Progressive dementia
Reading File
Asking for Preferences
Finding Sources
Searching the Web
progressive dementia causes classification overview medical
Searching PubMed
"dementia" AND "etiology" AND "classification"
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Progressive Dementia — Overview & Causes
Definition
Dementia is a syndrome of acquired, progressive decline in two or more cognitive domains (memory, language, executive function, visuospatial, behavior/personality) severe enough to impair daily functioning. "Progressive" distinguishes it from static deficits (e.g., post-stroke) — the underlying disease continues to destroy neurons over time.
The Four Major Causes (Exam Core)
Over 35 million people worldwide have dementia. While countless causes exist, four account for the vast majority of cases:
| Type | Prevalence | Core Pathology | Key Clinical Features |
|---|---|---|---|
| Alzheimer Disease (AD) | ~60–70% | Aβ plaques + neurofibrillary tau tangles + neuronal loss | Short-term memory loss first, temporal/parietal atrophy, APOE ε4 risk |
| Vascular Dementia | ~20% | Cerebrovascular disease (infarcts, white-matter changes, microbleeds) | Stepwise decline, stroke risk factors, subcortical pattern |
| Lewy Body Dementias (DLB/PDD) | ~10–15% | α-synuclein aggregates (Lewy bodies/neurites) | Fluctuating cognition, visual hallucinations, spontaneous parkinsonism, REM sleep disorder |
| Frontotemporal Dementia (FTD) | Varies; commonest in <65 yo | TDP-43, tau, or FUS proteinopathy | Behavioral/personality change, disinhibition or apathy; relatively preserved memory early |
— Stahl's Essential Psychopharmacology, Table 12-2; Bradley and Daroff's Neurology, Ch. 95
Alzheimer Disease (AD) — High-Yield Details
Pathological hallmarks (require autopsy for definitive diagnosis):
- Amyloid-beta (Aβ) plaques — extracellular aggregation
- Neurofibrillary tangles — intracellular hyperphosphorylated tau
- Profound neuronal loss — visible to the naked eye at autopsy

Neuronal loss is so profound in AD it is visible macroscopically. — Stahl's Essential Psychopharmacology, Fig. 12-3
Neuroimaging progression:
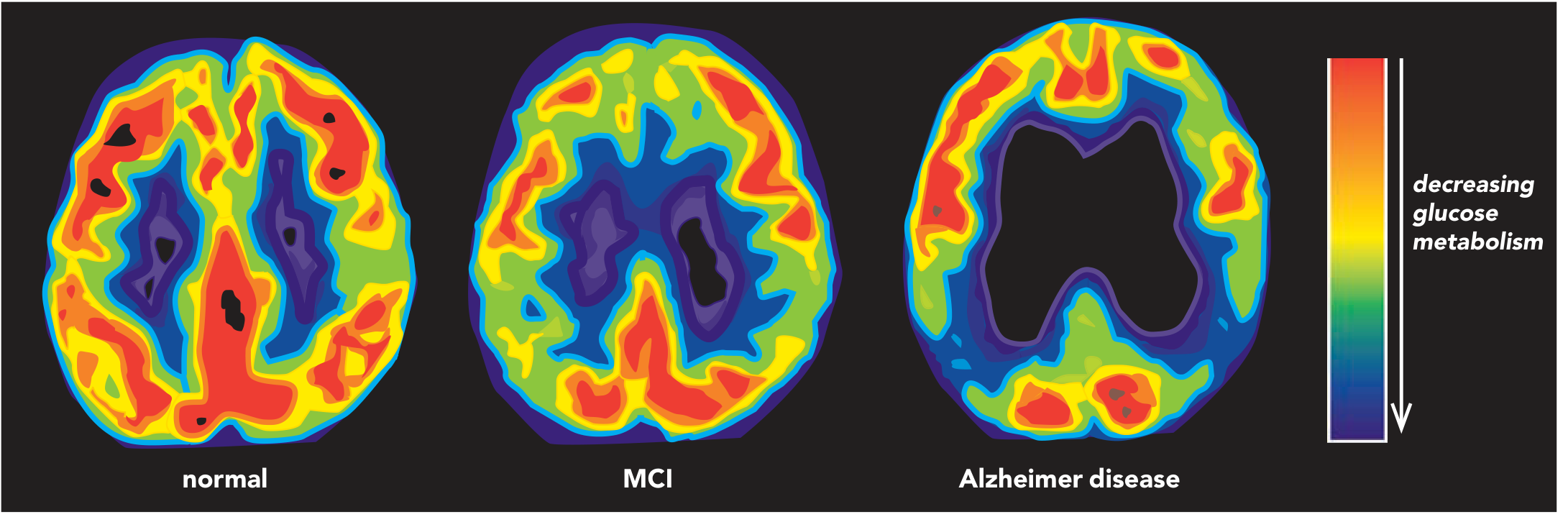
- FDG-PET: temporo-parietal hypometabolism → worsens with progression
- MRI: medial temporal lobe atrophy, hippocampal volume loss (20–30% even in mild AD), ventricular enlargement
- Key cholinergic deficit: NBM (nucleus basalis of Meynert) degeneration → loss of cortical cholinergic input
Vascular Dementia
Essentially a neurological manifestation of cardiovascular disease. Risk factors mirror those for peripheral vascular disease: hypertension, smoking, hypercholesterolemia, diabetes, heart disease.
- ~30% of stroke patients develop post-stroke cognitive impairment
- FDG-PET shows sensorimotor/subcortical hypometabolism (contrast: posterior pattern in AD)
- MRI shows white-matter hyperintensities
- AD and vascular dementia frequently co-exist (~mixed dementia); Aβ deposition into vessel walls may worsen vascular integrity and vice versa
Lewy Body Dementias (DLB/PDD)
Diagnostic criteria for DLB (must have dementia + ≥2 core features):
| Core Features | Suggestive Features |
|---|---|
| Fluctuating attention/concentration | REM sleep behavior disorder |
| Recurrent well-formed visual hallucinations | Severe neuroleptic sensitivity ⚠️ |
| Spontaneous parkinsonism | Low dopamine transporter uptake on SPECT/PET |
High-yield exam point: Lewy body dementia patients have severe neuroleptic sensitivity — antipsychotics can cause life-threatening reactions.
Frontotemporal Dementia (FTD)
- Most common neurodegenerative dementia in patients <65 years old
- Presents with progressive behavioral/personality change (apathy, disinhibition, loss of social conduct) or primary progressive aphasia — episodic memory relatively preserved early
- Strongly associated with motor neuron disease (FTD-MND)
- FDG-PET: frontotemporal hypometabolism
Non-Degenerative (Potentially Reversible) Causes — MUST KNOW
Always rule out reversible causes before labeling a patient with irreversible dementia.
Toxic/Metabolic
- B12 deficiency, thiamine (Wernicke), niacin (pellagra), vitamin E deficiency
- Hypothyroidism (commonest reversible endocrine cause)
- Liver disease (hepatic encephalopathy), renal disease
- Heavy metal toxicity, drugs/medications, carbon monoxide poisoning
Structural
- Normal pressure hydrocephalus (NPH): classic triad — wet, wobbly, wacky (incontinence + gait apraxia + dementia); Evans index >0.30; treatable with VP shunt
- Primary/metastatic CNS tumors, chronic subdural hematoma
Infectious
- Neurosyphilis, HIV/AIDS-associated dementia
- Chronic meningitis, Whipple disease, CNS tuberculosis, PML
- Prion disease (CJD) — rapidly progressive; most common cause of RPD overall (~75% of RPD cases at UCSF)
Autoimmune/Inflammatory
- Limbic encephalitis (paraneoplastic or autoimmune — anti-NMDA-R, anti-LGI1, etc.)
- SLE, Sjögren syndrome — neuropsychiatric symptoms in up to 90% of SLE
- Multiple sclerosis, sarcoidosis, Behçet disease
Neoplastic
- Paraneoplastic encephalopathy (cancer-associated)
- Lymphoma, slow-growing tumors (meningioma, pituitary tumors)
Rapidly Progressive Dementia (RPD)
A high-yield subtype — onset over weeks to months (up to 1–2 years):
| Cause | % at UCSF RPD referral center |
|---|---|
| Prion disorders | ~75% |
| Neurodegenerative | ~15% |
| Autoimmune/paraneoplastic | ~8% |
| Infectious, neoplastic | <5% |
— Bradley and Daroff's Neurology, Ch. 95
Key RPD features to look for: hallucinations, cortical visual loss, periodic epileptiform discharges on EEG (seen in CJD), normal CSF white cell count + elevated 14-3-3 protein.
Young-Onset Dementia (<45 years)
At Mayo Clinic, the distribution was:
- Neurodegenerative (31%) — FTD and Huntington disease most common
- Autoimmune/inflammatory (21%)
- Metabolic (11%)
- Unknown (19%)
Inherited causes to know: Wilson disease, Huntington disease, leukodystrophies (metachromatic leukodystrophy, adrenoleukodystrophy), Niemann-Pick, Gaucher disease, neuronal ceroid lipofuscinoses.
Differential Diagnosis Snapshot
| Feature | AD | Vascular | DLB | FTD |
|---|---|---|---|---|
| First symptom | Short-term memory | Variable/stepwise | Fluctuating cognition | Behavior/personality |
| Memory impairment | Prominent early | Verbal memory better preserved | Less severe | Relatively spared early |
| Hallucinations | Late | Uncommon | Visual, early | Uncommon |
| Motor signs | Late | Focal deficits | Parkinsonism early | MND in some |
| MRI | Medial temporal atrophy | WM hyperintensities | Medial temporal atrophy | Frontal/temporal atrophy |
| FDG-PET | Temporo-parietal ↓ | Fronto-subcortical ↓ | Parieto-occipital ↓ | Frontotemporal ↓ |
— Stahl's Essential Psychopharmacology, Tables 12-2 & 12-3
Key Pharmacotherapy Principles
- Cholinesterase inhibitors (donepezil, rivastigmine, galantamine): for mild–moderate AD; reduce ACh breakdown → modest symptomatic improvement. None halt neurodegeneration.
- Memantine: NMDA antagonist, protects against excitotoxic glutamate; used in moderate–severe AD; can combine with donepezil.
- Avoid anticholinergic drugs in all dementia patients.
- Avoid antipsychotics in DLB — can cause severe/fatal reactions.
Sources: Stahl's Essential Psychopharmacology, Ch. 12; Bradley and Daroff's Neurology in Clinical Practice, Ch. 95; Kaplan & Sadock's Synopsis of Psychiatry
This is a shared conversation. Sign in to Orris to start your own chat.