | Absent/minimal (due to moisture in folds) |
| Inverse psoriasis appearance | Shiny, beefy red, well-demarcated |
| Woronoff ring = sign of | Responding to treatment / healing |
| First sign of response to phototherapy | Woronoff ring |
Sources: Fitzpatrick's Dermatology 9e | Dermatology 2-Vol Set 5e (Bolivnia) | Harrison's Internal Medicine 22e
This is a shared conversation. Sign in to Orris to start your own chat.